Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2025;47:e-rbgo4
03-18-2025
This study aimed to verify the relation between gastrin-releasing peptide receptor (GRPR), oncogenic Human Papillomavirus (HPV) and cervical lesions severity.
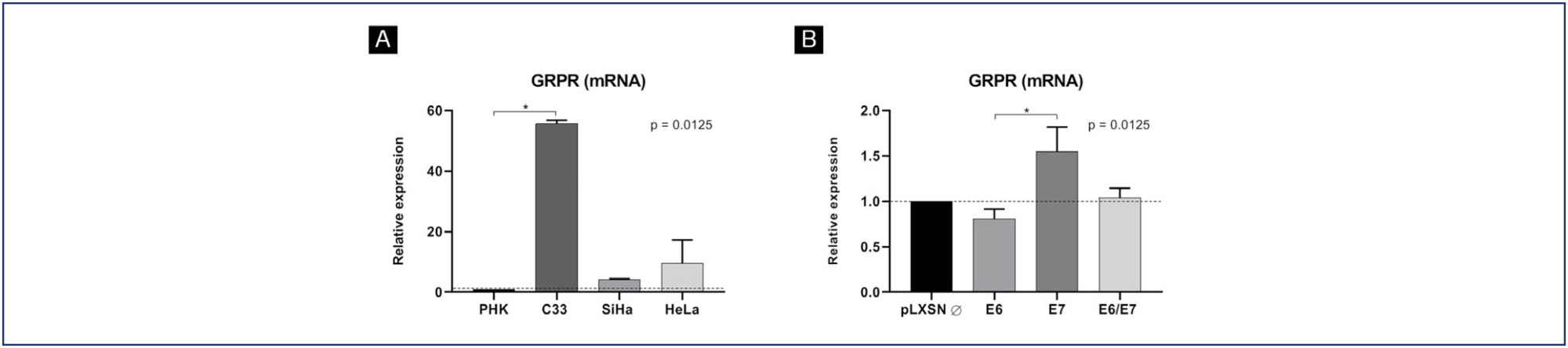
GRPR mRNA levels were evaluated in cervical cancer-derived cell lines and in primary keratinocytes expressing HPV16 oncogenes by RT-PCR. GRPR protein expression was assessed by immunohistochemistry in organotypic cell cultures derived from keratinocytes transduced with HPV16 oncogenes and in 208 cervical samples, including 59 non-neoplastic tissue, 28 cervical intraepithelial neoplasia grade 3 (CIN3), 44 squamous cell carcinomas (SCC) and 77 adenocarcinomas (ADC). Generic primers (GP5+/GP6+) were used to identify HPV infection in tissue samples. Experiments involving cell lines were analyzed through non-parametric tests (Kruskal Wallis), and Fisher's Exact Test for human tissues samples. All statistical tests were considered significant at p <0.05. Immunohistochemical evaluation was conducted independently and blindly by two observers (AD- LO). Any discordant findings were resolved through discussion to reach a consensus score.
GRPR mRNA levels were not increased in cells expressing HPV16 or HPV18 oncogenes. However, at the protein level, GRPR was upregulated in organotypic cell cultures containing HPV oncogenes. Besides, it was identified an association between GRPR expression and cervical lesion severity (p < 0.0001). The detection rate of high-risk HPV DNA was directly correlated with cervical disease. Nonetheless, HPV infection was not directly associated with GRPR in cervical samples.
GRPR expression is highly predictive of cervical lesion severity, irrespective of HPV infection and might contribute to improving patient's therapeutic management as well as being used a marker of disease progression.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2025;47:e-rbgo4
03-18-2025
This study aimed to verify the relation between gastrin-releasing peptide receptor (GRPR), oncogenic Human Papillomavirus (HPV) and cervical lesions severity.
GRPR mRNA levels were evaluated in cervical cancer-derived cell lines and in primary keratinocytes expressing HPV16 oncogenes by RT-PCR. GRPR protein expression was assessed by immunohistochemistry in organotypic cell cultures derived from keratinocytes transduced with HPV16 oncogenes and in 208 cervical samples, including 59 non-neoplastic tissue, 28 cervical intraepithelial neoplasia grade 3 (CIN3), 44 squamous cell carcinomas (SCC) and 77 adenocarcinomas (ADC). Generic primers (GP5+/GP6+) were used to identify HPV infection in tissue samples. Experiments involving cell lines were analyzed through non-parametric tests (Kruskal Wallis), and Fisher's Exact Test for human tissues samples. All statistical tests were considered significant at p <0.05. Immunohistochemical evaluation was conducted independently and blindly by two observers (AD- LO). Any discordant findings were resolved through discussion to reach a consensus score.
