Summary
Rev Bras Ginecol Obstet. 2023;45(9):511-516
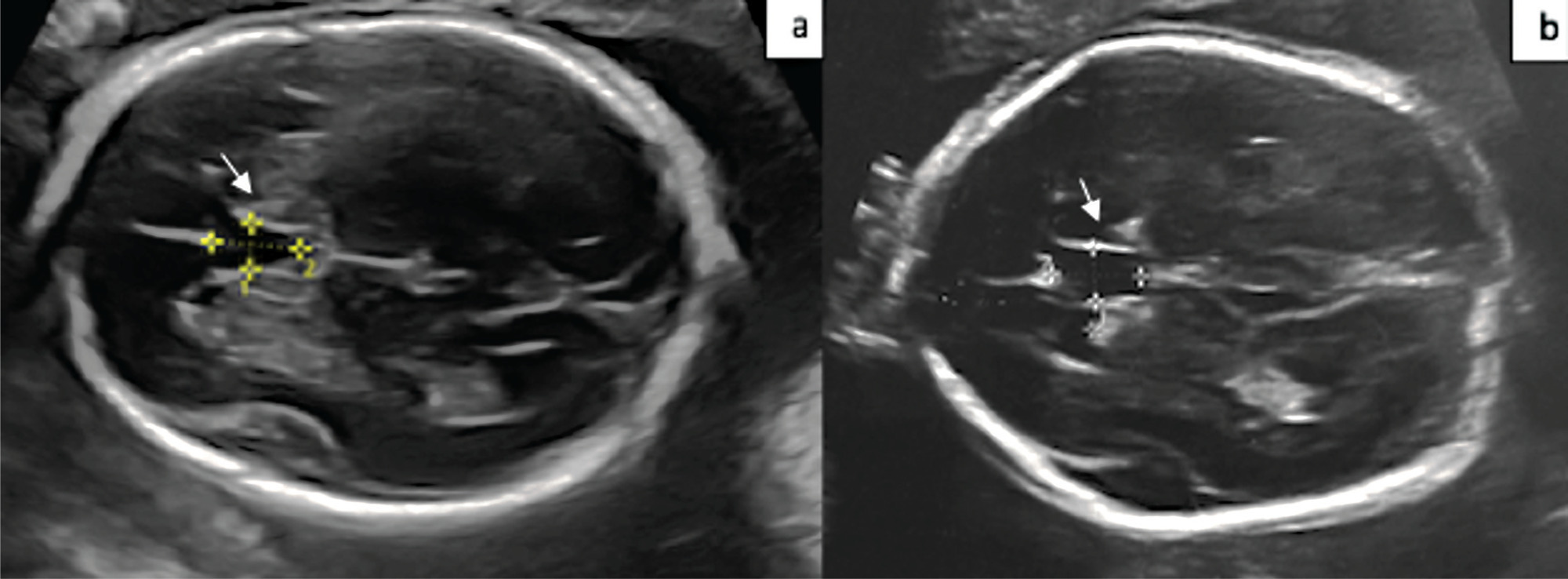
The aim of the present study is to compare the cavum septum pellucidi (CSP) z-score in euploid and aneuploid fetuses and to investigate the performance of the CSP width/length and CSP width/biparietal diameter (BPD) ratios as a diagnostic marker in aneuploidy.
A total of 54 patients, 20 aneuploid and 35 euploid fetuses, between 18 and 37 weeks of gestation, were included in this retrospective study. The CSP width z-score was compared between the two groups. Receiver operating characteristic (ROC) curves were calculated for the CSP width/length and CSP width/BPD ratios to predict aneuploidy.
The median CSP width was 4.8 mm (range, 1.8 to 8.5 mm) in the euploid group, and 5.4 mm (range 3.1 to 8.4 mm) in the aneuploid group. Cavum septum pellucidi width z-score, CSP width/length ratio, and CSP width/BPD ratio were significantly higher in fetuses with aneuploidy than in fetuses with normal karyotype (p = 0.001; p = 0.013; p = 0.028). In the ROC analysis, the CSP width/length ratio had the optimal cutoff value of 0.59, with 72.0% sensitivity and 58.0% specificity, and for the CSP width/BPD ratio, the cutoff value was 0.081 with 83.0% sensitivity and 61.0% specificity for detection of aneuploidy.
