Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo14
Postpartum hemorrhage (PPH) is the leading cause of maternal death globally. Therefore, prevention strategies have been created. The study aimed to evaluate the occurrence of PPH and its risk factors after implementing a risk stratification at admission in a teaching hospital.
A retrospective cohort involving a database of SISMATER® electronic medical record. Classification in low, medium, or high risk for PPH was performed through data filled out by the obstetrician-assistant. PPH frequency was calculated, compared among these groups and associated with the risk factors.
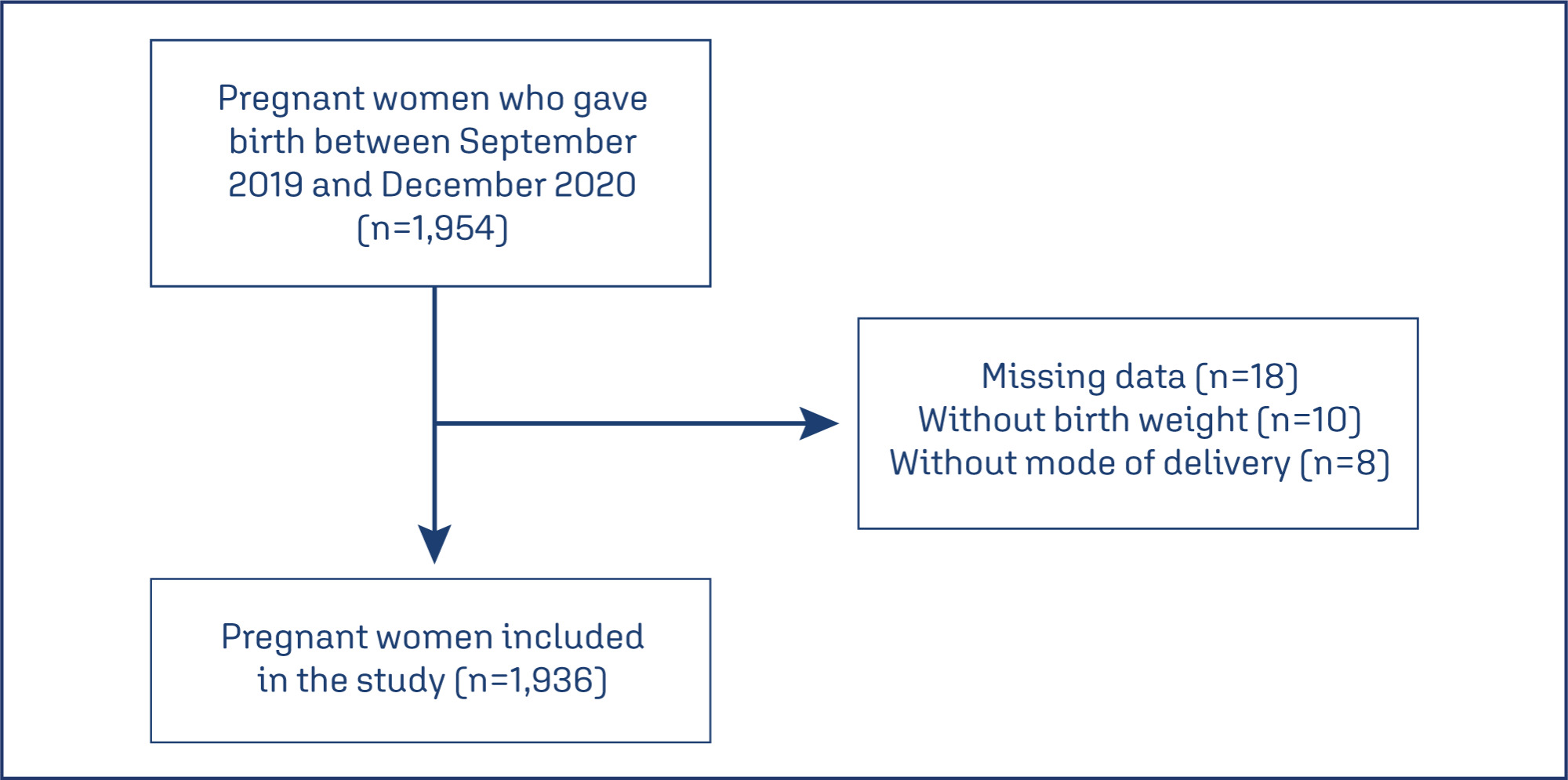
The prevalence of PPH was 6.8%, 131 among 1,936 women. Sixty-eight (51.9%) of them occurred in the high-risk group, 30 (22.9%) in the medium-risk and 33 (25.2%) in the low-risk group. The adjusted-odds ratio (OR) for PPH were analyzed using a confidence interval (95% CI) and was significantly higher in who presented multiple pregnancy (OR 2.88, 95% CI 1.28 to 6.49), active bleeding on admission (OR 6.12, 95% CI 1.20 to 4.65), non-cephalic presentation (OR 2.36, 95% CI 1.20 to 4.65), retained placenta (OR 9.39, 95% CI 2.90 to 30.46) and placental abruption (OR 6.95, 95% CI 2.06 to 23.48). Vaginal delivery figured out as a protective factor (OR 0.58, 95% CI 0.34 to 0.98).
Prediction of PPH is still a challenge since its unpredictable factor arrangements. The fact that the analysis did not demonstrate a relationship between risk category and frequency of PPH could be attributable to the efficacy of the strategy: Women classified as "high-risk" received adequate medical care, consequently.
Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo14