GRPR mRNA levels were not increased in cells expressing HPV16 or HPV18 oncogenes. However, at the protein level, GRPR was upregulated in organotypic cell cultures containing HPV oncogenes. Besides, it was identified an association between GRPR expression and cervical lesion severity (p < 0.0001). The detection rate of high-risk HPV DNA was directly correlated with cervical disease. Nonetheless, HPV infection was not directly associated with GRPR in cervical samples.
GRPR expression is highly predictive of cervical lesion severity, irrespective of HPV infection and might contribute to improving patient's therapeutic management as well as being used a marker of disease progression.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo86
12-04-2024
HPV infection is considered the most common sexually transmitted virus today. The persistence of HPV is the main cause for the development of precursor lesions and cervical cancer. There are environmental and non-environmental factors that contribute to the persistence of the virus. Studies indicate a possible relationship between the vaginal microbiota (environmental factor) and the risk of high-grade cervical squamous intraepithelial lesions and cervical cancer. This study evaluates the association between the type of vaginal microbiota and the occurrence of high-grade squamous intraepithelial lesions of the cervix.
Observational, longitudinal, prospective, and analytical studies carried out between 2019 and 2021, which evaluated the vaginal microbiota of patients diagnosed with high-grade cervical squamous intraepithelial lesion before and after treatment in two collections with an interval of 6 months, using scrapings and vaginal swabs.
In Group I (with lesions) 28 women participated and 29 in Group II (without lesions). According to Nugent, in the initial collection of Group I, 16 women (57%) had lactobacillary microbiota, eight (28%) intermediate, and four (14%) coccus. In Group II, twenty-one (75%) were lactobacillary, one (3%) was intermediate, and seven (24%) werecoccus. With p=0.03.
According to Nugent's criteria, there was an association between the type of vaginal microbiota and the occurrence of high-grade cervical squamous intraepithelial lesions of the cervix. The same was not observed in the Donders classification. Studies with a larger sample are needed to confirm our results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo86
12-04-2024
HPV infection is considered the most common sexually transmitted virus today. The persistence of HPV is the main cause for the development of precursor lesions and cervical cancer. There are environmental and non-environmental factors that contribute to the persistence of the virus. Studies indicate a possible relationship between the vaginal microbiota (environmental factor) and the risk of high-grade cervical squamous intraepithelial lesions and cervical cancer. This study evaluates the association between the type of vaginal microbiota and the occurrence of high-grade squamous intraepithelial lesions of the cervix.
Observational, longitudinal, prospective, and analytical studies carried out between 2019 and 2021, which evaluated the vaginal microbiota of patients diagnosed with high-grade cervical squamous intraepithelial lesion before and after treatment in two collections with an interval of 6 months, using scrapings and vaginal swabs.
In Group I (with lesions) 28 women participated and 29 in Group II (without lesions). According to Nugent, in the initial collection of Group I, 16 women (57%) had lactobacillary microbiota, eight (28%) intermediate, and four (14%) coccus. In Group II, twenty-one (75%) were lactobacillary, one (3%) was intermediate, and seven (24%) werecoccus. With p=0.03.
According to Nugent's criteria, there was an association between the type of vaginal microbiota and the occurrence of high-grade cervical squamous intraepithelial lesions of the cervix. The same was not observed in the Donders classification. Studies with a larger sample are needed to confirm our results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo85
10-23-2024
To evaluate the role of being human immunodeficiency virus (HIV) positive for predicting the risk of recurrence in women with a cervical high grade squamous intraepithelial lesion (HSIL) diagnosis.
Retrospective observational case-control study, comprising HIV positive (case) and HIV negative (control) women in a 1:4 ratio. Women assisted by the Erasto Gaertner Hospital, between 2009-2018, with cervical HSIL diagnosis, submitted to treatment by Loop electrosurgical excision procedure (LEEP), and with a minimum follow-up of 18 months, were included. The immunological status, number and time to recurrence were analyzed, with p<0.05 considered significant. In a second analysis, only patients with free margins were evaluated.