CSP width z-score was found to be increased in aneuploid fetuses. The CSP width /BPD ratio can be used as a new marker for predicting aneuploidy.
Summary
Rev Bras Ginecol Obstet. 2023;45(9):511-516
The aim of the present study is to compare the cavum septum pellucidi (CSP) z-score in euploid and aneuploid fetuses and to investigate the performance of the CSP width/length and CSP width/biparietal diameter (BPD) ratios as a diagnostic marker in aneuploidy.
A total of 54 patients, 20 aneuploid and 35 euploid fetuses, between 18 and 37 weeks of gestation, were included in this retrospective study. The CSP width z-score was compared between the two groups. Receiver operating characteristic (ROC) curves were calculated for the CSP width/length and CSP width/BPD ratios to predict aneuploidy.
The median CSP width was 4.8 mm (range, 1.8 to 8.5 mm) in the euploid group, and 5.4 mm (range 3.1 to 8.4 mm) in the aneuploid group. Cavum septum pellucidi width z-score, CSP width/length ratio, and CSP width/BPD ratio were significantly higher in fetuses with aneuploidy than in fetuses with normal karyotype (p = 0.001; p = 0.013; p = 0.028). In the ROC analysis, the CSP width/length ratio had the optimal cutoff value of 0.59, with 72.0% sensitivity and 58.0% specificity, and for the CSP width/BPD ratio, the cutoff value was 0.081 with 83.0% sensitivity and 61.0% specificity for detection of aneuploidy.
CSP width z-score was found to be increased in aneuploid fetuses. The CSP width /BPD ratio can be used as a new marker for predicting aneuploidy.
Summary
Rev Bras Ginecol Obstet. 2013;35(6):274-280
DOI 10.1590/S0100-72032013000600007
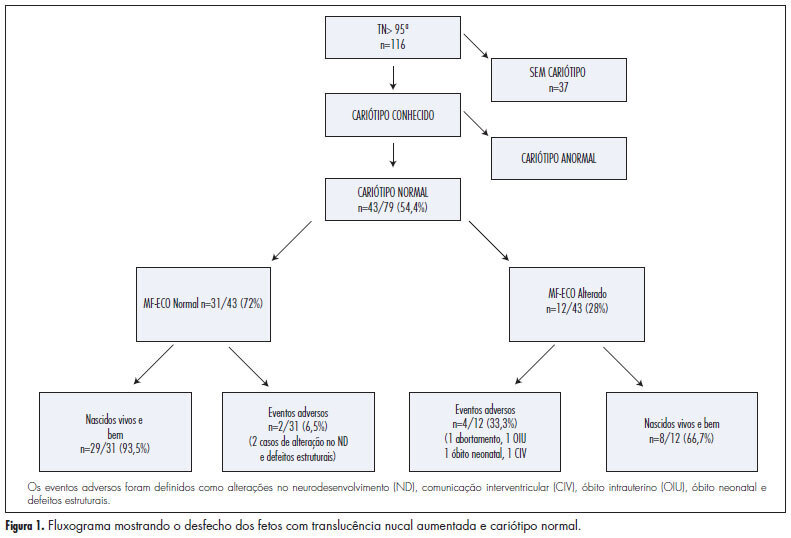
PURPOSE: To analyze the perinatal and pediatric outcome of fetuses that showed nuchal translucency (NT) above the 95th percentile (P95) and a normal karyotype in order to obtain data allowing better maternal prenatal counseling. METHODS: fetuses from a tertiary obstetric service with an NT above P95 and a normal karyotype were analyzed between 2005 and 2011. We analyzed gestational ultrasound follow-up, fetal and postnatal echocardiography (ECHO), weight, length and Apgar score at birth, and neuropsychomotor development by the Ages and Stages Questionnaire (ASQ) up to July 2012. RESULTS: During this period, there were 116 cases of nuchal translucency above the 95th percentile, and the fetal karyotype was determined in 79 of them (68%). Forty-three analyses were normal (54.4%) and 36 were altered (45.6%). Among the fetuses with a normal karyotype, one was miscarried at 15 weeks of gestation with Cantrel pentalogy and one died at 24 weeks with several structural abnormalities. There was one neonatal death of unknown cause and two cases of intraventricular communication (IVC) detected by fetal ECHO. Postnatal echocardiography revealed the persistence of IVC in one case and one case of atrial septal defect (ASD) and patent ductus arteriosus (PDA). Of the 40 surviving children, only 1 showed delayed speech development and another presented autism. The remaining cases resulted in normal neurodevelopment. CONCLUSION: During the monitoring of fetuses with increased NT and a normal karyotype, parents can be best advised that when a 2nd trimester morphological-echocardiography ultrasound study is normal, the probability of the child being born alive and well is high (93.5%).
