You searched for:"Diama Bhadra Vale"
We found (10) results for your search.Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo44
To describe Top-hat results and their association with margin status and disease relapse in a referral facility in Brazil.
A retrospective study of 440 women submitted to LEEP to treat HSIL, in which 80 cases were complemented immediately by the top hat procedure (Top-hat Group - TH). TH Group was compared to women not submitted to Top-hat (NTH). The sample by convenience included all women that underwent LEEP from January 2017 to July 2020. The main outcome was the histological result. Other variables were margins, age, transformation zone (TZ), depth, and relapse. The analysis used the Chi-square test and logistic regression.
The TH Group was predominantly 40 and older (NTH 23.1% vs. TH 65.0%, p<0.001). No difference was found in having CIN2/CIN3 as the final diagnosis (NTH 17.0% vs. TH 21.3%, p=0.362), or in the prevalence of relapse (NTH 12.0% vs. TH 9.0%, p=0.482). Of the 80 patients submitted to top hat, the histological result was CIN2/CIN3 in eight. A negative top hat result was related to a negative endocervical margin of 83.3%. A CIN2/CIN3 Top-hat result was related to CIN2/CIN3 margin in 62.5% (p=0.009). The chance of obtaining a top hat negative result was 22.4 times higher (2.4-211.0) when the endocervical margin was negative and 14.5 times higher (1.5-140.7) when the ectocervical margin was negative.
The top hat procedure did not alter the final diagnosis of LEEP. No impact on relapse was observed. The procedure should be avoided in women of reproductive age.
Summary
Rev Bras Ginecol Obstet. 2024;46:e-rbgo44
To describe Top-hat results and their association with margin status and disease relapse in a referral facility in Brazil.
A retrospective study of 440 women submitted to LEEP to treat HSIL, in which 80 cases were complemented immediately by the top hat procedure (Top-hat Group - TH). TH Group was compared to women not submitted to Top-hat (NTH). The sample by convenience included all women that underwent LEEP from January 2017 to July 2020. The main outcome was the histological result. Other variables were margins, age, transformation zone (TZ), depth, and relapse. The analysis used the Chi-square test and logistic regression.
The TH Group was predominantly 40 and older (NTH 23.1% vs. TH 65.0%, p<0.001). No difference was found in having CIN2/CIN3 as the final diagnosis (NTH 17.0% vs. TH 21.3%, p=0.362), or in the prevalence of relapse (NTH 12.0% vs. TH 9.0%, p=0.482). Of the 80 patients submitted to top hat, the histological result was CIN2/CIN3 in eight. A negative top hat result was related to a negative endocervical margin of 83.3%. A CIN2/CIN3 Top-hat result was related to CIN2/CIN3 margin in 62.5% (p=0.009). The chance of obtaining a top hat negative result was 22.4 times higher (2.4-211.0) when the endocervical margin was negative and 14.5 times higher (1.5-140.7) when the ectocervical margin was negative.
The top hat procedure did not alter the final diagnosis of LEEP. No impact on relapse was observed. The procedure should be avoided in women of reproductive age.
Summary
Rev Bras Ginecol Obstet. 2023;45(1):21-30
To evaluate the rates of precancerous lesions, colposcopy referral, and positive predictive value (PPV) by age groups of a population-based screening with DNA-HPV testing.
The present demonstration study compared 16,384 HPV tests performed in the first 30 months of the program with 19,992 women tested in the cytology screening. The colposcopy referral rate and PPV for CIN2+ and CIN3+ by age group and screening program were compared. The statistical analysis used the chi-squared test and odds ratio (OR) with 95% confidence interval (95%CI).
The HPV tests were 3.26% positive for HPV16-HPV18 and 9.92% positive for 12 other HPVs with a 3.7 times higher colposcopy referral rate than the cytology program, which had 1.68% abnormalities. Human Papillomavirus testing detected 103 CIN2, 89 CIN3, and one AIS, compared with 24 CIN2 and 54 CIN3 detected by cytology (p < 0.0001). The age group between 25 and 29 years old screened by HPV testing had 2.4 to 3.0 times more positivity, 13.0% colposcopy referral, twice more than women aged 30 to 39 years old (7.7%; p < 0.0001), and detected 20 CIN3 and 3 early-stage cancer versus 9 CIN3 and no cancer by cytology screening (CIN3 OR= 2.10; 95%CI: 0.91 -5.25; p = 0.043). The PPV of colposcopy for CIN2+ ranged from 29.5 to 41.0% in the HPV testing program.
There was a significant increase in detections of cervix precancerous lesions in a short period of screening with HPV testing. In women < 30 years old, the HPV testing exhibited more positivity, high colposcopy referral rate, similar colposcopy PPV to older women, and more detection of HSIL and early-stage cervical cancer.