Postpartum hemorrhage (PPH) is the leading cause of maternal death globally. Therefore, prevention strategies have been created. The study aimed to evaluate the occurrence of PPH and its risk factors after implementing a risk stratification at admission in a teaching hospital.
A retrospective cohort involving a database of SISMATER® electronic medical record. Classification in low, medium, or high risk for PPH was performed through data filled out by the obstetrician-assistant. PPH frequency was calculated, compared among these groups and associated with the risk factors.
The prevalence of PPH was 6.8%, 131 among 1,936 women. Sixty-eight (51.9%) of them occurred in the high-risk group, 30 (22.9%) in the medium-risk and 33 (25.2%) in the low-risk group. The adjusted-odds ratio (OR) for PPH were analyzed using a confidence interval (95% CI) and was significantly higher in who presented multiple pregnancy (OR 2.88, 95% CI 1.28 to 6.49), active bleeding on admission (OR 6.12, 95% CI 1.20 to 4.65), non-cephalic presentation (OR 2.36, 95% CI 1.20 to 4.65), retained placenta (OR 9.39, 95% CI 2.90 to 30.46) and placental abruption (OR 6.95, 95% CI 2.06 to 23.48). Vaginal delivery figured out as a protective factor (OR 0.58, 95% CI 0.34 to 0.98).
Prediction of PPH is still a challenge since its unpredictable factor arrangements. The fact that the analysis did not demonstrate a relationship between risk category and frequency of PPH could be attributable to the efficacy of the strategy: Women classified as "high-risk" received adequate medical care, consequently.
Summary
Rev Bras Ginecol Obstet. 2023;45(3):134-141
This study assessed maternal mortality (MM) and related factors in a large-sized municipality in the Southeastern region of Brazil (Campinas, São Paulo) during the period 2000-2015.
