-
Review Article03-18-2025
Clinical repercussions of statin use during pregnancy: a review of the literature
- Joan Lins Serafim
 ,
, - Pedro Lucas Santos de Menezes Teles ,
- Amanda Katharinne Souza Lima ,
- Jéssica dos Santos Coelho ,
- Paloma Luna Maranhão Conrado , [ ... ],
- George Alessandro Maranhão Conrado
Abstract
Review ArticleClinical repercussions of statin use during pregnancy: a review of the literature
Revista Brasileira de Ginecologia e Obstetrícia. 2025;47:e-rbgo2
- Joan Lins Serafim ,
- Pedro Lucas Santos de Menezes Teles ,
- Amanda Katharinne Souza Lima ,
- Jéssica dos Santos Coelho ,
- Paloma Luna Maranhão Conrado ,
- Valda Lúcia Moreira Luna ,
- Pauliana Valéria Machado Galvão ,
- George Alessandro Maranhão Conrado
Views144Abstract
Statins are the most widely used pharmacological class for treating hyperlipidemia, although they are contraindicated during pregnancy. This study aims to demonstrate the clinical effects of statins in pregnant women through an interactive review. Fifteen original articles were selected, in English or Portuguese, within of five years. Statins have not been associated with the development of fetal malformations and their use may be useful in preventing unfavorable cardiovascular outcomes, with the potential to reduce oxidative stress and angiogenic dysfunction. However, the use of statins to prevent pre-eclampsia in humans has not been properly clarified and further studies are needed. Pravastatin is considered safer than statins for use during pregnancy.
Key-words Antihypertensive agentsHydroxymethylglutaryl-CoA reductase inhibitorsPravastatinPre-eclampsiaPregnancyPregnant womanSee moreViews144

This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Review ArticleClinical repercussions of statin use during pregnancy: a review of the literature
Revista Brasileira de Ginecologia e Obstetrícia. 2025;47:e-rbgo2
- Joan Lins Serafim ,
- Pedro Lucas Santos de Menezes Teles ,
- Amanda Katharinne Souza Lima ,
- Jéssica dos Santos Coelho ,
- Paloma Luna Maranhão Conrado ,
- Valda Lúcia Moreira Luna ,
- Pauliana Valéria Machado Galvão ,
- George Alessandro Maranhão Conrado
Views144Abstract
Statins are the most widely used pharmacological class for treating hyperlipidemia, although they are contraindicated during pregnancy. This study aims to demonstrate the clinical effects of statins in pregnant women through an interactive review. Fifteen original articles were selected, in English or Portuguese, within of five years. Statins have not been associated with the development of fetal malformations and their use may be useful in preventing unfavorable cardiovascular outcomes, with the potential to reduce oxidative stress and angiogenic dysfunction. However, the use of statins to prevent pre-eclampsia in humans has not been properly clarified and further studies are needed. Pravastatin is considered safer than statins for use during pregnancy.