Summary
Rev Bras Ginecol Obstet. 2013;35(6):274-280
DOI 10.1590/S0100-72032013000600007
PURPOSE: To analyze the perinatal and pediatric outcome of fetuses that showed nuchal translucency (NT) above the 95th percentile (P95) and a normal karyotype in order to obtain data allowing better maternal prenatal counseling. METHODS: fetuses from a tertiary obstetric service with an NT above P95 and a normal karyotype were analyzed between 2005 and 2011. We analyzed gestational ultrasound follow-up, fetal and postnatal echocardiography (ECHO), weight, length and Apgar score at birth, and neuropsychomotor development by the Ages and Stages Questionnaire (ASQ) up to July 2012. RESULTS: During this period, there were 116 cases of nuchal translucency above the 95th percentile, and the fetal karyotype was determined in 79 of them (68%). Forty-three analyses were normal (54.4%) and 36 were altered (45.6%). Among the fetuses with a normal karyotype, one was miscarried at 15 weeks of gestation with Cantrel pentalogy and one died at 24 weeks with several structural abnormalities. There was one neonatal death of unknown cause and two cases of intraventricular communication (IVC) detected by fetal ECHO. Postnatal echocardiography revealed the persistence of IVC in one case and one case of atrial septal defect (ASD) and patent ductus arteriosus (PDA). Of the 40 surviving children, only 1 showed delayed speech development and another presented autism. The remaining cases resulted in normal neurodevelopment. CONCLUSION: During the monitoring of fetuses with increased NT and a normal karyotype, parents can be best advised that when a 2nd trimester morphological-echocardiography ultrasound study is normal, the probability of the child being born alive and well is high (93.5%).
Summary
Rev Bras Ginecol Obstet. 2008;30(10):511-517
DOI 10.1590/S0100-72032008001000006
PURPOSE: to correlate the clinical manifestations of patients with amenorrhea and X chromosome abnormalities. METHODS: a retrospective analysis of the clinical and laboratorial findings of patients with amenorrhea and abnormalities of X chromosome, attended between January 1975 and November 2007 was performed. Their anthropometric measures were evaluated through standard growth tables, and, when present, minor and major anomalies were noted. The chromosomal study was performed through the GTG banded karyotype. RESULTS: from the total of 141 patients with amenorrhea, 16% presented numerical and 13% structural abnormalities of X chromosome. From these patients with X chromosome abnormalities (n=41), 35 had a complete clinical description. All presented hypergonadotrophic hypogonadism. Primary amenorrhea was observed in 24 patients, 91.7% of them with a Turner syndrome phenotype. Despite a case with Xq22-q28 deletion, all patients with this phenotype presented alterations involving Xp (one case with an additional cell lineage 46,XY). The two remaining patients with only primary amenorrhea had proximal deletions of Xq. Among the 11 patients with secondary amenorrhea, 54.5% presented a Turner phenotype (all with isolated or mosaic X chromosome monosomy). Patients with phenotype of isolated ovarian failure had only Xq deletions and X trisomy. CONCLUSIONS: the cytogenetic analysis must always be performed in women with ovarian failure of unknown cause, even in the absence of clinical dysmorphic features. This analysis is also extremely relevant in syndromic patients, because it can either confirm the diagnosis or identify patients in risk, like the cases involving a 46,XY lineage.
