Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):399-404
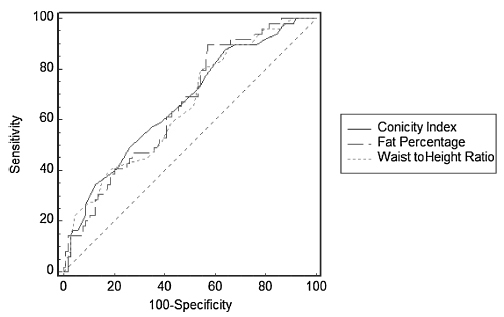
To determine the diagnostic accuracy and the cutoff point of the variables conicity index, waist to height ratio and fat percentage to detect urinary incontinence in physically active older women.
A total of 152 women were analyzed. The instruments used were the International Physical Activity Questionnaire (IPAQ [Area 4]) to check the level of physical activity, and the Diagnostic Form to obtain sociodemographic data and presence of urinary incontinence. To calculate the conicity index, waist to height ratio and fat percentage, body mass, height and waist circumference were measured. Descriptive and inferential statistics were used. Cutoff points, sensitivity (S) and specificity (SP) were determined by receiver operating characteristic (ROC) curves. A 5% significance level was adopted.
The prevalence of urinary incontinence was of 32.2%. The cutoff point with better sensitivity and specificity for the conicity index was 1.23 (S =87.8; SP =35.9); for the waist to height ratio, it was 0.57 (S =79.6; SP =45.6); and for the fat percentage, it was 39.71 (S =89.8; SP =42.7). The area under the ROC curve was 0.666 for the conicity index, 0.653 for the waist to height ratio, and 0.660 for the fat percentage.
The cutoff points for the anthropometric measurements conicity index, waist to height ratio and fat percentage indicate that these measures can be used to predict urinary incontinence in physically active older women. Furthermore, fat percentage seemed to be the best measure for this population.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):399-404
To determine the diagnostic accuracy and the cutoff point of the variables conicity index, waist to height ratio and fat percentage to detect urinary incontinence in physically active older women.
A total of 152 women were analyzed. The instruments used were the International Physical Activity Questionnaire (IPAQ [Area 4]) to check the level of physical activity, and the Diagnostic Form to obtain sociodemographic data and presence of urinary incontinence. To calculate the conicity index, waist to height ratio and fat percentage, body mass, height and waist circumference were measured. Descriptive and inferential statistics were used. Cutoff points, sensitivity (S) and specificity (SP) were determined by receiver operating characteristic (ROC) curves. A 5% significance level was adopted.
The prevalence of urinary incontinence was of 32.2%. The cutoff point with better sensitivity and specificity for the conicity index was 1.23 (S =87.8; SP =35.9); for the waist to height ratio, it was 0.57 (S =79.6; SP =45.6); and for the fat percentage, it was 39.71 (S =89.8; SP =42.7). The area under the ROC curve was 0.666 for the conicity index, 0.653 for the waist to height ratio, and 0.660 for the fat percentage.
The cutoff points for the anthropometric measurements conicity index, waist to height ratio and fat percentage indicate that these measures can be used to predict urinary incontinence in physically active older women. Furthermore, fat percentage seemed to be the best measure for this population.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):405-411
We aimed to evaluate the safety, efficacy and surgical outcomes of combined laparoscopic/vaginal prolapse repair by two surgeons.
A retrospective chart review of all patients (n =135) who underwent apical prolapse repair from February 2009 to December 2012 performed in a collaborative manner by a Minimally Invasive Gynecologic Surgeon and a Urogynecologist. Demographic data (age, body mass index [BMI], race, gravidity, parity) and surgical information (estimated blood loss, operative time, intraoperative complications, readmission and reoperation rates, presence of postoperative infection) were collected.
