Summary
Rev Bras Ginecol Obstet. 2023;45(12):796-807
Menopause causes several changes in the body that may affect the response to COVID-19. We aimed to investigate the possible association between menopausal status and incidence and outcomes in COVID-19 patients.
Combinations of keywordsCOVID-19, menopause, and estrogen were used to search the PubMed, Embase, Web-of-Science, and Scopus databases for articles reporting the incidence and outcomes of COVID-19 (discharge, length-of-admission, intensive care, or mortality) in premenopausal women, available through December 29, 2022. Data from studies comparing the incidence of COVID-19 infection with the age-matched male population were pooled and meta-analyzed using a random-effects model.
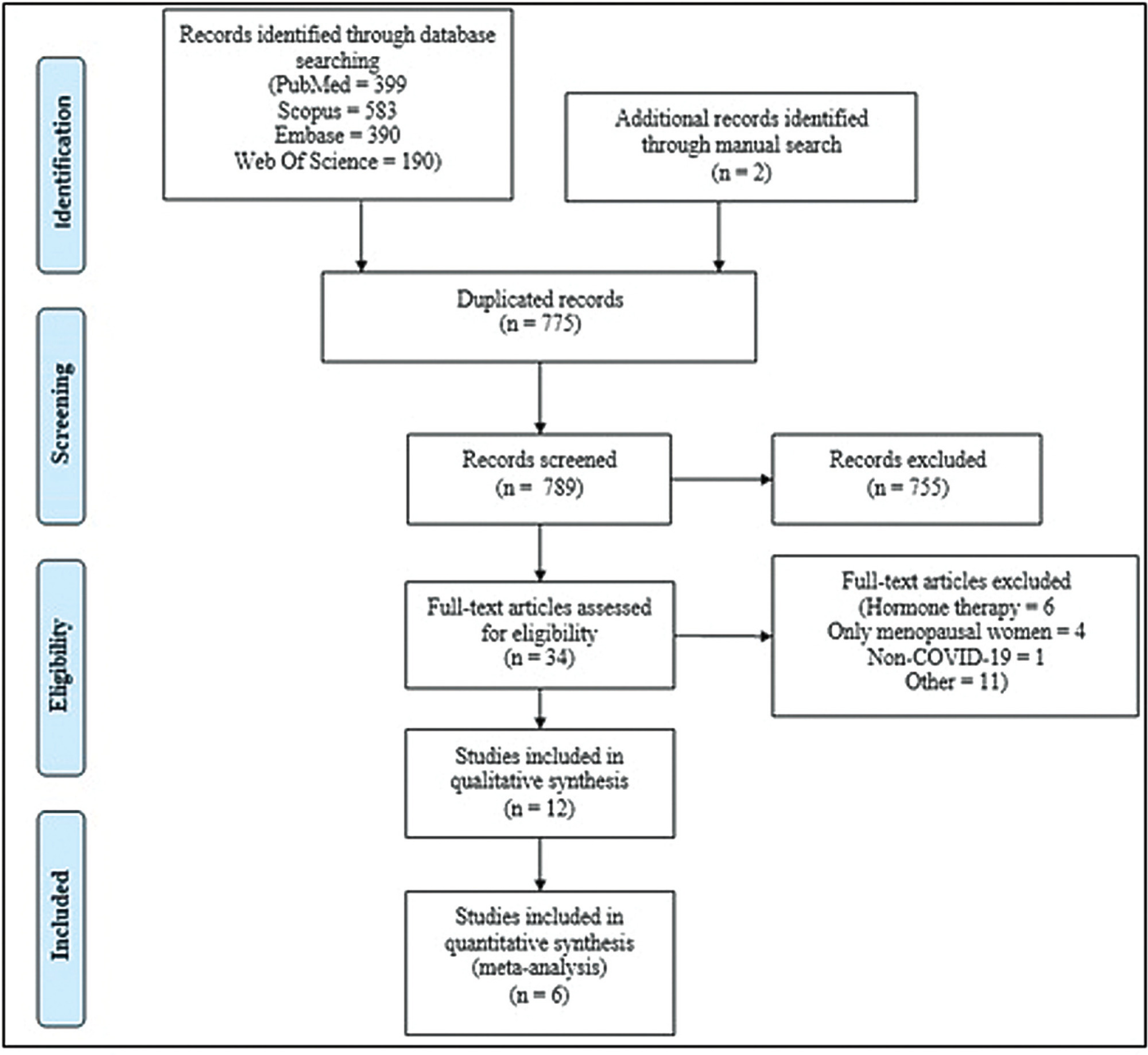
Overall, 1,564 studies were retrieved, of which 12 were finally included in the systematic review to compare disease outcomes, and 6 were meta-analyzed for the incidence of COVID-19 in premenopausal and postmenopausal women. All studies reported better COVID-19-associated outcomes in premenopausal women compared with postmenopausal women. After adjusting for confounding factors, three studies found better outcomes in postmenopausal women, and two found no association between menopausal status and COVID-19 outcomes. Our meta-analysis found a higher incidence of COVID-19 infection among premenopausal women than postmenopausal women, when compared with age-matched men (odds ratio = 1.270; 95% confidence interval: 1.086–1.486; p = 0.003).