Key-words Antihypertensive agentsHydroxymethylglutaryl-CoA reductase inhibitorsPravastatinPre-eclampsiaPregnancyPregnant womanSee moreThis is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. 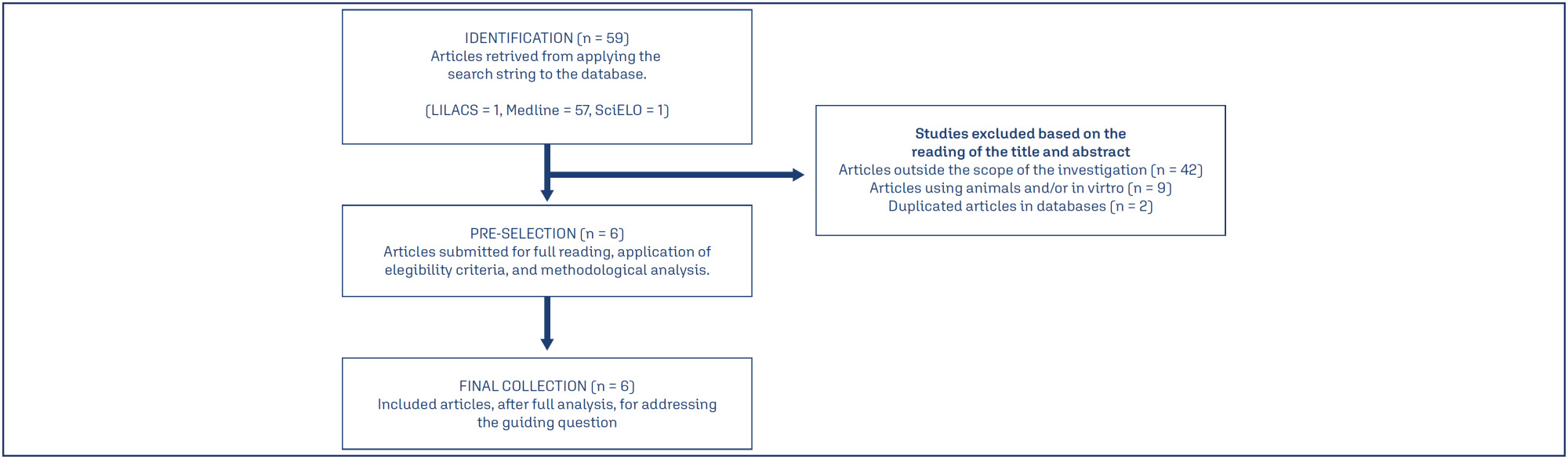
- Joan Lins Serafim
-
Review Article06-03-2024
How can we reduce maternal mortality due to preeclampsia? The 4P rule
- Henri Augusto Korkes ,
- Ricardo Carvalho Cavalli ,
- Leandro Gustavo De Oliveira ,
- José Geraldo Lopes Ramos ,
- Sérgio Hofmeister de Almeida Martins Costa , [ ... ],
- Maria Laura Costa
Abstract
Review ArticleHow can we reduce maternal mortality due to preeclampsia? The 4P rule
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo43
- Henri Augusto Korkes ,
- Ricardo Carvalho Cavalli ,
- Leandro Gustavo De Oliveira ,
- José Geraldo Lopes Ramos ,
- Sérgio Hofmeister de Almeida Martins Costa ,
- Francisco Lázaro Pereira de Sousa ,
- Edson Vieira da Cunha Filho ,
- Maria Rita de Souza Mesquita ,
- Mário Dias Corrêa Júnior ,
- Ana Cristina Pinheiro Fernandes Araújo ,
- Alberto Carlos Moreno Zaconeta ,
- Carlos Henrique Esteves Freire ,
- Carlos Eduardo Poli de Figueiredo ,
- Edilberto Alves Pereira da Rocha Filho ,
- Nelson Sass ,
- José Carlos Peraçoli ,
- Maria Laura Costa
Views309See moreAbstract
In low and middle-income countries such as Brazil, most maternal deaths are related to hypertensive complications. Preeclampsia is the leading cause of maternal mortality and morbidity. Significant proportion is associated with the following factors: lack of identification of high-risk women, lack of adequate prevention, difficulty in maintaining a high-risk prenatal follow-up, delayed diagnosis, insecurity and low use of magnesium sulphate, delayed pregnancy interruption and lack of postpartum follow-up of these high-risk cases. Four major actions are proposed to minimize this alarming clinical picture and reduce the mortality rates due to preeclampsia, called the "4 P Rule" (Adequate Prevention – Vigilant Prenatal Care – Timely Delivery (Parturition) – Safe Postpartum). From this simple "rule" we can open a range of important processes and reminders that may help in the guidance of preeclampsia management.