The majority of patients were postmenopausal (58.91%), multiparous (mean parity =2.49) and overweight (mean BMI =27.71). Nearly 20% had previous prolapse surgery. The most common surgical procedure was laparoscopic supracervical hysterectomy (LSH) with sacrocervicopexy (59.26%), and the most common vaginal repair was of the posterior compartment (78.68%). The median operative time was 149 minutes (82-302), and the estimated blood loss was 100 mL (10-530). Five intraoperative complications, five readmissions and four reoperations were noted. Performance of a concomitant hysterectomy did not affect surgical or anatomical outcomes.
Combination laparoscopic/vaginal prolapse repair by two separate surgeons seems to be an efficient option for operative management.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(8):405-411
We aimed to evaluate the safety, efficacy and surgical outcomes of combined laparoscopic/vaginal prolapse repair by two surgeons.
A retrospective chart review of all patients (n =135) who underwent apical prolapse repair from February 2009 to December 2012 performed in a collaborative manner by a Minimally Invasive Gynecologic Surgeon and a Urogynecologist. Demographic data (age, body mass index [BMI], race, gravidity, parity) and surgical information (estimated blood loss, operative time, intraoperative complications, readmission and reoperation rates, presence of postoperative infection) were collected.
The majority of patients were postmenopausal (58.91%), multiparous (mean parity =2.49) and overweight (mean BMI =27.71). Nearly 20% had previous prolapse surgery. The most common surgical procedure was laparoscopic supracervical hysterectomy (LSH) with sacrocervicopexy (59.26%), and the most common vaginal repair was of the posterior compartment (78.68%). The median operative time was 149 minutes (82-302), and the estimated blood loss was 100 mL (10-530). Five intraoperative complications, five readmissions and four reoperations were noted. Performance of a concomitant hysterectomy did not affect surgical or anatomical outcomes.
Combination laparoscopic/vaginal prolapse repair by two separate surgeons seems to be an efficient option for operative management.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):164-169
The objective of this study is to associate the results obtained while assessing the pelvic floor muscles (PFM) functionality with the score of sexual satisfaction of young adult women.
This is an observational and cross-sectional study. The inclusion criteria were women aged between 20 and 40 years who have had sexual intercourse, nulliparous, BMI lower than 25 kg/m2, and absence of pelvic floor dysfunction. The evaluation consisted of both the medical history and assessment of the PFM functionality using the Perina pressure biofeedback and Oxford Scale. We measured sexual satisfaction using the Female Sexual Quotient questionnaire and used the KolmogorovSmirnov test to verify the normality of the data. We analyzed non-parametric variables using the Spearman correlation test. The significance level was 5 %.
A total of 80 women with a median age of 26 years and median BMI of 21.64 kg/m2 participated in this study. We divided the subjects into two groups, best and worse PFM functionality, according to median Perina pressure biofeedback and Oxford scale. We found no difference between the groups when comparing the sexual satisfaction scores. There was only a slight significant correlation between the Contraction Voluntary Average obtained using the pressure biofeedback and the primary domain (r = 0.27; p = 0.01).
This study found a slight correlation between PFM functionality and the functionality of the primary domain of the Female Sexual Quotient questionnaire. Therefore, it is not possible to state whether there is an association between the PFM functionality and female sexual satisfaction in young adults.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):164-169
The objective of this study is to associate the results obtained while assessing the pelvic floor muscles (PFM) functionality with the score of sexual satisfaction of young adult women.
This is an observational and cross-sectional study. The inclusion criteria were women aged between 20 and 40 years who have had sexual intercourse, nulliparous, BMI lower than 25 kg/m2, and absence of pelvic floor dysfunction. The evaluation consisted of both the medical history and assessment of the PFM functionality using the Perina pressure biofeedback and Oxford Scale. We measured sexual satisfaction using the Female Sexual Quotient questionnaire and used the KolmogorovSmirnov test to verify the normality of the data. We analyzed non-parametric variables using the Spearman correlation test. The significance level was 5 %.