The incidence of COVID-19 was significantly higher in premenopausal women than in postmenopausal women when compared with age-matched men. Although premenopausal women may have more favorable COVID-19-associated outcomes, the presumed preventive effect of estrogens on the incidence and related outcomes of COVID-19 in premenopausal women cannot be proven at present. Further longitudinal studies comparing pre- and post-menopausal women are required to provide further insight into this matter.
Summary
Rev Bras Ginecol Obstet. 2023;45(12):796-807
Menopause causes several changes in the body that may affect the response to COVID-19. We aimed to investigate the possible association between menopausal status and incidence and outcomes in COVID-19 patients.
Combinations of keywordsCOVID-19, menopause, and estrogen were used to search the PubMed, Embase, Web-of-Science, and Scopus databases for articles reporting the incidence and outcomes of COVID-19 (discharge, length-of-admission, intensive care, or mortality) in premenopausal women, available through December 29, 2022. Data from studies comparing the incidence of COVID-19 infection with the age-matched male population were pooled and meta-analyzed using a random-effects model.
Overall, 1,564 studies were retrieved, of which 12 were finally included in the systematic review to compare disease outcomes, and 6 were meta-analyzed for the incidence of COVID-19 in premenopausal and postmenopausal women. All studies reported better COVID-19-associated outcomes in premenopausal women compared with postmenopausal women. After adjusting for confounding factors, three studies found better outcomes in postmenopausal women, and two found no association between menopausal status and COVID-19 outcomes. Our meta-analysis found a higher incidence of COVID-19 infection among premenopausal women than postmenopausal women, when compared with age-matched men (odds ratio = 1.270; 95% confidence interval: 1.086–1.486; p = 0.003).
The incidence of COVID-19 was significantly higher in premenopausal women than in postmenopausal women when compared with age-matched men. Although premenopausal women may have more favorable COVID-19-associated outcomes, the presumed preventive effect of estrogens on the incidence and related outcomes of COVID-19 in premenopausal women cannot be proven at present. Further longitudinal studies comparing pre- and post-menopausal women are required to provide further insight into this matter.
Summary
Rev Bras Ginecol Obstet. 2023;45(8):465-473
To analyze the effect of combined training (CT) in postural control and gait parameters in postmenopausal women.
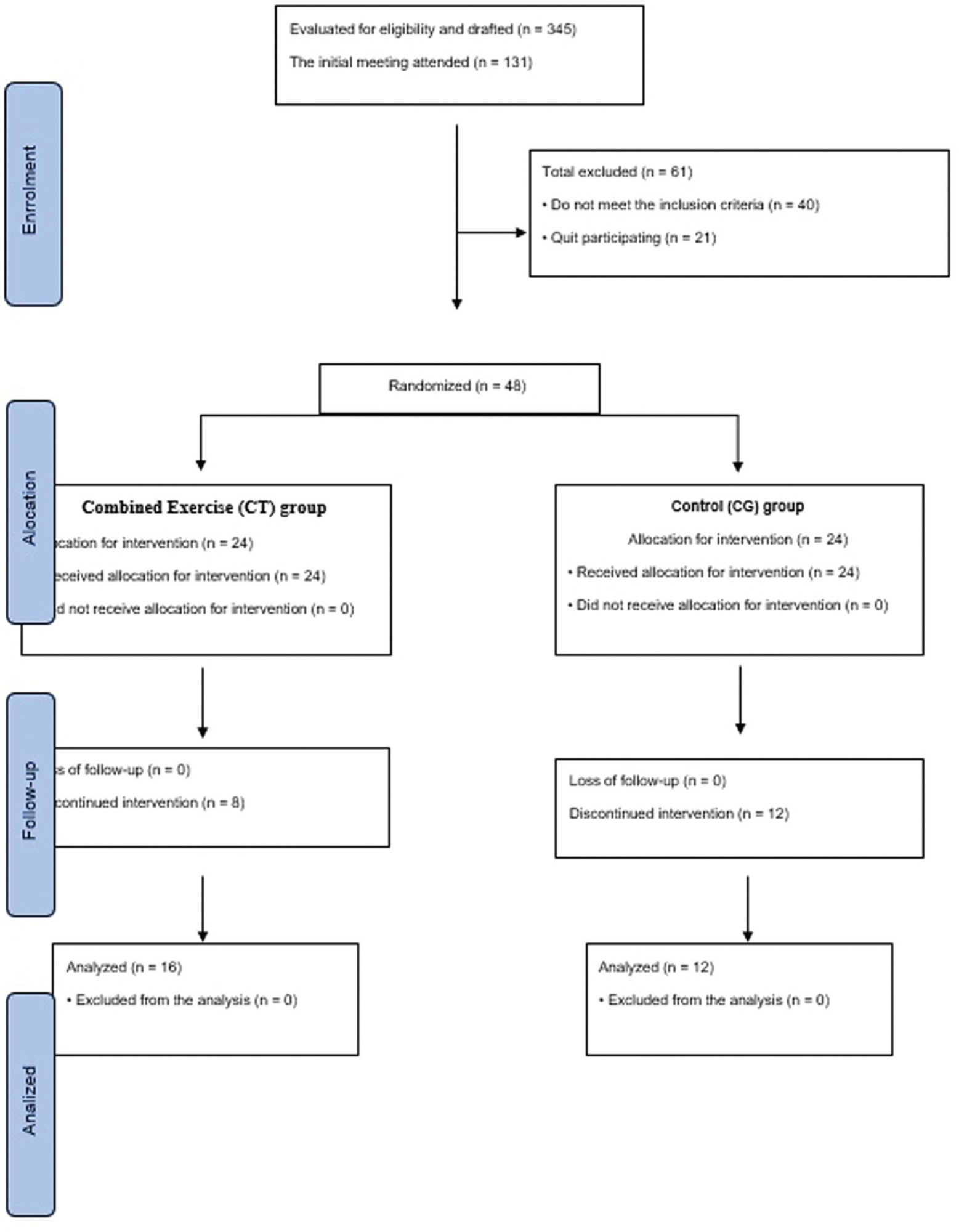
A parallel-group, randomized, control study was conducted with 16 weeks of combined training (n = 16) versus a non-training control group (n = 12) in postmenopausal women (aged 59.3 ± 8.0). Pre and postintervention assessments included postural control (using an AMTI force platform – Advanced Mechanical Technology, Inc., Watertown, MA, USA) and gait impairments (using baropodometry). In addition, the upper limb strength and abdominal tests, as well as aerobic capacity, assessed functional indicators.