Views309This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Review ArticleHow can we reduce maternal mortality due to preeclampsia? The 4P rule
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo43
- Henri Augusto Korkes ,
- Ricardo Carvalho Cavalli ,
- Leandro Gustavo De Oliveira ,
- José Geraldo Lopes Ramos ,
- Sérgio Hofmeister de Almeida Martins Costa ,
- Francisco Lázaro Pereira de Sousa ,
- Edson Vieira da Cunha Filho ,
- Maria Rita de Souza Mesquita ,
- Mário Dias Corrêa Júnior ,
- Ana Cristina Pinheiro Fernandes Araújo ,
- Alberto Carlos Moreno Zaconeta ,
- Carlos Henrique Esteves Freire ,
- Carlos Eduardo Poli de Figueiredo ,
- Edilberto Alves Pereira da Rocha Filho ,
- Nelson Sass ,
- José Carlos Peraçoli ,
- Maria Laura Costa
Views309See moreAbstract
In low and middle-income countries such as Brazil, most maternal deaths are related to hypertensive complications. Preeclampsia is the leading cause of maternal mortality and morbidity. Significant proportion is associated with the following factors: lack of identification of high-risk women, lack of adequate prevention, difficulty in maintaining a high-risk prenatal follow-up, delayed diagnosis, insecurity and low use of magnesium sulphate, delayed pregnancy interruption and lack of postpartum follow-up of these high-risk cases. Four major actions are proposed to minimize this alarming clinical picture and reduce the mortality rates due to preeclampsia, called the "4 P Rule" (Adequate Prevention – Vigilant Prenatal Care – Timely Delivery (Parturition) – Safe Postpartum). From this simple "rule" we can open a range of important processes and reminders that may help in the guidance of preeclampsia management.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Henri Augusto Korkes
-
Original Article00-00-2024
Early and late-onset preeclampsia: effects of DDAH2 polymorphisms on ADMA levels and association with DDAH2 haplotypes
- Fernanda Santos Mendes ,
- Marcelo Rizzatti Luizon ,
- Ana Cristina dos Santos Lopes ,
- Daniela Alves Pereira ,
- Fernanda Cristina Gontijo Evangelista , [ ... ],
- Patrícia Nessralla Alpoim
Abstract
Original ArticleEarly and late-onset preeclampsia: effects of DDAH2 polymorphisms on ADMA levels and association with DDAH2 haplotypes
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo19
- Fernanda Santos Mendes ,
- Marcelo Rizzatti Luizon ,
- Ana Cristina dos Santos Lopes ,
- Daniela Alves Pereira ,
- Fernanda Cristina Gontijo Evangelista ,
- Lara Carvalho Godoi ,
- Luci Maria Dusse ,
- Patrícia Nessralla Alpoim
Views634Abstract
Objective:
To examine whether the DDAH2 promoter polymorphisms -1415G/A (rs2272592), -1151A/C (rs805304) and -449G/C (rs805305), and their haplotypes, are associated with PE compared with normotensive pregnant women, and whether they affect ADMA levels in these groups.
Methods:
A total of 208 pregnant women were included in the study and classified as early-onset (N=57) or late-onset PE (N =49), and as normotensive pregnant women (N = 102).
Results:
Pregnant with early-onset PE carrying the GC and GG genotypes for the DDAH2 -449G/C polymorphism had increased ADMA levels (P=0.01). No association of DDAH2 polymorphisms with PE in single-locus analysis was found. However, the G-C-G haplotype was associated with the risk for late-onset PE.
Conclusion:
It is suggested that DDAH2 polymorphisms could affect ADMA levels in PE, and that DDAH2 haplotypes may affect the risk for PE.
Key-words Asymmetric dimethylarginineDimethylarginine dimethylaminohydrolase 2 geneGenotypeHaplotypesNitric Oxide SynthaseNitric Oxide Synthase Type III/ geneticsPolymorphism, geneticPre-eclampsiaPregnant womenSee moreViews634This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Original ArticleEarly and late-onset preeclampsia: effects of DDAH2 polymorphisms on ADMA levels and association with DDAH2 haplotypes
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo19
- Fernanda Santos Mendes ,
- Marcelo Rizzatti Luizon ,
- Ana Cristina dos Santos Lopes ,
- Daniela Alves Pereira ,
- Fernanda Cristina Gontijo Evangelista ,
- Lara Carvalho Godoi ,
- Luci Maria Dusse ,
- Patrícia Nessralla Alpoim
Views634Abstract
Objective:
To examine whether the DDAH2 promoter polymorphisms -1415G/A (rs2272592), -1151A/C (rs805304) and -449G/C (rs805305), and their haplotypes, are associated with PE compared with normotensive pregnant women, and whether they affect ADMA levels in these groups.