A total of 80 women with a median age of 26 years and median BMI of 21.64 kg/m2 participated in this study. We divided the subjects into two groups, best and worse PFM functionality, according to median Perina pressure biofeedback and Oxford scale. We found no difference between the groups when comparing the sexual satisfaction scores. There was only a slight significant correlation between the Contraction Voluntary Average obtained using the pressure biofeedback and the primary domain (r = 0.27; p = 0.01).
This study found a slight correlation between PFM functionality and the functionality of the primary domain of the Female Sexual Quotient questionnaire. Therefore, it is not possible to state whether there is an association between the PFM functionality and female sexual satisfaction in young adults.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):170-176
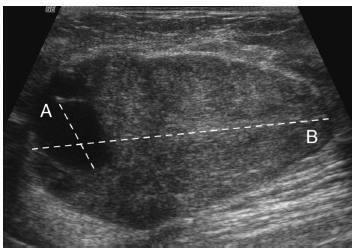
The objective of this study is to assess whether the largest cyst diameter is useful for BI-RADS ultrasonography classification of predominantly solid breast masses with an oval shape, circumscribed margins, and largest axis parallel to the skin, which, except for the cystic component, would be likely classified as benign.
This study received approval from the local institutional review board. From March 2009 to August 2014, we prospectively biopsied 170 breast masses from 164 women. We grouped the largest cyst and mass diameters according to histopathological diagnoses. We used Student's t-test, linear regression, and the area under the receiver operating characteristic curve (AUC) for statistical assessment.
Histopathological examination revealed 143 (84%) benign and 27 (16%) malignant masses. The mean largest mass diameter was larger among malignant (mean standard deviation, 34.1 16.6 mm) than benign masses (24.7 16.7 mm) (P < 0.008). The mean largest cyst diameter was also larger among malignant (9.9 7.1 mm) than benign masses (4.6 3.6 mm) (P < 0.001). Agreement between measurements of the largest mass and cyst diameters was low (R2 = 0.26). AUC for the largest cyst diameter (0.78) was similar to the AUC for the largest mass diameter (0.69) ( p = 0.2). A largest cyst diameter < 3, 3 to < 11, and 11 mm had a positive predictive value of 0, 15, and 52%, respectively.
A largest cystic component < 3 mm identified within breast masses that show favorable characteristics may be considered clinically inconsequential in ultrasonography characterization. Conversely, masses with a largest cystic component 3 mm should be classified as BI-RADS-US category 4.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):170-176
The objective of this study is to assess whether the largest cyst diameter is useful for BI-RADS ultrasonography classification of predominantly solid breast masses with an oval shape, circumscribed margins, and largest axis parallel to the skin, which, except for the cystic component, would be likely classified as benign.
This study received approval from the local institutional review board. From March 2009 to August 2014, we prospectively biopsied 170 breast masses from 164 women. We grouped the largest cyst and mass diameters according to histopathological diagnoses. We used Student's t-test, linear regression, and the area under the receiver operating characteristic curve (AUC) for statistical assessment.
Histopathological examination revealed 143 (84%) benign and 27 (16%) malignant masses. The mean largest mass diameter was larger among malignant (mean standard deviation, 34.1 16.6 mm) than benign masses (24.7 16.7 mm) (P < 0.008). The mean largest cyst diameter was also larger among malignant (9.9 7.1 mm) than benign masses (4.6 3.6 mm) (P < 0.001). Agreement between measurements of the largest mass and cyst diameters was low (R2 = 0.26). AUC for the largest cyst diameter (0.78) was similar to the AUC for the largest mass diameter (0.69) ( p = 0.2). A largest cyst diameter < 3, 3 to < 11, and 11 mm had a positive predictive value of 0, 15, and 52%, respectively.