The CT intervention in postmenopausal women resulted in improved gait (stride length (p = 0.006); speed (p = 0.013); double support time (p = 0.045); and improved postural control (displacement area of postural sway in a normal base of support with eyes open (p = 0.006). Combined training increased functional indicators (abdominal - p = 0.031; aerobic capacity - p = 0.002).
In conclusion, combined aerobic plus strength training effectively improved gait and balance control in older women. The postmenopausal women from the CT group walked faster and with bigger steps after the intervention than the control group. In addition, they presented decreased postural sway in standing and decreased the percentage of double support time while walking, which means improved static and dynamic balance control and functional indicators.
Summary
Rev Bras Ginecol Obstet. 2023;45(8):465-473
To analyze the effect of combined training (CT) in postural control and gait parameters in postmenopausal women.
A parallel-group, randomized, control study was conducted with 16 weeks of combined training (n = 16) versus a non-training control group (n = 12) in postmenopausal women (aged 59.3 ± 8.0). Pre and postintervention assessments included postural control (using an AMTI force platform – Advanced Mechanical Technology, Inc., Watertown, MA, USA) and gait impairments (using baropodometry). In addition, the upper limb strength and abdominal tests, as well as aerobic capacity, assessed functional indicators.
The CT intervention in postmenopausal women resulted in improved gait (stride length (p = 0.006); speed (p = 0.013); double support time (p = 0.045); and improved postural control (displacement area of postural sway in a normal base of support with eyes open (p = 0.006). Combined training increased functional indicators (abdominal - p = 0.031; aerobic capacity - p = 0.002).
In conclusion, combined aerobic plus strength training effectively improved gait and balance control in older women. The postmenopausal women from the CT group walked faster and with bigger steps after the intervention than the control group. In addition, they presented decreased postural sway in standing and decreased the percentage of double support time while walking, which means improved static and dynamic balance control and functional indicators.
Summary
Rev Bras Ginecol Obstet. 2022;44(10):986-994
To evaluate the efficacy of the hormonal and nonhormonal approaches to symptoms of sexual dysfunction and vaginal atrophy in postmenopausal women.
We conducted a search on the PubMed, Embase, Scopus, Web of Science, SciELO, the Cochrane Central Register of Controlled Trials (CENTRAL), and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases, as well as on clinical trial databases. We analyzed studies published between 1996 and May 30, 2020. No language restrictions were applied.
We selected randomized clinical trials that evaluated the treatment of sexual dysfunction in postmenopausal women.
Three authors (ACAS, APFC, and JL) reviewed each article based on its title and abstract. Relevant data were subsequently taken from the full-text article. Any discrepancies during the review were resolved by consensus between all the listed authors.