Summary
Rev Bras Ginecol Obstet. 2023;45(1):21-30
To evaluate the rates of precancerous lesions, colposcopy referral, and positive predictive value (PPV) by age groups of a population-based screening with DNA-HPV testing.
The present demonstration study compared 16,384 HPV tests performed in the first 30 months of the program with 19,992 women tested in the cytology screening. The colposcopy referral rate and PPV for CIN2+ and CIN3+ by age group and screening program were compared. The statistical analysis used the chi-squared test and odds ratio (OR) with 95% confidence interval (95%CI).
The HPV tests were 3.26% positive for HPV16-HPV18 and 9.92% positive for 12 other HPVs with a 3.7 times higher colposcopy referral rate than the cytology program, which had 1.68% abnormalities. Human Papillomavirus testing detected 103 CIN2, 89 CIN3, and one AIS, compared with 24 CIN2 and 54 CIN3 detected by cytology (p < 0.0001). The age group between 25 and 29 years old screened by HPV testing had 2.4 to 3.0 times more positivity, 13.0% colposcopy referral, twice more than women aged 30 to 39 years old (7.7%; p < 0.0001), and detected 20 CIN3 and 3 early-stage cancer versus 9 CIN3 and no cancer by cytology screening (CIN3 OR= 2.10; 95%CI: 0.91 -5.25; p = 0.043). The PPV of colposcopy for CIN2+ ranged from 29.5 to 41.0% in the HPV testing program.
There was a significant increase in detections of cervix precancerous lesions in a short period of screening with HPV testing. In women < 30 years old, the HPV testing exhibited more positivity, high colposcopy referral rate, similar colposcopy PPV to older women, and more detection of HSIL and early-stage cervical cancer.
Summary
Rev Bras Ginecol Obstet. 2015;37(5):229-232
DOI 10.1590/SO100-720320150005295
To compare the frequency of an ASCUS Pap Smear result in pregnant and
non-pregnant women, stratified by age group.
We analyzed the results of 1,336,180 cytopathologyc exams of Pap smears performed
between 2000 and 2009 (ten years) with the purpose of screening for cervical
carcinoma. Comparisons were made between pregnant and non-pregnant women, and the
sample was stratified into three age groups (20-24, 25-29 and 30-34 years). The
χ2 test was used and the magnitude of association was determined by
the by Odds Ratio (OR) with the 95% confidence interval (95%CI).
A Total of 447,489 samples were excluded on the basis of the criteria adopted,
for a total final sample of 37,137 pregnant women and 851,554 non-pregnant women.
An ASCUS result was detected in 1.2% of cases, with a significant difference
between pregnant and non-pregnant women in the age groups of 20-24 years (OR=0.85;
95%CI 0.75-0.97) and 25-29 years (OR=0.78; 95%CI 0.63-0.96). There was no
difference in the group between 30-34 years (OR=0.76; 95%CI 0.57-1.03).
This study suggested that non-pregnant women have a higher frequency of ASCUS,
most evident in the age group of 20 to 29 years. The collection of cervical cancer
screening should not be a compulsory part of the prenatal routine.
Summary
Rev Bras Ginecol Obstet. 2015;37(5):229-232
DOI 10.1590/SO100-720320150005295
To compare the frequency of an ASCUS Pap Smear result in pregnant and
non-pregnant women, stratified by age group.
We analyzed the results of 1,336,180 cytopathologyc exams of Pap smears performed
between 2000 and 2009 (ten years) with the purpose of screening for cervical
carcinoma. Comparisons were made between pregnant and non-pregnant women, and the
sample was stratified into three age groups (20-24, 25-29 and 30-34 years). The
χ2 test was used and the magnitude of association was determined by
the by Odds Ratio (OR) with the 95% confidence interval (95%CI).
A Total of 447,489 samples were excluded on the basis of the criteria adopted,
for a total final sample of 37,137 pregnant women and 851,554 non-pregnant women.
An ASCUS result was detected in 1.2% of cases, with a significant difference
between pregnant and non-pregnant women in the age groups of 20-24 years (OR=0.85;
95%CI 0.75-0.97) and 25-29 years (OR=0.78; 95%CI 0.63-0.96). There was no
difference in the group between 30-34 years (OR=0.76; 95%CI 0.57-1.03).
This study suggested that non-pregnant women have a higher frequency of ASCUS,
most evident in the age group of 20 to 29 years. The collection of cervical cancer
screening should not be a compulsory part of the prenatal routine.
Summary
Rev Bras Ginecol Obstet. 2019;41(4):249-255
The present study aimed to examine which development indicators are correlated with cervical cancer (CC) mortality rates in Brazil.
This was an ecological study that correlatedmortality rates and indicators, such as human development index (HDI), gross domestic product (GDP) per capita, illiteracy rate, fertility rate, screening coverage, proportion of private health insurance use, density of physicians, and density of radiotherapy centers. Themortality rateswere obtained fromthe Brazilian national registry, while the indicators were based on official reports from the Ministry of Health. Univariate and multivariate linear regression was used.