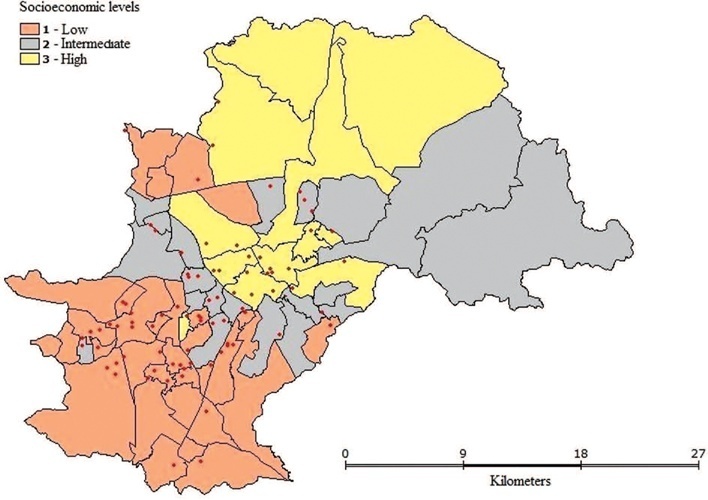
This study consisted of two phases: 1. An analytical nested case-control phase that assessed the impact of individual and contextual variables on MM; and 2. an ecological phase designed to contextualize maternal deaths by means of spatial analysis. The case group consisted of all maternal deaths (n = 87) and the control group consisted of 348 women who gave birth during the same period. Data analysis included descriptive statistics, association, and multiple logistic regression (MLR) tests at p < 0.05 as well as spatial analysis.
Maternal Mortality Ratio was 37 deaths per 100.000 live births. Deaths were dispersed throughout the urban territory and no formation of cluster was observed. MLR showed that pregnant women aged > 35 years old (OR = 2.63) or those with cesarean delivery (OR = 2.51) were more prone to maternal death.
Maternal deaths were distributed dispersedly among the different socioeconomic levels and more prone to occur among older women or those undergoing cesarean deliveries.
Summary
Rev Bras Ginecol Obstet. 2023;45(3):134-141
This study assessed maternal mortality (MM) and related factors in a large-sized municipality in the Southeastern region of Brazil (Campinas, São Paulo) during the period 2000-2015.
This study consisted of two phases: 1. An analytical nested case-control phase that assessed the impact of individual and contextual variables on MM; and 2. an ecological phase designed to contextualize maternal deaths by means of spatial analysis. The case group consisted of all maternal deaths (n = 87) and the control group consisted of 348 women who gave birth during the same period. Data analysis included descriptive statistics, association, and multiple logistic regression (MLR) tests at p < 0.05 as well as spatial analysis.
Maternal Mortality Ratio was 37 deaths per 100.000 live births. Deaths were dispersed throughout the urban territory and no formation of cluster was observed. MLR showed that pregnant women aged > 35 years old (OR = 2.63) or those with cesarean delivery (OR = 2.51) were more prone to maternal death.
Maternal deaths were distributed dispersedly among the different socioeconomic levels and more prone to occur among older women or those undergoing cesarean deliveries.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):593-601
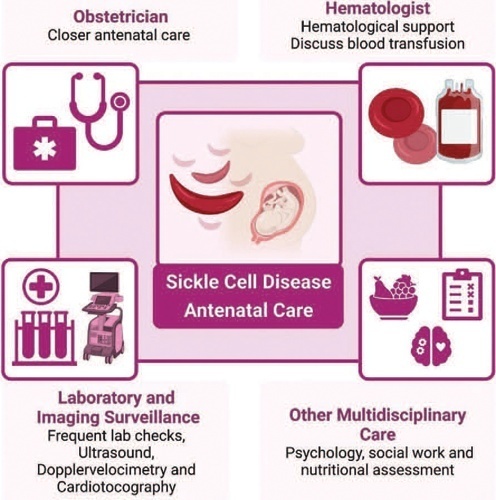
Sickle cell disease (SCD) is the most common monogenic disease worldwide, with a variable prevalence in each continent. A single nucleotide substitution leads to an amino-acid change in the β-globin chain, altering the normal structure of hemoglobin, which is then called hemoglobin S inherited in homozygosity (HbSS) or double heterozygosity (HbSC, HbSβ), and leads to chronic hemolysis, vaso-occlusion, inflammation, and endothelium activation. Pregnant women with SCD are at a higher risk of developing maternal and perinatal complications. We performed a narrative review of the literature considering SCD and pregnancy, the main clinical and obstetrical complications, the specific antenatal care, and the follow-up for maternal and fetal surveillance. Pregnant women with SCD are at a higher risk of developing clinical and obstetric complications such as pain episodes, pulmonary complications, infections, thromboembolic events, preeclampsia, and maternal death. Their newborns are also at an increased risk of developing neonatal complications: fetal growth restriction, preterm birth, stillbirth. Severe complications can occur in patients of any genotype. We concluded that SCD is a high-risk condition that increases maternal and perinatal morbidity and mortality. A multidisciplinary approach during pregnancy and the postpartum period is key to adequately diagnose and treat complications.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):593-601