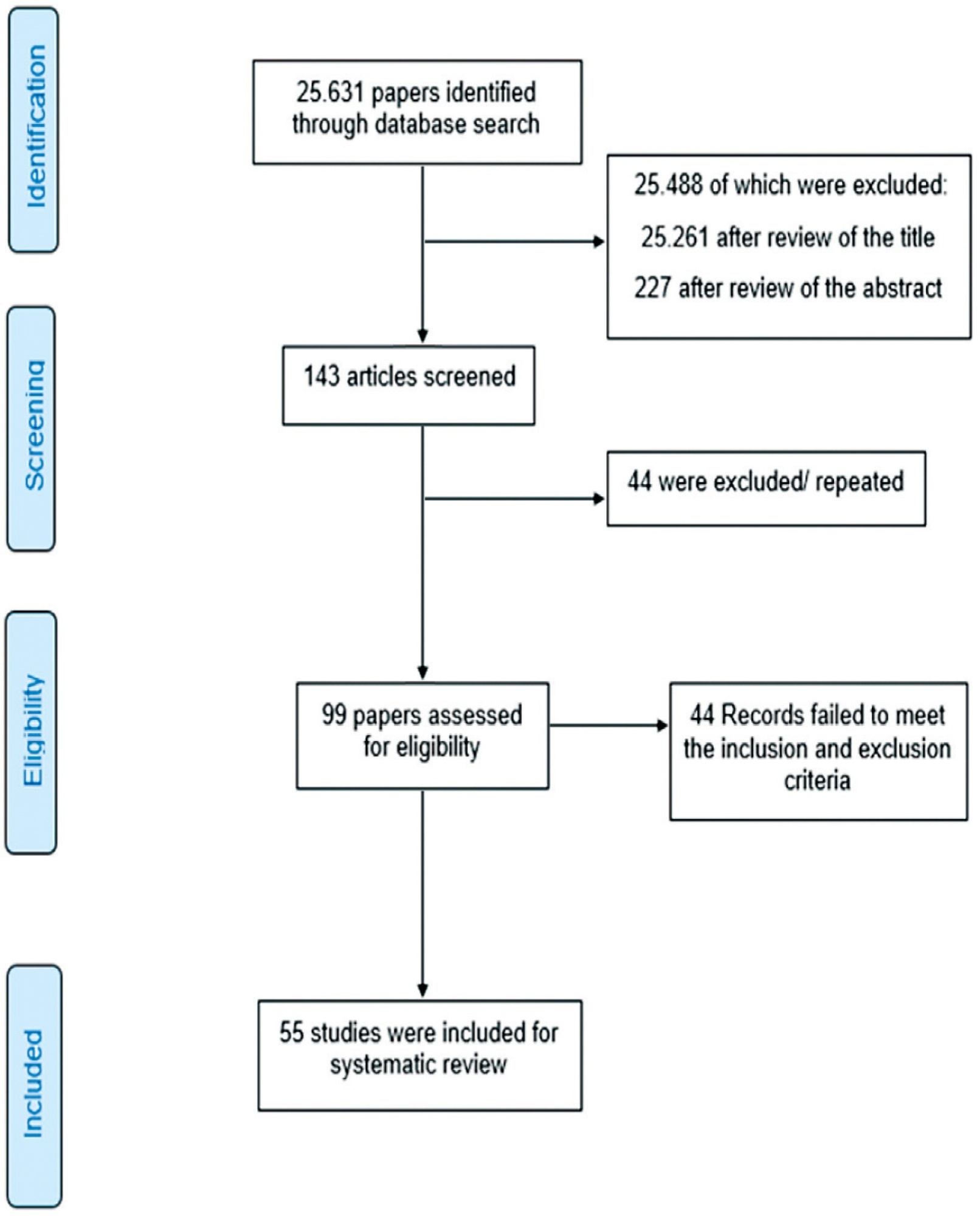
A total of 55 studies were included in the systematic review. The approaches tested to treat sexual dysfunction were as follows: lubricants and moisturizers (18 studies); phytoestrogens (14 studies); dehydroepiandrosterone (DHEA; 8 studies); ospemifene (5 studies); vaginal testosterone (4 studies); pelvic floor muscle exercises (2 studies); oxytocin (2 studies); vaginal CO2 laser (2 studies); lidocaine (1 study); and vitamin E vaginal suppository (1 study).
We identified literature that lacks coherence in terms of the proposed treatments and selected outcome measures. Despite the great diversity in treatment modalities and outcome measures, the present systematic review can shed light on potential targets for the treatment, which is deemed necessary for sexual dysfunction, assuming that most randomized trials were evaluated with a low risk of bias according to the Cochrane Collaboration risk of bias tool. The present review is registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42018100488).
Summary
Rev Bras Ginecol Obstet. 2022;44(10):986-994
To evaluate the efficacy of the hormonal and nonhormonal approaches to symptoms of sexual dysfunction and vaginal atrophy in postmenopausal women.
We conducted a search on the PubMed, Embase, Scopus, Web of Science, SciELO, the Cochrane Central Register of Controlled Trials (CENTRAL), and Cumulative Index to Nursing and Allied Health Literature (CINAHL) databases, as well as on clinical trial databases. We analyzed studies published between 1996 and May 30, 2020. No language restrictions were applied.