Methods:
A total of 208 pregnant women were included in the study and classified as early-onset (N=57) or late-onset PE (N =49), and as normotensive pregnant women (N = 102).
Results:
Pregnant with early-onset PE carrying the GC and GG genotypes for the DDAH2 -449G/C polymorphism had increased ADMA levels (P=0.01). No association of DDAH2 polymorphisms with PE in single-locus analysis was found. However, the G-C-G haplotype was associated with the risk for late-onset PE.
Conclusion:
It is suggested that DDAH2 polymorphisms could affect ADMA levels in PE, and that DDAH2 haplotypes may affect the risk for PE.
Key-words Asymmetric dimethylarginineDimethylarginine dimethylaminohydrolase 2 geneGenotypeHaplotypesNitric Oxide SynthaseNitric Oxide Synthase Type III/ geneticsPolymorphism, geneticPre-eclampsiaPregnant womenSee moreThis is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Fernanda Santos Mendes
-
Original Article02-09-2022
Could Aspirin Treatment Modify the Assessment of the Uterine Arteries?
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):231-237
Abstract
Original ArticleCould Aspirin Treatment Modify the Assessment of the Uterine Arteries?
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):231-237
Views207See moreAbstract
Objective
To analyze whether acetylsalicylic (ASA) intake modifies the mean uterine arteries pulsatility index (UtA-PI) at the 2nd or 3rd trimester in a cohort of pregnant women with abnormal mean UtA-PI at between 11 and 14 weeks of gestation.
Methods
This is a retrospective cohort study. Singleton pregnancies with abnormal mean UtA-PI at between 11 and 14 weeks of gestation were studied. The participants were divided into 3 groups: 1) If the participant did not take ASA during pregnancy; 2) If the participant took ASA before 14 weeks of gestation; and 3) If the participant took ASA after 14 weeks of gestation. The mean UtA-PI was evaluated at the 2nd and 3rd trimesters, and it was considered to improve when it decreased below the 95th percentile. The prevalence ratio (PR) and the number needed to treat (NNT) werecalculated.
Results
A total of 72 participants with a mean UtA-PI>95th percentile at the 1st trimester of gestation were evaluated. Out of the 18 participants who took ASA, 8 participants started it before 14 weeks of gestation and 10 after. A total of 33.3% of these participants had improved the mean UtA-PI at the 2nd and 3rd trimesters of gestation, although it was not statistically significant (p=0.154). The prevalence ratio was 0.95 (95% confidence interval [CI]: 0.31-1.89), but between the 1st and 2nd trimesters of gestation, the PR was 0.92 (95%CI: 0.21-0.99) and it was statistically significant.
Conclusion
The present work demonstrates a modification of the mean UtA-PI in participants who took ASA compared with those who did not. It is important to check if ASA can modify the normal limits of uterine arteries because this could have an impact on surveillance.
Views207This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Original ArticleCould Aspirin Treatment Modify the Assessment of the Uterine Arteries?
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):231-237
Views207See moreAbstract
Objective
To analyze whether acetylsalicylic (ASA) intake modifies the mean uterine arteries pulsatility index (UtA-PI) at the 2nd or 3rd trimester in a cohort of pregnant women with abnormal mean UtA-PI at between 11 and 14 weeks of gestation.
Methods
This is a retrospective cohort study. Singleton pregnancies with abnormal mean UtA-PI at between 11 and 14 weeks of gestation were studied. The participants were divided into 3 groups: 1) If the participant did not take ASA during pregnancy; 2) If the participant took ASA before 14 weeks of gestation; and 3) If the participant took ASA after 14 weeks of gestation. The mean UtA-PI was evaluated at the 2nd and 3rd trimesters, and it was considered to improve when it decreased below the 95th percentile. The prevalence ratio (PR) and the number needed to treat (NNT) werecalculated.