Sickle cell disease (SCD) is the most common monogenic disease worldwide, with a variable prevalence in each continent. A single nucleotide substitution leads to an amino-acid change in the β-globin chain, altering the normal structure of hemoglobin, which is then called hemoglobin S inherited in homozygosity (HbSS) or double heterozygosity (HbSC, HbSβ), and leads to chronic hemolysis, vaso-occlusion, inflammation, and endothelium activation. Pregnant women with SCD are at a higher risk of developing maternal and perinatal complications. We performed a narrative review of the literature considering SCD and pregnancy, the main clinical and obstetrical complications, the specific antenatal care, and the follow-up for maternal and fetal surveillance. Pregnant women with SCD are at a higher risk of developing clinical and obstetric complications such as pain episodes, pulmonary complications, infections, thromboembolic events, preeclampsia, and maternal death. Their newborns are also at an increased risk of developing neonatal complications: fetal growth restriction, preterm birth, stillbirth. Severe complications can occur in patients of any genotype. We concluded that SCD is a high-risk condition that increases maternal and perinatal morbidity and mortality. A multidisciplinary approach during pregnancy and the postpartum period is key to adequately diagnose and treat complications.
Summary
Rev Bras Ginecol Obstet. 2021;43(9):655-661
To describe the clinical experience with the B-Lynch technique in the management of postpartum hemorrhage as well as the factors related to the indication of the technique and to present the success rates of the application of the B-Lynch technique.
Observational, retrospective, cross-sectional, and analytical study. Patient data was obtained through the study of medical records. The study population comprised of patients who underwent hemostatic suture using the B-Lynch technique, including 104 patients within the period from January 1, 2005, to December 31, 2019.
Of the total of 104 patients, 82.7% did not present any complications. Blood transfusion and intensive care unit admission were the most prevalent complications, with 13.5% and 15.4%, respectively. Only 1% of the patients had puerperal and surgical site infections. The factors most related to the application of the technique were the presence of previous cesarean section (30.8%), use of oxytocin (16.3%), and pre-eclampsia (11.6%). Puerperal hysterectomy was performed in 4.8% of the patients due to failure of the method.
The clinical experience with the B-Lynch technique was satisfactory since it presented few complications, with excellent results in hemorrhagic control. Previous cesarean section, the use of oxytocin, and preeclampsia stood out as factors related to the indication of the application of the technique, and the success rate in controlling postpartum hemorrhage was 95.2%.
Summary
Rev Bras Ginecol Obstet. 2021;43(9):655-661
To describe the clinical experience with the B-Lynch technique in the management of postpartum hemorrhage as well as the factors related to the indication of the technique and to present the success rates of the application of the B-Lynch technique.
Observational, retrospective, cross-sectional, and analytical study. Patient data was obtained through the study of medical records. The study population comprised of patients who underwent hemostatic suture using the B-Lynch technique, including 104 patients within the period from January 1, 2005, to December 31, 2019.
Of the total of 104 patients, 82.7% did not present any complications. Blood transfusion and intensive care unit admission were the most prevalent complications, with 13.5% and 15.4%, respectively. Only 1% of the patients had puerperal and surgical site infections. The factors most related to the application of the technique were the presence of previous cesarean section (30.8%), use of oxytocin (16.3%), and pre-eclampsia (11.6%). Puerperal hysterectomy was performed in 4.8% of the patients due to failure of the method.