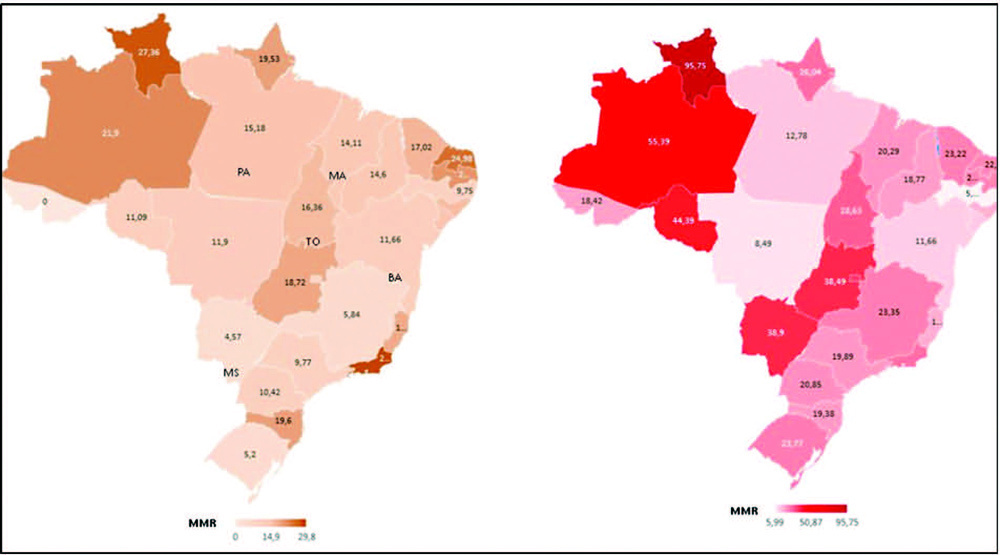
Among the states of Brazil, the average age-specific CC mortality rate from 2008 to 2012 varied from 4.6 to 22.9 per 100,000 women/year. In the univariate analysis, HDI, proportion of private health insurance use, density of physicians, and density of radiotherapy centers were inversely correlated with the mortality rates. Fertility rate was positively correlated with the mortality rates. In the multivariate analysis, only fertility rate was significantly associated with the CC mortality rate (coefficient of correlation: 9.38; 95% confidence interval [CI]: 5.16-13.59).
A decrease in the fertility rate, as expected when the level of development of the regions increases, is related to a decrease in the mortality rate of CC. The results of the present study can help to better monitor the quality assessment of CC programs both among and within countries.
Summary
Rev Bras Ginecol Obstet. 2019;41(4):249-255
The present study aimed to examine which development indicators are correlated with cervical cancer (CC) mortality rates in Brazil.
This was an ecological study that correlatedmortality rates and indicators, such as human development index (HDI), gross domestic product (GDP) per capita, illiteracy rate, fertility rate, screening coverage, proportion of private health insurance use, density of physicians, and density of radiotherapy centers. Themortality rateswere obtained fromthe Brazilian national registry, while the indicators were based on official reports from the Ministry of Health. Univariate and multivariate linear regression was used.
Among the states of Brazil, the average age-specific CC mortality rate from 2008 to 2012 varied from 4.6 to 22.9 per 100,000 women/year. In the univariate analysis, HDI, proportion of private health insurance use, density of physicians, and density of radiotherapy centers were inversely correlated with the mortality rates. Fertility rate was positively correlated with the mortality rates. In the multivariate analysis, only fertility rate was significantly associated with the CC mortality rate (coefficient of correlation: 9.38; 95% confidence interval [CI]: 5.16-13.59).
A decrease in the fertility rate, as expected when the level of development of the regions increases, is related to a decrease in the mortality rate of CC. The results of the present study can help to better monitor the quality assessment of CC programs both among and within countries.