Results
A total of 72 participants with a mean UtA-PI>95th percentile at the 1st trimester of gestation were evaluated. Out of the 18 participants who took ASA, 8 participants started it before 14 weeks of gestation and 10 after. A total of 33.3% of these participants had improved the mean UtA-PI at the 2nd and 3rd trimesters of gestation, although it was not statistically significant (p=0.154). The prevalence ratio was 0.95 (95% confidence interval [CI]: 0.31-1.89), but between the 1st and 2nd trimesters of gestation, the PR was 0.92 (95%CI: 0.21-0.99) and it was statistically significant.
Conclusion
The present work demonstrates a modification of the mean UtA-PI in participants who took ASA compared with those who did not. It is important to check if ASA can modify the normal limits of uterine arteries because this could have an impact on surveillance.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Original Article12-21-2020
Evaluation of Angiogenic Factors (PlGF and sFlt-1) in Pre-eclampsia Diagnosis
- Catherine Primo Nogueira de Sá ,
- Mirela Foresti Jiménez ,
- Marcos Wengrover Rosa ,
- Ellen Machado Arlindo ,
- Antonio Celso Koehler Ayub , [ ... ],
- Patrícia El Beitune
Abstract
Original ArticleEvaluation of Angiogenic Factors (PlGF and sFlt-1) in Pre-eclampsia Diagnosis
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):697-704
- Catherine Primo Nogueira de Sá ,
- Mirela Foresti Jiménez ,
- Marcos Wengrover Rosa ,
- Ellen Machado Arlindo ,
- Antonio Celso Koehler Ayub ,
- Rodrigo Bernardes Cardoso ,
- Régis Kreitchmann ,
- Patrícia El Beitune
Views312See moreAbstract
Objective:
Recent observations support the hypothesis that an imbalance between angiogenic factors has a fundamental role in the pathogenesis of pre-eclampsia and is responsible for the clinical manifestations of the disease. The goal of the present study was to evaluate the sensitivity, specificity, and the best accuracy level of Soluble fms-like tyrosine kinase-1 (sFlt-1), placental growth factor (PlGF), and sFlt-1/PlGF ratio in maternal serum and protein/creatinine ratio in urine sample to define the best cutoff point of these tests to discriminate between the patients with gestational hypertension and the patients with pre-eclampsia, to evaluate the possibility of using them as diagnostic methods.
Methods:
A prospective longitudinal study was performed, and blood samples were collected from 95 pregnant patients with hypertension to measure serum concentrations of biomarkers sFlt-1 and PlGF. Urine samples were collected for protein screening. Significance was set as p < 0.05.
Results:
The sFlt-1/PlGF ratio demonstrated a sensitivity of 57.5% and a specificity of 60% using 50.4 as a cutoff point. The test that showed the best accuracy in the diagnosis of pre-eclampsia was protein/creatinine ratio, with a sensitivity of 78.9% and a specificity of 70% using 0.4 as a cutoff point and showing an area under the receiver operating characteristic curve of 0.80 (p < 0.001).
Conclusion:
No studied laboratory test proved to be fairly accurate for the diagnosis of pre-eclampsia, except for the protein/creatinine ratio. The evidence is insufficient to recommend biomarkers sFlt-1 and PlGF to be used for the diagnosis of pre-eclampsia.