The clinical experience with the B-Lynch technique was satisfactory since it presented few complications, with excellent results in hemorrhagic control. Previous cesarean section, the use of oxytocin, and preeclampsia stood out as factors related to the indication of the application of the technique, and the success rate in controlling postpartum hemorrhage was 95.2%.
Summary
Rev Bras Ginecol Obstet. 2021;43(9):662-668
To determine the profile of maternal deaths occurred in the period between 2000 and 2019 in the Hospital de Clínicas de Porto Alegre (HCPA, in the Portuguese acronym) and to compare it with maternal deaths between 1980 and 1999 in the same institution.
Retrospective study that analyzed 2,481 medical records of women between 10 and 49 years old who died between 2000 and 2018. The present study was approved by the Ethics Committee (CAAE 78021417600005327).
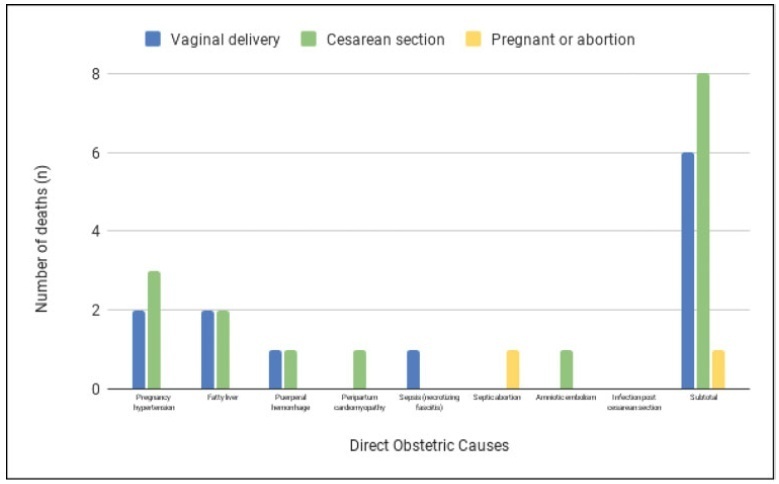
After reviewing 2,481 medical records of women who died in reproductive age, 43 deaths had occurred during pregnancy or in the postpartum period. Of these, 28 were considered maternal deaths. The maternal mortality ratio was 37.6 per 100,000 live births. Regarding causes, 16 deaths (57.1%) were directly associated with pregnancy, 10 (35.1%) were indirectly associated, and 2 (7.1%) were unrelated. The main cause of death was hypertension during pregnancy (31.2%) followed by acute liver steatosis during pregnancy (25%). In the previous study, published in 2003 in the same institution4, the mortality rate was 129 per 100,000 live births, and most deaths were related to direct obstetric causes (62%). The main causes of death in this period were due to hypertensive complications (17.2%), followed by postcesarean infection (16%).
Compared with data before the decade of 2000, there was an important reduction in maternal deaths due to infectious causes.
Summary
Rev Bras Ginecol Obstet. 2021;43(9):662-668
To determine the profile of maternal deaths occurred in the period between 2000 and 2019 in the Hospital de Clínicas de Porto Alegre (HCPA, in the Portuguese acronym) and to compare it with maternal deaths between 1980 and 1999 in the same institution.
Retrospective study that analyzed 2,481 medical records of women between 10 and 49 years old who died between 2000 and 2018. The present study was approved by the Ethics Committee (CAAE 78021417600005327).
After reviewing 2,481 medical records of women who died in reproductive age, 43 deaths had occurred during pregnancy or in the postpartum period. Of these, 28 were considered maternal deaths. The maternal mortality ratio was 37.6 per 100,000 live births. Regarding causes, 16 deaths (57.1%) were directly associated with pregnancy, 10 (35.1%) were indirectly associated, and 2 (7.1%) were unrelated. The main cause of death was hypertension during pregnancy (31.2%) followed by acute liver steatosis during pregnancy (25%). In the previous study, published in 2003 in the same institution4, the mortality rate was 129 per 100,000 live births, and most deaths were related to direct obstetric causes (62%). The main causes of death in this period were due to hypertensive complications (17.2%), followed by postcesarean infection (16%).