The sample consisted of 320 women (64 cases and 256 controls). Presence of HIV, CD4 levels <200 and detectable viral load (CV) were associated with high risk of recurrence, with odds ratio (OR) of 5.4 (p<0.001/95CI:2.8-10); 3.6 (p<0.001 /IC95:0.6-21.1) and 1.8 (p=0.039 /IC95:0.3-9.3), respectively. In the sample with free margins (n=271), this risk was also higher among seropositive patients, with OR 4.18 (p=0.001/95CI:1.8-9.2).
HIV is an independent risk factor for cervical HSIL recurrence and reduced disease-free survival time. Glandular involvement, compromised margins, undetectable CV and CD4<200 also increase the risk of relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo85
10-23-2024
To evaluate the role of being human immunodeficiency virus (HIV) positive for predicting the risk of recurrence in women with a cervical high grade squamous intraepithelial lesion (HSIL) diagnosis.
Retrospective observational case-control study, comprising HIV positive (case) and HIV negative (control) women in a 1:4 ratio. Women assisted by the Erasto Gaertner Hospital, between 2009-2018, with cervical HSIL diagnosis, submitted to treatment by Loop electrosurgical excision procedure (LEEP), and with a minimum follow-up of 18 months, were included. The immunological status, number and time to recurrence were analyzed, with p<0.05 considered significant. In a second analysis, only patients with free margins were evaluated.
The sample consisted of 320 women (64 cases and 256 controls). Presence of HIV, CD4 levels <200 and detectable viral load (CV) were associated with high risk of recurrence, with odds ratio (OR) of 5.4 (p<0.001/95CI:2.8-10); 3.6 (p<0.001 /IC95:0.6-21.1) and 1.8 (p=0.039 /IC95:0.3-9.3), respectively. In the sample with free margins (n=271), this risk was also higher among seropositive patients, with OR 4.18 (p=0.001/95CI:1.8-9.2).
HIV is an independent risk factor for cervical HSIL recurrence and reduced disease-free survival time. Glandular involvement, compromised margins, undetectable CV and CD4<200 also increase the risk of relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo44
06-03-2024
To describe Top-hat results and their association with margin status and disease relapse in a referral facility in Brazil.
A retrospective study of 440 women submitted to LEEP to treat HSIL, in which 80 cases were complemented immediately by the top hat procedure (Top-hat Group - TH). TH Group was compared to women not submitted to Top-hat (NTH). The sample by convenience included all women that underwent LEEP from January 2017 to July 2020. The main outcome was the histological result. Other variables were margins, age, transformation zone (TZ), depth, and relapse. The analysis used the Chi-square test and logistic regression.
The TH Group was predominantly 40 and older (NTH 23.1% vs. TH 65.0%, p<0.001). No difference was found in having CIN2/CIN3 as the final diagnosis (NTH 17.0% vs. TH 21.3%, p=0.362), or in the prevalence of relapse (NTH 12.0% vs. TH 9.0%, p=0.482). Of the 80 patients submitted to top hat, the histological result was CIN2/CIN3 in eight. A negative top hat result was related to a negative endocervical margin of 83.3%. A CIN2/CIN3 Top-hat result was related to CIN2/CIN3 margin in 62.5% (p=0.009). The chance of obtaining a top hat negative result was 22.4 times higher (2.4-211.0) when the endocervical margin was negative and 14.5 times higher (1.5-140.7) when the ectocervical margin was negative.
The top hat procedure did not alter the final diagnosis of LEEP. No impact on relapse was observed. The procedure should be avoided in women of reproductive age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo44
06-03-2024
To describe Top-hat results and their association with margin status and disease relapse in a referral facility in Brazil.
A retrospective study of 440 women submitted to LEEP to treat HSIL, in which 80 cases were complemented immediately by the top hat procedure (Top-hat Group - TH). TH Group was compared to women not submitted to Top-hat (NTH). The sample by convenience included all women that underwent LEEP from January 2017 to July 2020. The main outcome was the histological result. Other variables were margins, age, transformation zone (TZ), depth, and relapse. The analysis used the Chi-square test and logistic regression.