Summary
Rev Bras Ginecol Obstet. 2008;30(10):511-517
DOI 10.1590/S0100-72032008001000006
PURPOSE: to correlate the clinical manifestations of patients with amenorrhea and X chromosome abnormalities. METHODS: a retrospective analysis of the clinical and laboratorial findings of patients with amenorrhea and abnormalities of X chromosome, attended between January 1975 and November 2007 was performed. Their anthropometric measures were evaluated through standard growth tables, and, when present, minor and major anomalies were noted. The chromosomal study was performed through the GTG banded karyotype. RESULTS: from the total of 141 patients with amenorrhea, 16% presented numerical and 13% structural abnormalities of X chromosome. From these patients with X chromosome abnormalities (n=41), 35 had a complete clinical description. All presented hypergonadotrophic hypogonadism. Primary amenorrhea was observed in 24 patients, 91.7% of them with a Turner syndrome phenotype. Despite a case with Xq22-q28 deletion, all patients with this phenotype presented alterations involving Xp (one case with an additional cell lineage 46,XY). The two remaining patients with only primary amenorrhea had proximal deletions of Xq. Among the 11 patients with secondary amenorrhea, 54.5% presented a Turner phenotype (all with isolated or mosaic X chromosome monosomy). Patients with phenotype of isolated ovarian failure had only Xq deletions and X trisomy. CONCLUSIONS: the cytogenetic analysis must always be performed in women with ovarian failure of unknown cause, even in the absence of clinical dysmorphic features. This analysis is also extremely relevant in syndromic patients, because it can either confirm the diagnosis or identify patients in risk, like the cases involving a 46,XY lineage.

Summary
Rev Bras Ginecol Obstet. 2005;27(3):155-160
DOI 10.1590/S0100-72032005000300010
PURPOSE: to evaluate the outcome of fetuses with risk of chromosomal anomalies over 1:300, based on the nuchal translucency measurement, according to the Fetal Medicine Program. METHODS: in the pregnancies with risk of chromosomal anomalies over 1:300, variables like fetal karyotype, spontaneous or induced abortion, prematurity, stillbirth, neonatal death, malformations, and healthy newborn were considered. We used Fisher's exact test to compare differences in proportions between groups. RESULTS: we selected 193 (3.6%) single pregnancies with risk of chromosomal anomalies over 1:300. Only 165 cases fulfilled the inclusion criteria. Of these only 32.1% underwent fetal karyotyping and of which 8.5% had chromosomal anomalies (85.7% had trisomy 21). Regarding pregnancy outcomes, 4.2% were spontaneous miscarriages, 4.2% induced abortions, 4.8% were premature, 1.8% had neonatal death, 1.8% were stillborn, and 4.2% had structural malformation (85.7% congenital heart diseases). Almost 85.0% were healthy newborns. Patients with abnormal karyotyping had more induced abortions (p<0.001) and more structural malformations (p<0.001) than patients with normal karyotyping. None of the genetic diseases or miscarriages was associated with invasive procedures. Sixty-six percent of the pregnancies with prenatal diagnosis of abnormal karyotype were interrupted. CONCLUSION: nuchal translucency is an important screening tool for chromosomal diseases especially for low-risk pregnancies. However, counseling pregnancies with high risk of chromosomal anomalies should consider that, although these fetuses have a worse prognosis, most of the outcomes are favorable.
Summary
Rev Bras Ginecol Obstet. 2005;27(3):155-160
DOI 10.1590/S0100-72032005000300010
PURPOSE: to evaluate the outcome of fetuses with risk of chromosomal anomalies over 1:300, based on the nuchal translucency measurement, according to the Fetal Medicine Program. METHODS: in the pregnancies with risk of chromosomal anomalies over 1:300, variables like fetal karyotype, spontaneous or induced abortion, prematurity, stillbirth, neonatal death, malformations, and healthy newborn were considered. We used Fisher's exact test to compare differences in proportions between groups. RESULTS: we selected 193 (3.6%) single pregnancies with risk of chromosomal anomalies over 1:300. Only 165 cases fulfilled the inclusion criteria. Of these only 32.1% underwent fetal karyotyping and of which 8.5% had chromosomal anomalies (85.7% had trisomy 21). Regarding pregnancy outcomes, 4.2% were spontaneous miscarriages, 4.2% induced abortions, 4.8% were premature, 1.8% had neonatal death, 1.8% were stillborn, and 4.2% had structural malformation (85.7% congenital heart diseases). Almost 85.0% were healthy newborns. Patients with abnormal karyotyping had more induced abortions (p<0.001) and more structural malformations (p<0.001) than patients with normal karyotyping. None of the genetic diseases or miscarriages was associated with invasive procedures. Sixty-six percent of the pregnancies with prenatal diagnosis of abnormal karyotype were interrupted. CONCLUSION: nuchal translucency is an important screening tool for chromosomal diseases especially for low-risk pregnancies. However, counseling pregnancies with high risk of chromosomal anomalies should consider that, although these fetuses have a worse prognosis, most of the outcomes are favorable.