Views312This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Original ArticleEvaluation of Angiogenic Factors (PlGF and sFlt-1) in Pre-eclampsia Diagnosis
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):697-704
- Catherine Primo Nogueira de Sá ,
- Mirela Foresti Jiménez ,
- Marcos Wengrover Rosa ,
- Ellen Machado Arlindo ,
- Antonio Celso Koehler Ayub ,
- Rodrigo Bernardes Cardoso ,
- Régis Kreitchmann ,
- Patrícia El Beitune
Views312See moreAbstract
Objective:
Recent observations support the hypothesis that an imbalance between angiogenic factors has a fundamental role in the pathogenesis of pre-eclampsia and is responsible for the clinical manifestations of the disease. The goal of the present study was to evaluate the sensitivity, specificity, and the best accuracy level of Soluble fms-like tyrosine kinase-1 (sFlt-1), placental growth factor (PlGF), and sFlt-1/PlGF ratio in maternal serum and protein/creatinine ratio in urine sample to define the best cutoff point of these tests to discriminate between the patients with gestational hypertension and the patients with pre-eclampsia, to evaluate the possibility of using them as diagnostic methods.
Methods:
A prospective longitudinal study was performed, and blood samples were collected from 95 pregnant patients with hypertension to measure serum concentrations of biomarkers sFlt-1 and PlGF. Urine samples were collected for protein screening. Significance was set as p < 0.05.
Results:
The sFlt-1/PlGF ratio demonstrated a sensitivity of 57.5% and a specificity of 60% using 50.4 as a cutoff point. The test that showed the best accuracy in the diagnosis of pre-eclampsia was protein/creatinine ratio, with a sensitivity of 78.9% and a specificity of 70% using 0.4 as a cutoff point and showing an area under the receiver operating characteristic curve of 0.80 (p < 0.001).
Conclusion:
No studied laboratory test proved to be fairly accurate for the diagnosis of pre-eclampsia, except for the protein/creatinine ratio. The evidence is insufficient to recommend biomarkers sFlt-1 and PlGF to be used for the diagnosis of pre-eclampsia.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Catherine Primo Nogueira de Sá
-
Original Article12-21-2020
Hypertensive Disorders: Prevalence, Perinatal Outcomes and Cesarean Section Rates in Pregnant Women Hospitalized for Delivery
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):690-696
Abstract
Original ArticleHypertensive Disorders: Prevalence, Perinatal Outcomes and Cesarean Section Rates in Pregnant Women Hospitalized for Delivery
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):690-696
Views171See moreAbstract
Objective:
To evaluate the prevalence of hypertensive disorders, perinatal outcomes (preterm infants, low birthweight infants and Apgar score < 7 at the 5th minute and fetal deaths) and the cesarean rates in pregnant women hospitalized for delivery at the Maternidade Hilda Brandão da Santa Casa de Belo Horizonte, Belo Horizonte, state of Minas Gerais, Brazil, from March 1, 2008 to February 28, 2018.
Methods:
A case-control study was performed, and the groups selected for comparison were those of pregnant women with and without hypertensive disorders. Out of the 36,724 women, 4,464 were diagnosed with hypertensive disorders and 32,260 did not present hypertensive disorders
Results:
The prevalence of hypertensive disorders was 12.16%; the perinatal outcomes and cesarean rates between the 2 groups with and without hypertensive disorders were: preterm infants (21.70% versus 9.66%, odds ratio [OR] 2.59, 95% confidence interval [CI], 2.40-2.80, p < 0.001); low birthweight infants (24.48% versus 10.56%; OR 2.75; 95% CI, 2.55-2.96; p < 0.001); Apgar score < 7 at the 5th minute (1.40% versus 1.10%; OR 1.27; 95% CI, 0.97-1.67; p = 0.84); dead fetuses diagnosed prior to delivery (1.90% versus 0.91%; OR 2.12; 95% CI, 1.67-2.70; p < 0.001); cesarean rates (60.22% versus 31.21%; OR 3.34; 95% CI, 3.14-3.55; p < 0.001).
Conclusion:
Hypertensive disorders are associated with higher rates of cesarean deliveries and higher risk of preterm infants, low birthweight infants and a higher risk of fetal deaths.