We selected randomized clinical trials that evaluated the treatment of sexual dysfunction in postmenopausal women.
Three authors (ACAS, APFC, and JL) reviewed each article based on its title and abstract. Relevant data were subsequently taken from the full-text article. Any discrepancies during the review were resolved by consensus between all the listed authors.
A total of 55 studies were included in the systematic review. The approaches tested to treat sexual dysfunction were as follows: lubricants and moisturizers (18 studies); phytoestrogens (14 studies); dehydroepiandrosterone (DHEA; 8 studies); ospemifene (5 studies); vaginal testosterone (4 studies); pelvic floor muscle exercises (2 studies); oxytocin (2 studies); vaginal CO2 laser (2 studies); lidocaine (1 study); and vitamin E vaginal suppository (1 study).
We identified literature that lacks coherence in terms of the proposed treatments and selected outcome measures. Despite the great diversity in treatment modalities and outcome measures, the present systematic review can shed light on potential targets for the treatment, which is deemed necessary for sexual dysfunction, assuming that most randomized trials were evaluated with a low risk of bias according to the Cochrane Collaboration risk of bias tool. The present review is registered with the International Prospective Register of Systematic Reviews (PROSPERO; CRD42018100488).
Summary
Rev Bras Ginecol Obstet. 2022;44(6):586-592
To determine if there is a correlation between body mass index (BMI) and climacteric symptoms in postmenopausal women.
The study sample was composed of 109 postmenopausal women with a mean age of 57 ± 8 years, mean body mass index (BMI) of 30 ± 6 kg/m2, and 8 ± 8 years after menopause. For the assessment of the climacteric symptoms, the Blatt-Kupperman Index (BKI), the Menopause Rating Scale (MRS), and the Cervantes Scale (CS) were used. Data analysis was performed through the Chi-squared test, analysis of variance (ANOVA) with the Bonferroni post hoc test, and multiple linear regression. The level of significance adopted was of p < 0.05. The statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, United States) software, version 26.0.
The multiple linear regression showed a positive association (p<0.01) between BMI values and menopause symptoms when adjusted for age and time after menopause in the 3 questionnaires used (BKI: B = 0.432; CS: B = 304; and MRS: B = 302). Regarding symptom scores, the obese women had higher mean scores (p<0.05) when compared to eutrophic women (BKI = 28 ± 10 and 20 ± 10; and MRS = 20 ± 10 and 13±7, respectively). In the Chi-squared analysis, 28% of obese women had severe symptoms and 46% had moderate symptoms, while only 1% and 46% of eutrophic women had these same symptoms.
There is an association between BMI and climacteric symptoms, and overweight or obese women have more intense and moderate symptoms than eutrophic women.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):586-592
To determine if there is a correlation between body mass index (BMI) and climacteric symptoms in postmenopausal women.
The study sample was composed of 109 postmenopausal women with a mean age of 57 ± 8 years, mean body mass index (BMI) of 30 ± 6 kg/m2, and 8 ± 8 years after menopause. For the assessment of the climacteric symptoms, the Blatt-Kupperman Index (BKI), the Menopause Rating Scale (MRS), and the Cervantes Scale (CS) were used. Data analysis was performed through the Chi-squared test, analysis of variance (ANOVA) with the Bonferroni post hoc test, and multiple linear regression. The level of significance adopted was of p < 0.05. The statistical analyses were performed using the Statistical Package for the Social Sciences (IBM SPSS Statistics for Windows, IBM Corp., Armonk, NY, United States) software, version 26.0.
The multiple linear regression showed a positive association (p<0.01) between BMI values and menopause symptoms when adjusted for age and time after menopause in the 3 questionnaires used (BKI: B = 0.432; CS: B = 304; and MRS: B = 302). Regarding symptom scores, the obese women had higher mean scores (p<0.05) when compared to eutrophic women (BKI = 28 ± 10 and 20 ± 10; and MRS = 20 ± 10 and 13±7, respectively). In the Chi-squared analysis, 28% of obese women had severe symptoms and 46% had moderate symptoms, while only 1% and 46% of eutrophic women had these same symptoms.
There is an association between BMI and climacteric symptoms, and overweight or obese women have more intense and moderate symptoms than eutrophic women.
Summary
Rev Bras Ginecol Obstet. 2022;44(1):32-39
To evaluate the improvement in screening accuracy of the Fracture Risk Assessment Tool (FRAX) for the risk of developing osteoporosis among young postmenopausal women by associating with it clinical muscle mass measures.