The TH Group was predominantly 40 and older (NTH 23.1% vs. TH 65.0%, p<0.001). No difference was found in having CIN2/CIN3 as the final diagnosis (NTH 17.0% vs. TH 21.3%, p=0.362), or in the prevalence of relapse (NTH 12.0% vs. TH 9.0%, p=0.482). Of the 80 patients submitted to top hat, the histological result was CIN2/CIN3 in eight. A negative top hat result was related to a negative endocervical margin of 83.3%. A CIN2/CIN3 Top-hat result was related to CIN2/CIN3 margin in 62.5% (p=0.009). The chance of obtaining a top hat negative result was 22.4 times higher (2.4-211.0) when the endocervical margin was negative and 14.5 times higher (1.5-140.7) when the ectocervical margin was negative.
The top hat procedure did not alter the final diagnosis of LEEP. No impact on relapse was observed. The procedure should be avoided in women of reproductive age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(12):790-795
01-11-2023
To compare cytological and histological results from women > 64 years old who followed the Brazilian national cervical cancer screening guidelines with those who did not.
The present observational retrospective study analyzed 207 abnormal cervical smear results from women > 64 years old in a mid-sized city in Brazil over 14 years. All results were reported according to the Bethesda System. The women were divided into those who followed the screening guidelines and those who did not.
Atypical squamous cells of undetermined significance and low-grade squamous intraepithelial lesion cytology results were found in 128 (62.2%) cases. Of these, 112 (87.5%) had repeated cytology with positive results. The other 79 (38.1%) with abnormal results should have been referred to colposcopy and biopsy. Out of 41 (51.9%) biopsied women, 23 (29.1%) had a confirmed diagnosis of neoplasia or precursor lesion. In contrast, among the 78 (37.7%) biopsied patients, 40 (51.3%) followed the guideline recommendations, with 9 (22.5%) positive biopsies. Of the 38 (48.7%) women who did not follow the guidelines, there were 24 (63.1%) positive results. Women who did not follow the guidelines demonstrated higher chances of cancer and precursor lesions (odds ratio [OR]: 5.904; 95% confidence interval [CI]: 2.188–15.932; p = 0.0002).
Women > 64 years old who did not follow the national screening protocol showed significant differences in the frequency of abnormal results and severity of diagnosis compared with those who followed the protocol.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(12):790-795
01-11-2023
To compare cytological and histological results from women > 64 years old who followed the Brazilian national cervical cancer screening guidelines with those who did not.
The present observational retrospective study analyzed 207 abnormal cervical smear results from women > 64 years old in a mid-sized city in Brazil over 14 years. All results were reported according to the Bethesda System. The women were divided into those who followed the screening guidelines and those who did not.
Atypical squamous cells of undetermined significance and low-grade squamous intraepithelial lesion cytology results were found in 128 (62.2%) cases. Of these, 112 (87.5%) had repeated cytology with positive results. The other 79 (38.1%) with abnormal results should have been referred to colposcopy and biopsy. Out of 41 (51.9%) biopsied women, 23 (29.1%) had a confirmed diagnosis of neoplasia or precursor lesion. In contrast, among the 78 (37.7%) biopsied patients, 40 (51.3%) followed the guideline recommendations, with 9 (22.5%) positive biopsies. Of the 38 (48.7%) women who did not follow the guidelines, there were 24 (63.1%) positive results. Women who did not follow the guidelines demonstrated higher chances of cancer and precursor lesions (odds ratio [OR]: 5.904; 95% confidence interval [CI]: 2.188–15.932; p = 0.0002).
Women > 64 years old who did not follow the national screening protocol showed significant differences in the frequency of abnormal results and severity of diagnosis compared with those who followed the protocol.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(11):689-698
12-05-2023
The present study aims to establish a risk profile for high-grade cervical lesions and cervical cancer (CIN2 + ) in women undergoing colposcopy at the Hospital do Câncer de Barretos, through the analysis of Human Papillomavirus (HPV) infection, cervical cytology, and patient's age.
Retrospective cross-sectional study based on a computerized database of women aged ≥ 18 years old who underwent colposcopy at the Prevention Department of the Hospital do Câncer de Barretos from 2017 to 2019.