Views171This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Original ArticleHypertensive Disorders: Prevalence, Perinatal Outcomes and Cesarean Section Rates in Pregnant Women Hospitalized for Delivery
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):690-696
Views171See moreAbstract
Objective:
To evaluate the prevalence of hypertensive disorders, perinatal outcomes (preterm infants, low birthweight infants and Apgar score < 7 at the 5th minute and fetal deaths) and the cesarean rates in pregnant women hospitalized for delivery at the Maternidade Hilda Brandão da Santa Casa de Belo Horizonte, Belo Horizonte, state of Minas Gerais, Brazil, from March 1, 2008 to February 28, 2018.
Methods:
A case-control study was performed, and the groups selected for comparison were those of pregnant women with and without hypertensive disorders. Out of the 36,724 women, 4,464 were diagnosed with hypertensive disorders and 32,260 did not present hypertensive disorders
Results:
The prevalence of hypertensive disorders was 12.16%; the perinatal outcomes and cesarean rates between the 2 groups with and without hypertensive disorders were: preterm infants (21.70% versus 9.66%, odds ratio [OR] 2.59, 95% confidence interval [CI], 2.40-2.80, p < 0.001); low birthweight infants (24.48% versus 10.56%; OR 2.75; 95% CI, 2.55-2.96; p < 0.001); Apgar score < 7 at the 5th minute (1.40% versus 1.10%; OR 1.27; 95% CI, 0.97-1.67; p = 0.84); dead fetuses diagnosed prior to delivery (1.90% versus 0.91%; OR 2.12; 95% CI, 1.67-2.70; p < 0.001); cesarean rates (60.22% versus 31.21%; OR 3.34; 95% CI, 3.14-3.55; p < 0.001).
Conclusion:
Hypertensive disorders are associated with higher rates of cesarean deliveries and higher risk of preterm infants, low birthweight infants and a higher risk of fetal deaths.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. -
Case Report12-21-2020
Serous Retinal Detachment in Pre-eclampsia: Case Report and Literature Review
- Joana Teresa Botelho Vasconcelos Raposo ,
- Bruna Carina Da Silva Melo ,
- Nuno Filipe Bernardo Belo Maciel ,
- Sara Dias Leite ,
- Óscar Renato Coutinho Rebelo , [ ... ],
- Ana Maria Furtado Lima
Abstract
Case ReportSerous Retinal Detachment in Pre-eclampsia: Case Report and Literature Review
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):772-773
- Joana Teresa Botelho Vasconcelos Raposo ,
- Bruna Carina Da Silva Melo ,
- Nuno Filipe Bernardo Belo Maciel ,
- Sara Dias Leite ,
- Óscar Renato Coutinho Rebelo ,
- Ana Maria Furtado Lima
Views234See moreAbstract
Pre-eclampsia (PE) is an obstetric disease with a multifactorial cause that affects ∼ 5% of pregnant women. Vision can be affected with varying severity, and retinal detachment is a very rare complication. It tends to be bilateral, diagnosed postpartum, and more prevalent in women who are primiparous and/or undergo caesarean delivery. The condition typically resolves completely and rarely causes total visual loss in the affected women. Fluorescence angiographic findings support the hypothesis that retinal detachment in PE is secondary to choroidal ischemia from intense arteriolar vasospasm. The present article is related to a case of a 37-year-old pregnant woman who had PE associated with a progressive blurred vision, diagnosed by ophthalmology as serous macular detachment of the retina.
Views234This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
Case ReportSerous Retinal Detachment in Pre-eclampsia: Case Report and Literature Review
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):772-773
- Joana Teresa Botelho Vasconcelos Raposo ,
- Bruna Carina Da Silva Melo ,
- Nuno Filipe Bernardo Belo Maciel ,
- Sara Dias Leite ,
- Óscar Renato Coutinho Rebelo ,
- Ana Maria Furtado Lima
Views234See moreAbstract
Pre-eclampsia (PE) is an obstetric disease with a multifactorial cause that affects ∼ 5% of pregnant women. Vision can be affected with varying severity, and retinal detachment is a very rare complication. It tends to be bilateral, diagnosed postpartum, and more prevalent in women who are primiparous and/or undergo caesarean delivery. The condition typically resolves completely and rarely causes total visual loss in the affected women. Fluorescence angiographic findings support the hypothesis that retinal detachment in PE is secondary to choroidal ischemia from intense arteriolar vasospasm. The present article is related to a case of a 37-year-old pregnant woman who had PE associated with a progressive blurred vision, diagnosed by ophthalmology as serous macular detachment of the retina.