Compared with data before the decade of 2000, there was an important reduction in maternal deaths due to infectious causes.
Summary
Rev Bras Ginecol Obstet. 2021;43(3):158-164
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
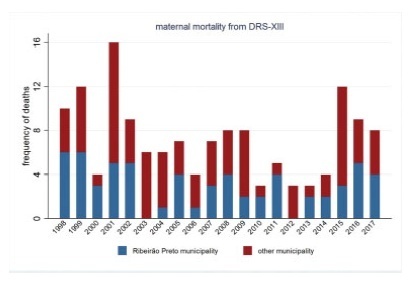
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
Rev Bras Ginecol Obstet. 2021;43(3):158-164
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
Rev Bras Ginecol Obstet. 2021;43(2):113-118
To identify risk factors related to postpartum hemorrhage (PPH) and severe PPH with blood loss quantified objectively.
This is a complementary analysis of a prospective cohort study that included pregnant women delivering vaginally. The total blood loss was obtained through the sum of the volume collected from the drape with the weight of gauzes, compresses and pads used by women within 2 hours. Exploratory data analysis was performed to assess mean, standard deviation (SD), frequency, percentage and percentiles. The risk factors for postpartum bleeding were evaluated using linear and logistic regression.
We included 270 women. Themean blood loss at 120 minutes was 427.49 mL (±335.57 mL). Thirty-one percent (84 women) bled > 500mL and 8.2% (22 women) bled > 1,000 mL within 2 hours. Episiotomy, longer second stage of labor and forceps delivery were related to blood loss > 500mL within 2 hours, in the univariate analysis. In the multivariate analysis, only forceps remained associated with bleeding > 500 mL within 2 hours (odds ratio [OR] = 9.5 [2.85-31.53]). Previous anemia and episiotomy were also related to blood loss > 1,000mL.
Prolonged second stage of labor, forceps and episiotomy are related to increased incidence of PPH, and should be used as an alert for the delivery assistants for early recognition and prompt treatment for PPH.
Summary
Rev Bras Ginecol Obstet. 2021;43(2):113-118
To identify risk factors related to postpartum hemorrhage (PPH) and severe PPH with blood loss quantified objectively.
This is a complementary analysis of a prospective cohort study that included pregnant women delivering vaginally. The total blood loss was obtained through the sum of the volume collected from the drape with the weight of gauzes, compresses and pads used by women within 2 hours. Exploratory data analysis was performed to assess mean, standard deviation (SD), frequency, percentage and percentiles. The risk factors for postpartum bleeding were evaluated using linear and logistic regression.
We included 270 women. Themean blood loss at 120 minutes was 427.49 mL (±335.57 mL). Thirty-one percent (84 women) bled > 500mL and 8.2% (22 women) bled > 1,000 mL within 2 hours. Episiotomy, longer second stage of labor and forceps delivery were related to blood loss > 500mL within 2 hours, in the univariate analysis. In the multivariate analysis, only forceps remained associated with bleeding > 500 mL within 2 hours (odds ratio [OR] = 9.5 [2.85-31.53]). Previous anemia and episiotomy were also related to blood loss > 1,000mL.
Prolonged second stage of labor, forceps and episiotomy are related to increased incidence of PPH, and should be used as an alert for the delivery assistants for early recognition and prompt treatment for PPH.
Search
Search in:
breast (42) breast cancer (42) breast neoplasms (95) Cesarean section (72) endometriosis (66) infertility (56) Maternal mortality (43) menopause (82) obesity (58) postpartum period (40) pregnancy (225) Pregnancy complications (99) Prenatal care (68) prenatal diagnosis (50) Prevalence (41) Quality of life (51) risk factors (94) ultrasonography (79) urinary incontinence (40) women's health (48)