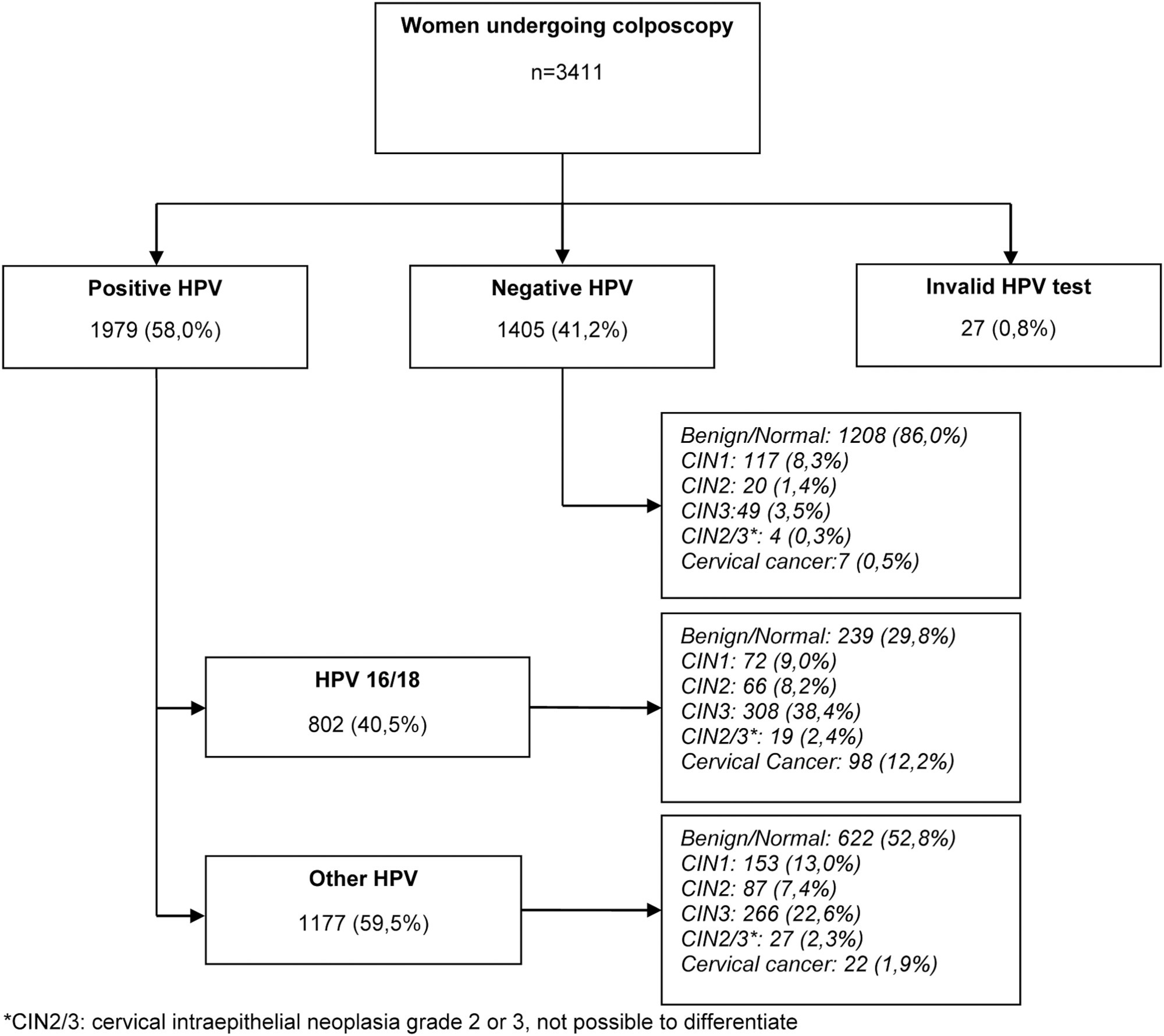
A total of 3,411 women were included, 58.0% were positive for high-risk-HPV test, with a higher prevalence of CIN2+ for HPV16 (30.3%) and other HPV (45.0%). Cytological findings that suggest invasive cervical cancer (squamous cells or adenocarcinoma), regardless of the status of HPV test, showed 100% diagnosis of CIN2 + , while atypias that suggest high-grade lesions, HSIL and ASC-H, positive for HPV test, showed in 86 and 55.2%, respectively, diagnosis of CIN2 + . ASC-H cytological results among women aged > 40 years old and negative HPV were mainly associated with benign findings. We observed that ≤ CIN1 has a higher prevalence among older women with negative HPV, while for high-grade lesions there is an increase among young women HPV16- and/or 18-positive. In cancer diagnosis, we observed a predominance of HPV 16/18 regardless of the age group.