Summary
Rev Bras Ginecol Obstet. 2022;44(3):264-271
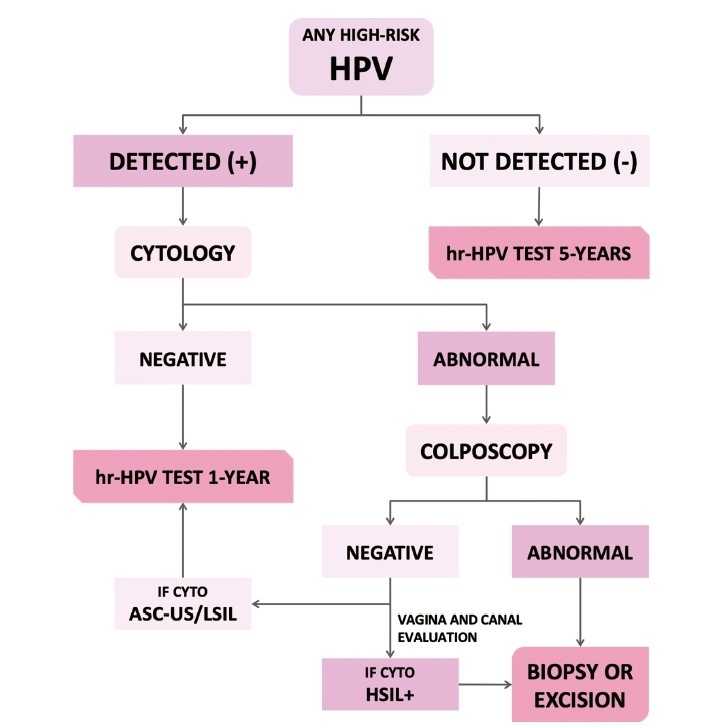
The present update is a reassessment of the 2018 ‘Guidelines for HPV-DNA Testing for Cervical Cancer Screening in Brazil’ (Zeferino et al.)9, according to the changes observed in new international guidelines and knowledge updates. The most relevant and recent guidelines were assessed. Questions regarding the clinical practice were formulated, and the answers considered the perspective of the public and private sectors of the Brazilian health system. The review addressed risk-based strategies regarding age to start and stop screening, the use of cytology and colposcopy to support management decisions, treatment, follow-up strategies, and screening in specific groups, including vaccinated women. The update aims to improve the prevention of cervical cancer and to reduce overtreatment and the misuse of HPV testing.
Summary
Rev Bras Ginecol Obstet. 2022;44(3):264-271
The present update is a reassessment of the 2018 ‘Guidelines for HPV-DNA Testing for Cervical Cancer Screening in Brazil’ (Zeferino et al.)9, according to the changes observed in new international guidelines and knowledge updates. The most relevant and recent guidelines were assessed. Questions regarding the clinical practice were formulated, and the answers considered the perspective of the public and private sectors of the Brazilian health system. The review addressed risk-based strategies regarding age to start and stop screening, the use of cytology and colposcopy to support management decisions, treatment, follow-up strategies, and screening in specific groups, including vaccinated women. The update aims to improve the prevention of cervical cancer and to reduce overtreatment and the misuse of HPV testing.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Rev Bras Ginecol Obstet. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Rev Bras Ginecol Obstet. 2019;41(10):579-580
Summary
Rev Bras Ginecol Obstet. 2019;41(10):579-580
Summary
Rev Bras Ginecol Obstet. 2017;39(2):80-85
To evaluate the association of age at first sexual intercourse with the results of the cervicovaginal cytology.
Observational analytical study about the prevalence of altered cervicovaginal cytology results in women aged between 18 and 34 years from a densely populated area in Brazil, during 10 years. The patients were stratified into 2 categories according to their age at first sexual intercourse (13-16 years and 17-24 years).
From the total of 2,505,154 exams, 898,921 tests were in accordance with the inclusion criteria. Considering women with 4 years or less from the first sexual intercourse as a reference, those with 5 to 9 years and 10 years or more showed a higher prevalence of high-grade squamous intraepithelial lesions (HSILs). Women with an earlier onset of sexual intercourse (13-16 years) showed higher prevalence ratios for atypical squamous cells (ASC), low-grade squamous intraepithelial lesion (LSIL) and HSIL. The prevalence ratio for HSIL adjusted by age at diagnosis and by age at first sexual intercourse was higher only for women with an earlier onset of sexual intercourse.
The age of first sexual intercourse could be a variable that might qualify the selection among young women who are really at a higher risk for HSIL.
Summary
Rev Bras Ginecol Obstet. 2017;39(2):80-85
To evaluate the association of age at first sexual intercourse with the results of the cervicovaginal cytology.
Observational analytical study about the prevalence of altered cervicovaginal cytology results in women aged between 18 and 34 years from a densely populated area in Brazil, during 10 years. The patients were stratified into 2 categories according to their age at first sexual intercourse (13-16 years and 17-24 years).
From the total of 2,505,154 exams, 898,921 tests were in accordance with the inclusion criteria. Considering women with 4 years or less from the first sexual intercourse as a reference, those with 5 to 9 years and 10 years or more showed a higher prevalence of high-grade squamous intraepithelial lesions (HSILs). Women with an earlier onset of sexual intercourse (13-16 years) showed higher prevalence ratios for atypical squamous cells (ASC), low-grade squamous intraepithelial lesion (LSIL) and HSIL. The prevalence ratio for HSIL adjusted by age at diagnosis and by age at first sexual intercourse was higher only for women with an earlier onset of sexual intercourse.
The age of first sexual intercourse could be a variable that might qualify the selection among young women who are really at a higher risk for HSIL.