A largest cystic component < 3 mm identified within breast masses that show favorable characteristics may be considered clinically inconsequential in ultrasonography characterization. Conversely, masses with a largest cystic component 3 mm should be classified as BI-RADS-US category 4.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):177-182
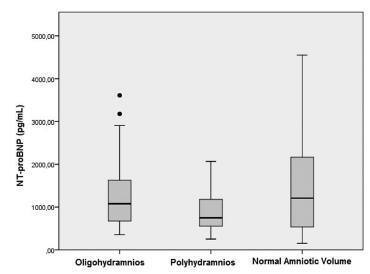
The amniotic fluid volume (AFV) is known as a predictor for the wellness of a fetus. We aimed to investigate whether N-terminal pro-brain natriuretic peptide (NTproBNP) levels reflect AFV abnormalities in otherwise normal fetuses.
We recruited 24 women with isolated oligohydramnios, 23 women with isolated polyhydramnios, and 36 women with normal AFV at a tertiary referral center. NT-proBNP levels in umbilical venous samples and the individual characteristics of the three groups were compared. One-way ANOVA and Kruskal-Wallis analysis of variance were used for multi-group comparisons of continuous variables. When a significant difference was detected, the Scheffe test was performed as a post-hoc analysis. Proportions were compared using the Chi-square (2) test.
Maternal age, body mass indices, weight gained in pregnancy and NT-proBNP levels were similar among the three groups. Apgar scores at 1 and 5 minutes significantly correlated with NT-proBNP levels in all newborns (Spearman's r = 0.23 ; p = 0.03 and Spearman's r = 0.24; p = 0.02, respectively). The umbilical venous NTproBNP levels did not differ between newborns who needed mechanical ventilation and those who didn't (p = 0.595).
NT-proBNP is a biomolecule that may provide insights into the pathogenesis of fetal circulatory problems and subsequent renal failure. Further investigations are warranted.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):177-182
The amniotic fluid volume (AFV) is known as a predictor for the wellness of a fetus. We aimed to investigate whether N-terminal pro-brain natriuretic peptide (NTproBNP) levels reflect AFV abnormalities in otherwise normal fetuses.
We recruited 24 women with isolated oligohydramnios, 23 women with isolated polyhydramnios, and 36 women with normal AFV at a tertiary referral center. NT-proBNP levels in umbilical venous samples and the individual characteristics of the three groups were compared. One-way ANOVA and Kruskal-Wallis analysis of variance were used for multi-group comparisons of continuous variables. When a significant difference was detected, the Scheffe test was performed as a post-hoc analysis. Proportions were compared using the Chi-square (2) test.
Maternal age, body mass indices, weight gained in pregnancy and NT-proBNP levels were similar among the three groups. Apgar scores at 1 and 5 minutes significantly correlated with NT-proBNP levels in all newborns (Spearman's r = 0.23 ; p = 0.03 and Spearman's r = 0.24; p = 0.02, respectively). The umbilical venous NTproBNP levels did not differ between newborns who needed mechanical ventilation and those who didn't (p = 0.595).
NT-proBNP is a biomolecule that may provide insights into the pathogenesis of fetal circulatory problems and subsequent renal failure. Further investigations are warranted.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):183-188
The purpose of this study was to evaluate the perinatal outcomes in pregnant women who use illicit drugs.
A retrospective observational study of patients who, at the time of delivery, were sent to or who spontaneously sought a public maternity hospital in the eastern area of São Paulo city. We compared the perinatal outcomes of two distinct groups of pregnant women - illicit drugs users and non-users - that gave birth in the same period and analyzed the obstetric and neonatal variables. We used Student's t-test to calculate the averages among the groups, and the Chi-square test or Fisher's exact test to compare categorical data from each group.
We analyzed 166 women (83 users and 83 non-users) in both groups with a mean of age of 26 years. Ninety-five percent of the drug users would use crack or pure cocaine alone or associated with other psychoactive substances during pregnancy. Approximately half of the users group made no prenatal visit, compared with 2.4% in the non-users group (p < 0.001). Low birth weight (2,620 g versus 3,333 g on average, p < 0.001) and maternal syphilis (15.7% versus 0%, p < 0.001) were associated with the use of these illicit drugs.