A sample of postmenopausal women was submitted to calcaneal quantitative ultrasound (QUS), application of the FRAX questionnaire, and screening for the risk of developing sarcopenia at a health fair held in the city of São Bernardo do Campo in 2019. The sample also underwent anthropometric measurements, muscle mass, walking speed and handgrip tests. A major osteoporotic fracture (MOF) risk ≥ 8.5% on the FRAX, a classification of medium risk on the clinical guideline of the National Osteoporosis Guideline Group (NOGG), and a QUS T-score ≤ -1.8 sd were considered risks of having low bone mass, and QUS T-score ≤ -2.5sd, risk of having fractures.
In total, 198 women were evaluated, with a median age of 64±7.7 years, median body mass index (BMI) of 27.3±5.3 kg/m2 and median QUS T-score of -1.3±1.3 sd. The accuracy of the FRAX with a MOF risk ≥ 8.5% to identify women with T-scores ≤ -1.8 sd was poor, with an area under the curve (AUC) of 0.604 (95% confidence interval [95%CI]: 0.509-0.694) for women under 65 years of age, and of 0.642 (95%CI: 0.571-0.709) when age was not considered. Including data on muscle mass in the statistical analysis led to a significant improvement for the group of women under 65 years of age, with an AUC of 0,705 (95%CI: 0.612-0.786). The ability of the high-risk NOGG tool to identify T-scores ≤ -1.8 sd was limited.
Clinical muscle mass measurements increased the accuracy of the FRAX to screen for osteoporosis in women aged under 65 years.
Summary
Rev Bras Ginecol Obstet. 2022;44(1):32-39
To evaluate the improvement in screening accuracy of the Fracture Risk Assessment Tool (FRAX) for the risk of developing osteoporosis among young postmenopausal women by associating with it clinical muscle mass measures.
A sample of postmenopausal women was submitted to calcaneal quantitative ultrasound (QUS), application of the FRAX questionnaire, and screening for the risk of developing sarcopenia at a health fair held in the city of São Bernardo do Campo in 2019. The sample also underwent anthropometric measurements, muscle mass, walking speed and handgrip tests. A major osteoporotic fracture (MOF) risk ≥ 8.5% on the FRAX, a classification of medium risk on the clinical guideline of the National Osteoporosis Guideline Group (NOGG), and a QUS T-score ≤ -1.8 sd were considered risks of having low bone mass, and QUS T-score ≤ -2.5sd, risk of having fractures.
In total, 198 women were evaluated, with a median age of 64±7.7 years, median body mass index (BMI) of 27.3±5.3 kg/m2 and median QUS T-score of -1.3±1.3 sd. The accuracy of the FRAX with a MOF risk ≥ 8.5% to identify women with T-scores ≤ -1.8 sd was poor, with an area under the curve (AUC) of 0.604 (95% confidence interval [95%CI]: 0.509-0.694) for women under 65 years of age, and of 0.642 (95%CI: 0.571-0.709) when age was not considered. Including data on muscle mass in the statistical analysis led to a significant improvement for the group of women under 65 years of age, with an AUC of 0,705 (95%CI: 0.612-0.786). The ability of the high-risk NOGG tool to identify T-scores ≤ -1.8 sd was limited.
Clinical muscle mass measurements increased the accuracy of the FRAX to screen for osteoporosis in women aged under 65 years.

Summary
Rev Bras Ginecol Obstet. 2020;42(1):26-34
To assess the construct and criterion validity of the Postmenopause Sexuality Questionnaire (PMSQ).
The present methodological questionnaire validation study included postmenopausal women. The construct validity was tested by factor analysis and the criterion validity was performed using the correlation between the PMSQ and the Female Sexual Function Index (FSFI). The ROC curve was used to verify sensitivity, specificity and to determine the cutoff point of the PMSQ.
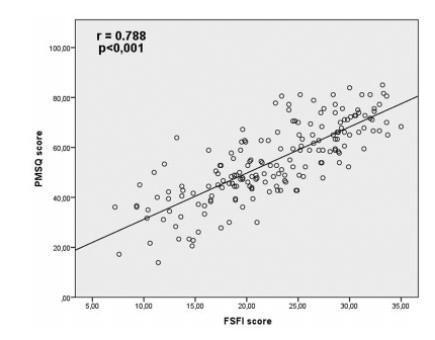
A total of 181 women with amean age of 56.4 ± 5.7 years old were evaluated. The exploratory factor analysis showed that the PMSQ presented Kaiser test = 0.88 and χ2 = 3293.7 (p < 0.001), commonalities ≥ 0.5, and extraction of 9 factors with eigenvalue ≥ 1; explaining 66.3% of the total variance. The PMSQ presented factor loadings between 0.4 and 0.8. A strong correlation between the 2 questionnaires (r = 0.79; p = 0.000) was shown. The cutoff point of the PMSQ was ≤ 55.5, assuming 87.9% sensitivity and 78.9% specificity (p < 0.001).
Since the PMSQ showed a strong correlation with the FSFI questionnaire, it presented good psychometric properties to assess the sexuality in postmenopausal women. Based on these results, the PMSQ could be widely tested as a specific instrument to examine the sexual function in postmenopausal women. Future studies, designed to examine the PMSQ instrument in different populations, are needed.