Summary
Rev Bras Ginecol Obstet. 2005;27(3):125-129
DOI 10.1590/S0100-72032005000300005
BACKGROUND: patients with primary amenorrhea and gonadal dysgenesia have higher serum gonadotrophins and should be submitted to chromosome studies. Karyotype studies may be performed in gonadal tissue or peripheral blood however, it is not yet established if cases of primary amenorrhea without signs of virilization need additional investigation of gonadal karyotype. PURPOSE: to analize the gonadal karyotypes (ovaries) from patients with primary amenorrhea and compare them to their respective peripheral blood karyotypes. METHODS: clinical and karyotype data of 12 patients were retrospectively analyzed from January 1997 to December 2003. RESULTS: when the investigation was indicated for primary amenorrhea without signs of virilization, the gonadal and peripheral blood karyotypes were concordant in 8 cases (7 cases 46XX and 1 case 46XY). One patient with virilization signs was the only case of discordant karyotype. CONCLUSION: the present study suggests that the gonadal karyotype does not bring additional information to peripheral blood karyotype in patients with amenorrhea and no signs of virilization. Although all previous studies had a small number of patients, it seems advisable to investigate the gonadal karyotype in patients with signs of virilization. The cost-benefit analysis could allow cost and stress reduction for patients, family and institutions.
Summary
Rev Bras Ginecol Obstet. 2005;27(3):125-129
DOI 10.1590/S0100-72032005000300005
BACKGROUND: patients with primary amenorrhea and gonadal dysgenesia have higher serum gonadotrophins and should be submitted to chromosome studies. Karyotype studies may be performed in gonadal tissue or peripheral blood however, it is not yet established if cases of primary amenorrhea without signs of virilization need additional investigation of gonadal karyotype. PURPOSE: to analize the gonadal karyotypes (ovaries) from patients with primary amenorrhea and compare them to their respective peripheral blood karyotypes. METHODS: clinical and karyotype data of 12 patients were retrospectively analyzed from January 1997 to December 2003. RESULTS: when the investigation was indicated for primary amenorrhea without signs of virilization, the gonadal and peripheral blood karyotypes were concordant in 8 cases (7 cases 46XX and 1 case 46XY). One patient with virilization signs was the only case of discordant karyotype. CONCLUSION: the present study suggests that the gonadal karyotype does not bring additional information to peripheral blood karyotype in patients with amenorrhea and no signs of virilization. Although all previous studies had a small number of patients, it seems advisable to investigate the gonadal karyotype in patients with signs of virilization. The cost-benefit analysis could allow cost and stress reduction for patients, family and institutions.
Summary
Rev Bras Ginecol Obstet. 2001;23(4):243-246
DOI 10.1590/S0100-72032001000400007
Purpose: to evaluate the possibility and accuracy of fetal karyotyping in pleural effusions. Methods: we studied fifteen fetuses with unilateral or bilateral pleural effusions. All of these fetuses underwent intrauterine thoracocentesis guided by ultrasound examinations. The gestational age varied from 19 to 34 weeks. A morphogenetic ultrasound examination was performed in each case by the authors in order to identify associated structural anomalies. When the cellular cultures of pleural effusion samples were negative, an alternative karyotype was obtained by cordocentesis. A fetal lymphocyte culture was made of pleural effusion samples for karyotype in a similar technique as for fetal blood. Results: the fetal karyotype was successful in 12 cases. There were 4 abnormal results, all of them were Down syndromes, and in the other 8 cases the chromosomal analyses were normal. The fetal karyotype was confirmed and compared by newborn blood chromosomal analysis, genetic evaluation or necropsy. There were no maternal or fetal side effects related to the procedure. Conclusions: the fetal karyotyping performed in pleural effusions obtained by intrauterine thoracocentesis proved to be highly efficient and safe. It must be the method of choice for rapid karyotyping in fetuses with pleural edema.