The use of illicit drugs, mainly crack cocaine, represents an important perinatal risk. Any medical intervention in this population should combine adherence to prenatal care with strategies for reducing maternal exposure to illicit drugs.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):183-188
The purpose of this study was to evaluate the perinatal outcomes in pregnant women who use illicit drugs.
A retrospective observational study of patients who, at the time of delivery, were sent to or who spontaneously sought a public maternity hospital in the eastern area of São Paulo city. We compared the perinatal outcomes of two distinct groups of pregnant women - illicit drugs users and non-users - that gave birth in the same period and analyzed the obstetric and neonatal variables. We used Student's t-test to calculate the averages among the groups, and the Chi-square test or Fisher's exact test to compare categorical data from each group.
We analyzed 166 women (83 users and 83 non-users) in both groups with a mean of age of 26 years. Ninety-five percent of the drug users would use crack or pure cocaine alone or associated with other psychoactive substances during pregnancy. Approximately half of the users group made no prenatal visit, compared with 2.4% in the non-users group (p < 0.001). Low birth weight (2,620 g versus 3,333 g on average, p < 0.001) and maternal syphilis (15.7% versus 0%, p < 0.001) were associated with the use of these illicit drugs.
The use of illicit drugs, mainly crack cocaine, represents an important perinatal risk. Any medical intervention in this population should combine adherence to prenatal care with strategies for reducing maternal exposure to illicit drugs.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):189-195
Previous studies have shown that low birth weight (LBW) is associated with cardiovascular risk in late adulthood. Recent studies in adolescents suggest that modifiable factors may have greater influence on increased cardiovascular risk. This study aims to investigate the association between LBW and changes in anthropometric and biochemical risk factors during adolescence in a population with low average socioeconomic status.
In a retrospective double cohort, data of birth weight were extracted from hospital records of children born on the same day between 1992 and 2002. According to the World Health Organization, we classified the children as having LBW or normal birth weight. A total of 172 subjects among children, adolescents and adults were researched. We measured anthropometric and clinical data, lipid profile and glucose after an overnight fasting. The low and normal weight groups were compared using Mann-Whitney U, Fischer exact, Chi-square (2) and Student's t tests.
Pregnant women with preeclampsia delivered more newborns with LBW (p< 0.001). Anthropometric and clinical parameters were similar between groups. No differences were found in the family history of cardiovascular diseases (p= 0.1), family incomes (p= 0.8) and maternal school education (p= 0.8) between groups.
In this study, LBW did not increase cardiovascular disease risk factors in adolescents. We observed absence of association between low birth weight and poor health outcomes among adolescents with low socioeconomic status from an urban city in the Brazilian northeast.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(4):189-195
Previous studies have shown that low birth weight (LBW) is associated with cardiovascular risk in late adulthood. Recent studies in adolescents suggest that modifiable factors may have greater influence on increased cardiovascular risk. This study aims to investigate the association between LBW and changes in anthropometric and biochemical risk factors during adolescence in a population with low average socioeconomic status.
In a retrospective double cohort, data of birth weight were extracted from hospital records of children born on the same day between 1992 and 2002. According to the World Health Organization, we classified the children as having LBW or normal birth weight. A total of 172 subjects among children, adolescents and adults were researched. We measured anthropometric and clinical data, lipid profile and glucose after an overnight fasting. The low and normal weight groups were compared using Mann-Whitney U, Fischer exact, Chi-square (2) and Student's t tests.
Pregnant women with preeclampsia delivered more newborns with LBW (p< 0.001). Anthropometric and clinical parameters were similar between groups. No differences were found in the family history of cardiovascular diseases (p= 0.1), family incomes (p= 0.8) and maternal school education (p= 0.8) between groups.