Summary
Rev Bras Ginecol Obstet. 2020;42(1):26-34
To assess the construct and criterion validity of the Postmenopause Sexuality Questionnaire (PMSQ).
The present methodological questionnaire validation study included postmenopausal women. The construct validity was tested by factor analysis and the criterion validity was performed using the correlation between the PMSQ and the Female Sexual Function Index (FSFI). The ROC curve was used to verify sensitivity, specificity and to determine the cutoff point of the PMSQ.
A total of 181 women with amean age of 56.4 ± 5.7 years old were evaluated. The exploratory factor analysis showed that the PMSQ presented Kaiser test = 0.88 and χ2 = 3293.7 (p < 0.001), commonalities ≥ 0.5, and extraction of 9 factors with eigenvalue ≥ 1; explaining 66.3% of the total variance. The PMSQ presented factor loadings between 0.4 and 0.8. A strong correlation between the 2 questionnaires (r = 0.79; p = 0.000) was shown. The cutoff point of the PMSQ was ≤ 55.5, assuming 87.9% sensitivity and 78.9% specificity (p < 0.001).
Since the PMSQ showed a strong correlation with the FSFI questionnaire, it presented good psychometric properties to assess the sexuality in postmenopausal women. Based on these results, the PMSQ could be widely tested as a specific instrument to examine the sexual function in postmenopausal women. Future studies, designed to examine the PMSQ instrument in different populations, are needed.
Summary
Rev Bras Ginecol Obstet. 2019;41(11):660-667
The incidence of obesity, which is a chronic condition, has increased in recent years. The association between obesity and female sexual dysfunction remains unclear, particularly in postmenopausal women. In the present study, we evaluated whether obesity is a risk factor for sexual dysfunction in postmenopausal women.
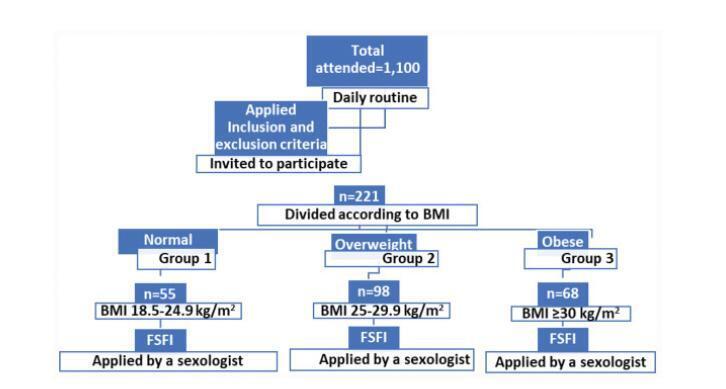
This is a cross-sectional study that analyzed data from interviews of postmenopausal women at the Climacteric Outpatient Clinic from 2015 to 2018. After applying the inclusion and exclusion criteria, 221 women aged between 40 and 65 years old were selected and invited to participate in the study. Obesity was diagnosed according to body mass index (BMI). The participants were grouped into the following BMI categories: group 1, 18.5-24.9 kg/m2 (normal); group 2, 25.0- 29.9 kg/m2 (overweight); and group 3, ≥30.0 kg/m2 (obese). Sexual function was assessed using the Female Sexual Function Index (FSFI) questionnaire. Cutoff points of ≥23 and ≥26.5 were adopted to define a diagnosis of female sexual dysfunction (FSD) based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision by the American Psychiatric Association (DSM-IV-TR).
The desire and arousal scores were statistically higher in the normal BMI group than in the obese group (p=0.028 and p=0.043, respectively). The satisfaction scores were statistically higher in the normal BMI group than in the overweight and obese groups (p<0.05). The total FSFI score statistically differed among the BMI categories (p=0.027).
In the present study, obese and overweight postmenopausal women had higher total scores than women with normal BMI. Our results show that obese and overweight postmenopausal women had a higher index of dysfunction in desire and arousal and lower sexual satisfaction than normal-weight women.
Summary
Rev Bras Ginecol Obstet. 2019;41(11):660-667
The incidence of obesity, which is a chronic condition, has increased in recent years. The association between obesity and female sexual dysfunction remains unclear, particularly in postmenopausal women. In the present study, we evaluated whether obesity is a risk factor for sexual dysfunction in postmenopausal women.
This is a cross-sectional study that analyzed data from interviews of postmenopausal women at the Climacteric Outpatient Clinic from 2015 to 2018. After applying the inclusion and exclusion criteria, 221 women aged between 40 and 65 years old were selected and invited to participate in the study. Obesity was diagnosed according to body mass index (BMI). The participants were grouped into the following BMI categories: group 1, 18.5-24.9 kg/m2 (normal); group 2, 25.0- 29.9 kg/m2 (overweight); and group 3, ≥30.0 kg/m2 (obese). Sexual function was assessed using the Female Sexual Function Index (FSFI) questionnaire. Cutoff points of ≥23 and ≥26.5 were adopted to define a diagnosis of female sexual dysfunction (FSD) based on the Diagnostic and Statistical Manual of Mental Disorders, 4th edition, Text Revision by the American Psychiatric Association (DSM-IV-TR).