Summary
Rev Bras Ginecol Obstet. 2001;23(4):243-246
DOI 10.1590/S0100-72032001000400007
Purpose: to evaluate the possibility and accuracy of fetal karyotyping in pleural effusions. Methods: we studied fifteen fetuses with unilateral or bilateral pleural effusions. All of these fetuses underwent intrauterine thoracocentesis guided by ultrasound examinations. The gestational age varied from 19 to 34 weeks. A morphogenetic ultrasound examination was performed in each case by the authors in order to identify associated structural anomalies. When the cellular cultures of pleural effusion samples were negative, an alternative karyotype was obtained by cordocentesis. A fetal lymphocyte culture was made of pleural effusion samples for karyotype in a similar technique as for fetal blood. Results: the fetal karyotype was successful in 12 cases. There were 4 abnormal results, all of them were Down syndromes, and in the other 8 cases the chromosomal analyses were normal. The fetal karyotype was confirmed and compared by newborn blood chromosomal analysis, genetic evaluation or necropsy. There were no maternal or fetal side effects related to the procedure. Conclusions: the fetal karyotyping performed in pleural effusions obtained by intrauterine thoracocentesis proved to be highly efficient and safe. It must be the method of choice for rapid karyotyping in fetuses with pleural edema.
Summary
Rev Bras Ginecol Obstet. 2002;24(2):121-127
DOI 10.1590/S0100-72032002000200008
Purpose: to estimate the performance of ultrasound to detect gestations at risk for fetal chromosomal abnormalities. Methods: four hundred and thirty-six patients selected for the study had undergone ultrasound examination and fetal karyotyping, between March 1993 and March 1998. Two hundred and seventy-seven patients had fetal karyotype for fetal malformation detected on ultrasound and 158 for parental anxiety with normal ultrasound examination. Ultrasound sensitivity and specificity were calculated using fetal karyotype as gold standard. The relative risk for each chromosomal abnormality was calculated according to the altered system on ultrasound examination and the risks of the presence of one or more abnormalities on ultrasound, using the Epi-Info 6.0 software package for statistical analysis. Results: the relative risks for chromosomal abnormalities were 89 for face malformations, 53 for abdominal wall and cardiovascular, 49.6 for neck, 44.6 for extremities, 42.4 for lung, 32.7 for gastrointestinal tract, 27.4 for central nervous system and 23.0 for urinary tract malformations. The relative risk for fetal chromosomal anomalies for genital, thorax, spine and muscle and/or skeletal malformations was not appropriate for calculation because they occurred at very low frequencies. An isolated malformation detected by ultrasound is associated with a 7.8 times higher relative risk for chromosomal anomalies than none, and associated morphologic malformations have a 33.8 times higher relative risk for chromosomal abnormalities. Conclusion: ultrasound has good performance to detect gestations at risk for chromosomal abnormalities.
Summary
Rev Bras Ginecol Obstet. 2002;24(2):121-127
DOI 10.1590/S0100-72032002000200008
Purpose: to estimate the performance of ultrasound to detect gestations at risk for fetal chromosomal abnormalities. Methods: four hundred and thirty-six patients selected for the study had undergone ultrasound examination and fetal karyotyping, between March 1993 and March 1998. Two hundred and seventy-seven patients had fetal karyotype for fetal malformation detected on ultrasound and 158 for parental anxiety with normal ultrasound examination. Ultrasound sensitivity and specificity were calculated using fetal karyotype as gold standard. The relative risk for each chromosomal abnormality was calculated according to the altered system on ultrasound examination and the risks of the presence of one or more abnormalities on ultrasound, using the Epi-Info 6.0 software package for statistical analysis. Results: the relative risks for chromosomal abnormalities were 89 for face malformations, 53 for abdominal wall and cardiovascular, 49.6 for neck, 44.6 for extremities, 42.4 for lung, 32.7 for gastrointestinal tract, 27.4 for central nervous system and 23.0 for urinary tract malformations. The relative risk for fetal chromosomal anomalies for genital, thorax, spine and muscle and/or skeletal malformations was not appropriate for calculation because they occurred at very low frequencies. An isolated malformation detected by ultrasound is associated with a 7.8 times higher relative risk for chromosomal anomalies than none, and associated morphologic malformations have a 33.8 times higher relative risk for chromosomal abnormalities. Conclusion: ultrasound has good performance to detect gestations at risk for chromosomal abnormalities.
Search
Search in:
breast (42) breast cancer (42) breast neoplasms (95) Cesarean section (72) endometriosis (66) infertility (56) Maternal mortality (43) menopause (82) obesity (58) postpartum period (40) pregnancy (225) Pregnancy complications (99) Prenatal care (68) prenatal diagnosis (50) Prevalence (41) Quality of life (51) risk factors (94) ultrasonography (79) urinary incontinence (40) women's health (48)