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - Joana Teresa Botelho Vasconcelos Raposo
-
FEBRASGO POSITION STATEMENT06-27-2019
Pre-eclampsia/Eclampsia
- José Carlos Peraçoli ,
- Vera Therezinha Medeiros Borges,
- José Geraldo Lopes Ramos,
- Ricardo de Carvalho Cavalli,
- Sérgio Hofmeister de Almeida Martins Costa, [ ... ],
- Edson Viera da Cunha Filho
Abstract
FEBRASGO POSITION STATEMENTPre-eclampsia/Eclampsia
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(5):318-332
- José Carlos Peraçoli ,
- Vera Therezinha Medeiros Borges,
- José Geraldo Lopes Ramos,
- Ricardo de Carvalho Cavalli,
- Sérgio Hofmeister de Almeida Martins Costa,
- Leandro Gustavo de Oliveira,
- Francisco Lazaro Pereira de Souza,
- Henri Augusto Korkes,
- Ione Rodrigues Brum,
- Maria Laura Costa,
- Mário Dias Corrêa Junior,
- Nelson Sass,
- Angélica Lemos Debs Diniz,
- Caio Antonio de Campos Prado,
- Edson Viera da Cunha Filho
Views90See moreAbstract
Pre-eclampsia is a multifactorial and multisystemic disease specific to gestation. It is classically diagnosed by the presence of hypertension associated with proteinuria manifested in a previously normotensive pregnant woman after the 20th week of gestation. Pre-eclampsia is also considered in the absence of proteinuria if there is target organ damage. The present review takes a general approach focused on aspects of practical interest in the clinical and obstetric care of these women. Thus, it explores the still unknown etiology, current aspects of pathophysiology and of the diagnosis, the approach to disease prediction, its adverse outcomes and prevention. Management is based on general principles, on nonpharmacological and on pharmacological clinical treatment of severe or nonsevere situations with emphasis on the hypertensive crisis and eclampsia. Obstetric management is based on preeclampsia without or with signs of clinical and/or laboratory deterioration, stratification of gestational age
Views90This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract
FEBRASGO POSITION STATEMENTPre-eclampsia/Eclampsia
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(5):318-332
- José Carlos Peraçoli ,
- Vera Therezinha Medeiros Borges,
- José Geraldo Lopes Ramos,
- Ricardo de Carvalho Cavalli,
- Sérgio Hofmeister de Almeida Martins Costa,
- Leandro Gustavo de Oliveira,
- Francisco Lazaro Pereira de Souza,
- Henri Augusto Korkes,
- Ione Rodrigues Brum,
- Maria Laura Costa,
- Mário Dias Corrêa Junior,
- Nelson Sass,
- Angélica Lemos Debs Diniz,
- Caio Antonio de Campos Prado,
- Edson Viera da Cunha Filho
Views90See moreAbstract
Pre-eclampsia is a multifactorial and multisystemic disease specific to gestation. It is classically diagnosed by the presence of hypertension associated with proteinuria manifested in a previously normotensive pregnant woman after the 20th week of gestation. Pre-eclampsia is also considered in the absence of proteinuria if there is target organ damage. The present review takes a general approach focused on aspects of practical interest in the clinical and obstetric care of these women. Thus, it explores the still unknown etiology, current aspects of pathophysiology and of the diagnosis, the approach to disease prediction, its adverse outcomes and prevention. Management is based on general principles, on nonpharmacological and on pharmacological clinical treatment of severe or nonsevere situations with emphasis on the hypertensive crisis and eclampsia. Obstetric management is based on preeclampsia without or with signs of clinical and/or laboratory deterioration, stratification of gestational age
This is an Open Access article distributed under the terms of the Creative Commons Attribution License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. - José Carlos Peraçoli