The desire and arousal scores were statistically higher in the normal BMI group than in the obese group (p=0.028 and p=0.043, respectively). The satisfaction scores were statistically higher in the normal BMI group than in the overweight and obese groups (p<0.05). The total FSFI score statistically differed among the BMI categories (p=0.027).
In the present study, obese and overweight postmenopausal women had higher total scores than women with normal BMI. Our results show that obese and overweight postmenopausal women had a higher index of dysfunction in desire and arousal and lower sexual satisfaction than normal-weight women.
Summary
Rev Bras Ginecol Obstet. 2019;41(7):432-439
To validate the six-item female sexual function index (FSFI-6) in middleaged Brazilian women.
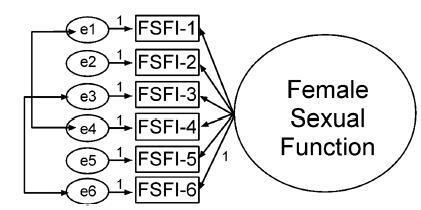
Cross-sectional observational study, involving 737 (premenopausal n = 117, perimenopausal n = 249, postmenopausal n = 371) Brazilian sexually active women, aged between 40 and 55 years, not using hormonal contraceptive methods. The Brazilian FSFI-6 was developed from the translation and cultural adaptation of the Portuguese FSFI-6 version. The participants completed a general questionnaire, the FSFI-6, and the menopause rating scale (MRS). The validation was performed by AMOS 16.0 software (SPSS, Inc., Chicago, IL, USA) for a confirmatory factor analysis (CFA). The chi-square of degrees of freedom (χ2/df), the comparative fit index (CFI), the Tucker- Lewis index (TLI) and the root-mean-square error of approximation (RMSEA) were used as indices of goodness of fit. Cronbach α coefficient was used for internal consistency.
The process of cultural adaptation has not altered the Brazilian FSFI-6, as compared with the original content. The CFA for the FSFI-6 score showed an acceptable fit (χ2/df = 3.434, CFI = 0.990, TLI = 0.980, RMSEA = 0.058, 90% confidence interval (90%CI) = 0.033-0.083, p ≤ 0.001) and a good reliability was established in FSFI-6 and MRS (Cronbach α = 0.840 and = 0.854, respectively). In addition, 53.5% of the sample had low sexual function.
The FSFI-6 was translated and adapted to the Brazilian culture and is a consistent and reliable tool for female sexual dysfunction screening in Brazilianmiddleaged women.
Summary
Rev Bras Ginecol Obstet. 2019;41(7):432-439
To validate the six-item female sexual function index (FSFI-6) in middleaged Brazilian women.
Cross-sectional observational study, involving 737 (premenopausal n = 117, perimenopausal n = 249, postmenopausal n = 371) Brazilian sexually active women, aged between 40 and 55 years, not using hormonal contraceptive methods. The Brazilian FSFI-6 was developed from the translation and cultural adaptation of the Portuguese FSFI-6 version. The participants completed a general questionnaire, the FSFI-6, and the menopause rating scale (MRS). The validation was performed by AMOS 16.0 software (SPSS, Inc., Chicago, IL, USA) for a confirmatory factor analysis (CFA). The chi-square of degrees of freedom (χ2/df), the comparative fit index (CFI), the Tucker- Lewis index (TLI) and the root-mean-square error of approximation (RMSEA) were used as indices of goodness of fit. Cronbach α coefficient was used for internal consistency.
The process of cultural adaptation has not altered the Brazilian FSFI-6, as compared with the original content. The CFA for the FSFI-6 score showed an acceptable fit (χ2/df = 3.434, CFI = 0.990, TLI = 0.980, RMSEA = 0.058, 90% confidence interval (90%CI) = 0.033-0.083, p ≤ 0.001) and a good reliability was established in FSFI-6 and MRS (Cronbach α = 0.840 and = 0.854, respectively). In addition, 53.5% of the sample had low sexual function.
The FSFI-6 was translated and adapted to the Brazilian culture and is a consistent and reliable tool for female sexual dysfunction screening in Brazilianmiddleaged women.
Search
Search in:
breast (42) breast cancer (42) breast neoplasms (95) Cesarean section (72) endometriosis (66) infertility (56) Maternal mortality (43) menopause (82) obesity (58) postpartum period (40) pregnancy (225) Pregnancy complications (99) Prenatal care (68) prenatal diagnosis (50) Prevalence (41) Quality of life (51) risk factors (94) ultrasonography (79) urinary incontinence (40) women's health (48)