In this study, LBW did not increase cardiovascular disease risk factors in adolescents. We observed absence of association between low birth weight and poor health outcomes among adolescents with low socioeconomic status from an urban city in the Brazilian northeast.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(3):120-126
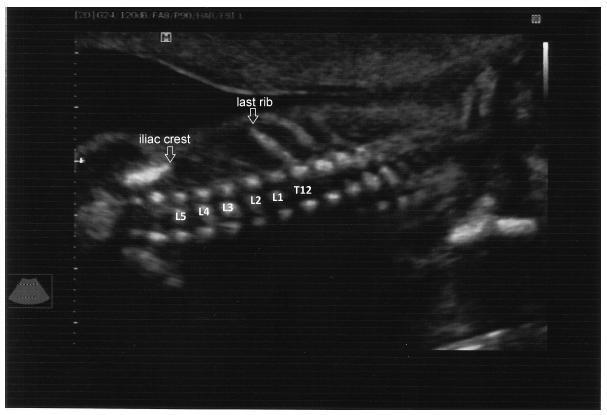
To evaluate the precision of both two- and three-dimensional ultrasonography in determining vertebral lesion level (the first open vertebra) in patients with spina bifida.
This was a prospective longitudinal study comprising of fetuses with open spina bifida who were treated in the fetal medicine division of the department of obstetrics of Hospital das Clínicas of the Universidade de São Paulo between 2004 and 2013. Vertebral lesion level was established by using both two- and three-dimensional ultrasonography in 50 fetuses (two examiners in each method). The lesion level in the neonatal period was established by radiological assessment of the spine. All pregnancies were followed in our hospital prenatally, and delivery was scheduled to allow immediate postnatal surgical correction.
Two-dimensional sonography precisely estimated the spina bifida level in 53% of the cases. The estimate error was within one vertebra in 80% of the cases, in up to two vertebrae in 89%, and in up to three vertebrae in 100%, showing a good interobserver agreement. Three-dimensional ultrasonography precisely estimated the lesion level in 50% of the cases. The estimate error was within one vertebra in 82% of the cases, in up to two vertebrae in 90%, and in up to three vertebrae in 100%, also showing good interobserver agreement. Whenever an estimate error was observed, both two- and three-dimensional ultrasonography scans tended to underestimate the true lesion level (55.3% and 62% of the cases, respectively).
No relevant difference in diagnostic performance was observed between the two- and three-dimensional ultrasonography. The use of three-dimensional ultrasonography showed no additional benefit in diagnosing the lesion level in the fetuses with spina bifida. Errors in both methods showed a tendency to underestimate lesion level.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(3):120-126
To evaluate the precision of both two- and three-dimensional ultrasonography in determining vertebral lesion level (the first open vertebra) in patients with spina bifida.
This was a prospective longitudinal study comprising of fetuses with open spina bifida who were treated in the fetal medicine division of the department of obstetrics of Hospital das Clínicas of the Universidade de São Paulo between 2004 and 2013. Vertebral lesion level was established by using both two- and three-dimensional ultrasonography in 50 fetuses (two examiners in each method). The lesion level in the neonatal period was established by radiological assessment of the spine. All pregnancies were followed in our hospital prenatally, and delivery was scheduled to allow immediate postnatal surgical correction.
Two-dimensional sonography precisely estimated the spina bifida level in 53% of the cases. The estimate error was within one vertebra in 80% of the cases, in up to two vertebrae in 89%, and in up to three vertebrae in 100%, showing a good interobserver agreement. Three-dimensional ultrasonography precisely estimated the lesion level in 50% of the cases. The estimate error was within one vertebra in 82% of the cases, in up to two vertebrae in 90%, and in up to three vertebrae in 100%, also showing good interobserver agreement. Whenever an estimate error was observed, both two- and three-dimensional ultrasonography scans tended to underestimate the true lesion level (55.3% and 62% of the cases, respectively).
No relevant difference in diagnostic performance was observed between the two- and three-dimensional ultrasonography. The use of three-dimensional ultrasonography showed no additional benefit in diagnosing the lesion level in the fetuses with spina bifida. Errors in both methods showed a tendency to underestimate lesion level.