The highest risks of precursor lesions and cervical cancer were found among women with positive HPV 16/18 tests and severe cytological atypia in population screening tests. In addition, cytological findings of ASC-H HPV negative in women > 40 years old usually represent benign findings in histological investigation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(11):689-698
12-05-2023
The present study aims to establish a risk profile for high-grade cervical lesions and cervical cancer (CIN2 + ) in women undergoing colposcopy at the Hospital do Câncer de Barretos, through the analysis of Human Papillomavirus (HPV) infection, cervical cytology, and patient's age.
Retrospective cross-sectional study based on a computerized database of women aged ≥ 18 years old who underwent colposcopy at the Prevention Department of the Hospital do Câncer de Barretos from 2017 to 2019.
A total of 3,411 women were included, 58.0% were positive for high-risk-HPV test, with a higher prevalence of CIN2+ for HPV16 (30.3%) and other HPV (45.0%). Cytological findings that suggest invasive cervical cancer (squamous cells or adenocarcinoma), regardless of the status of HPV test, showed 100% diagnosis of CIN2 + , while atypias that suggest high-grade lesions, HSIL and ASC-H, positive for HPV test, showed in 86 and 55.2%, respectively, diagnosis of CIN2 + . ASC-H cytological results among women aged > 40 years old and negative HPV were mainly associated with benign findings. We observed that ≤ CIN1 has a higher prevalence among older women with negative HPV, while for high-grade lesions there is an increase among young women HPV16- and/or 18-positive. In cancer diagnosis, we observed a predominance of HPV 16/18 regardless of the age group.
The highest risks of precursor lesions and cervical cancer were found among women with positive HPV 16/18 tests and severe cytological atypia in population screening tests. In addition, cytological findings of ASC-H HPV negative in women > 40 years old usually represent benign findings in histological investigation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(5):235-241
08-07-2023
To evaluate the accuracy and patient acceptability toward self-sampling using a new device - SelfCervix® - for detecting HPV-DNA.
A total of 73 women aged 25–65 who underwent regular cervical cancer screening from March to October 2016 were included. Women performed self-sampling followed by a physician-sampling, and the samples were analyzed for HPV-DNA. After that, patients were surveyed about their acceptability of self-sampling.
HPV-DNA detection rate of self-sampling presented high accuracy and was similar to physician-collection. Sixty-four (87.7%) patients answered the acceptability survey. Most patients (89%) considered the self-sampling comfortable, and 82.5% preferred self-sampling to physician-sampling. The reasons cited were time-saving and convenience. Fifty-one (79.7%) reported that they would recommend self-sampling.
Self-sampling using the new Brazilian device SelfCervix® is not inferior in HPV-DNA detection rate compared with physician-collection, and patients are supportive of the method. Therefore, it might be an option to reach under-screened populations in Brazil.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(5):235-241
08-07-2023
To evaluate the accuracy and patient acceptability toward self-sampling using a new device - SelfCervix® - for detecting HPV-DNA.
A total of 73 women aged 25–65 who underwent regular cervical cancer screening from March to October 2016 were included. Women performed self-sampling followed by a physician-sampling, and the samples were analyzed for HPV-DNA. After that, patients were surveyed about their acceptability of self-sampling.
HPV-DNA detection rate of self-sampling presented high accuracy and was similar to physician-collection. Sixty-four (87.7%) patients answered the acceptability survey. Most patients (89%) considered the self-sampling comfortable, and 82.5% preferred self-sampling to physician-sampling. The reasons cited were time-saving and convenience. Fifty-one (79.7%) reported that they would recommend self-sampling.
Self-sampling using the new Brazilian device SelfCervix® is not inferior in HPV-DNA detection rate compared with physician-collection, and patients are supportive of the method. Therefore, it might be an option to reach under-screened populations in Brazil.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
06-30-2023
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
06-30-2023
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.