Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo65
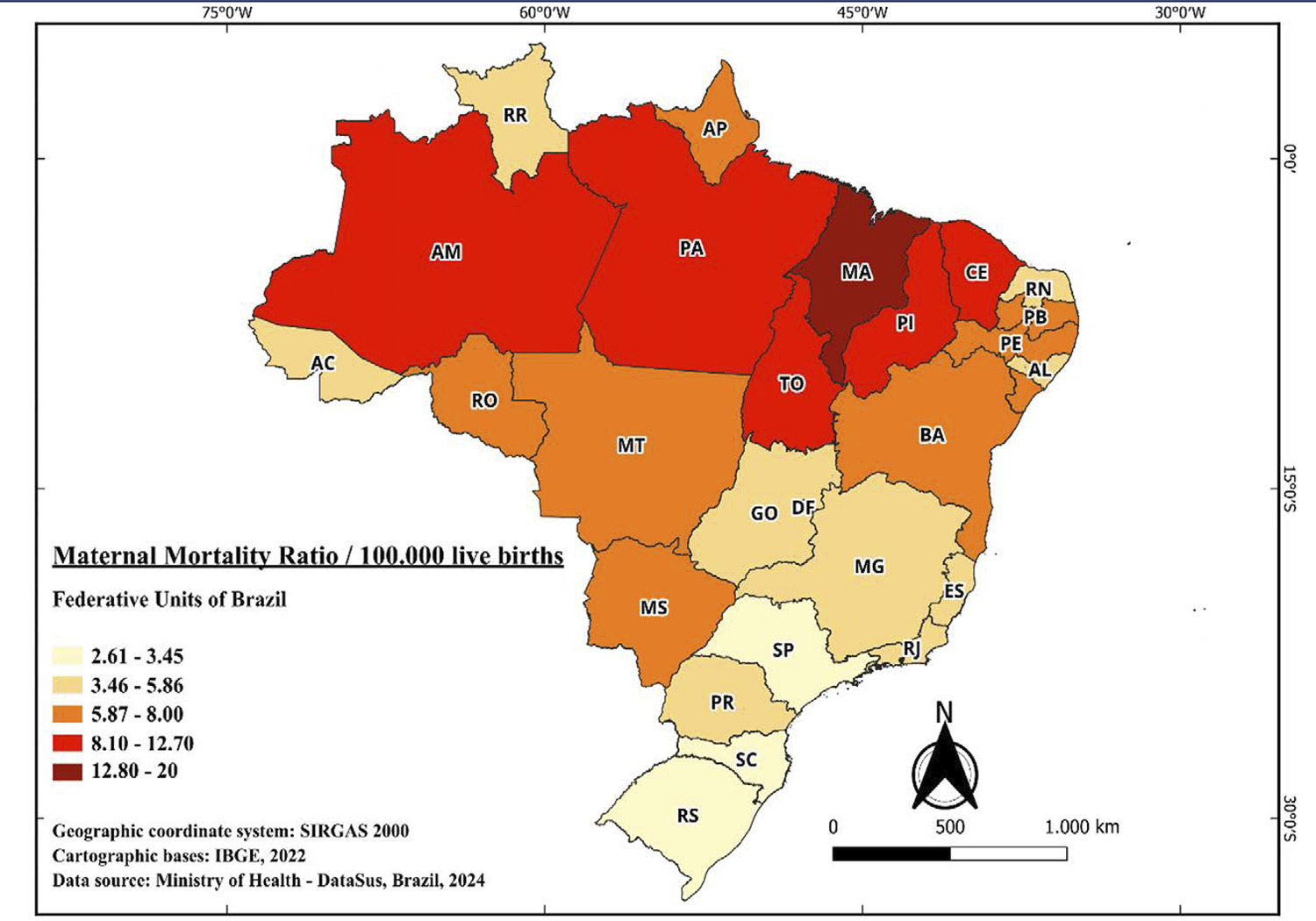
Eclampsia is a hypertensive disorder that occurs during pregnancy and can lead to death. The literature has gaps by not providing comprehensive data on the epidemiology of the disease, restricting analysis to limited temporal intervals and geographical locations. This study aims to characterize the epidemiological profile of women who died from eclampsia in Brazil from 2000 to 2021.
The maternal mortality data were obtained from the Sistema de Informações sobre Mortalidade, with the following variables of interest selected: “Federative Unit,” “Year,” “Age Range,” “Race/Color,” and “Education Level.” The collection of the number of live births for data normalization was conducted in the Sistema de Informações sobre Nascidos Vivos. Statistical analyses were performed using GraphPad Prism, calculating odds ratio for variables and fixing number of deaths per 100,000 live births for calculating maternal mortality ratio (MMR).
There was a downward trend in maternal mortality rate during the study period. Maranhão stood out as the federative unit with the highest MMR (17 deaths per 100.000 live births). Mothers aged between 40 and 49 years (OR = 3.55, CI: 3.11–4.05) presents higher MMR. Additionally, black women showed the highest MMR (OR = 4.67, CI: 4.18–5.22), as well as mothers with no educational background (OR = 5.83, CI: 4.82–7.06).
The epidemiological profile studied is predominantly composed of mothers with little or no formal education, self-declared as Black, residing in needy states and with advanced aged. These data are useful for formulating public policies aimed at combating the issue.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo65
Eclampsia is a hypertensive disorder that occurs during pregnancy and can lead to death. The literature has gaps by not providing comprehensive data on the epidemiology of the disease, restricting analysis to limited temporal intervals and geographical locations. This study aims to characterize the epidemiological profile of women who died from eclampsia in Brazil from 2000 to 2021.
The maternal mortality data were obtained from the Sistema de Informações sobre Mortalidade, with the following variables of interest selected: “Federative Unit,” “Year,” “Age Range,” “Race/Color,” and “Education Level.” The collection of the number of live births for data normalization was conducted in the Sistema de Informações sobre Nascidos Vivos. Statistical analyses were performed using GraphPad Prism, calculating odds ratio for variables and fixing number of deaths per 100,000 live births for calculating maternal mortality ratio (MMR).
There was a downward trend in maternal mortality rate during the study period. Maranhão stood out as the federative unit with the highest MMR (17 deaths per 100.000 live births). Mothers aged between 40 and 49 years (OR = 3.55, CI: 3.11–4.05) presents higher MMR. Additionally, black women showed the highest MMR (OR = 4.67, CI: 4.18–5.22), as well as mothers with no educational background (OR = 5.83, CI: 4.82–7.06).
The epidemiological profile studied is predominantly composed of mothers with little or no formal education, self-declared as Black, residing in needy states and with advanced aged. These data are useful for formulating public policies aimed at combating the issue.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo66
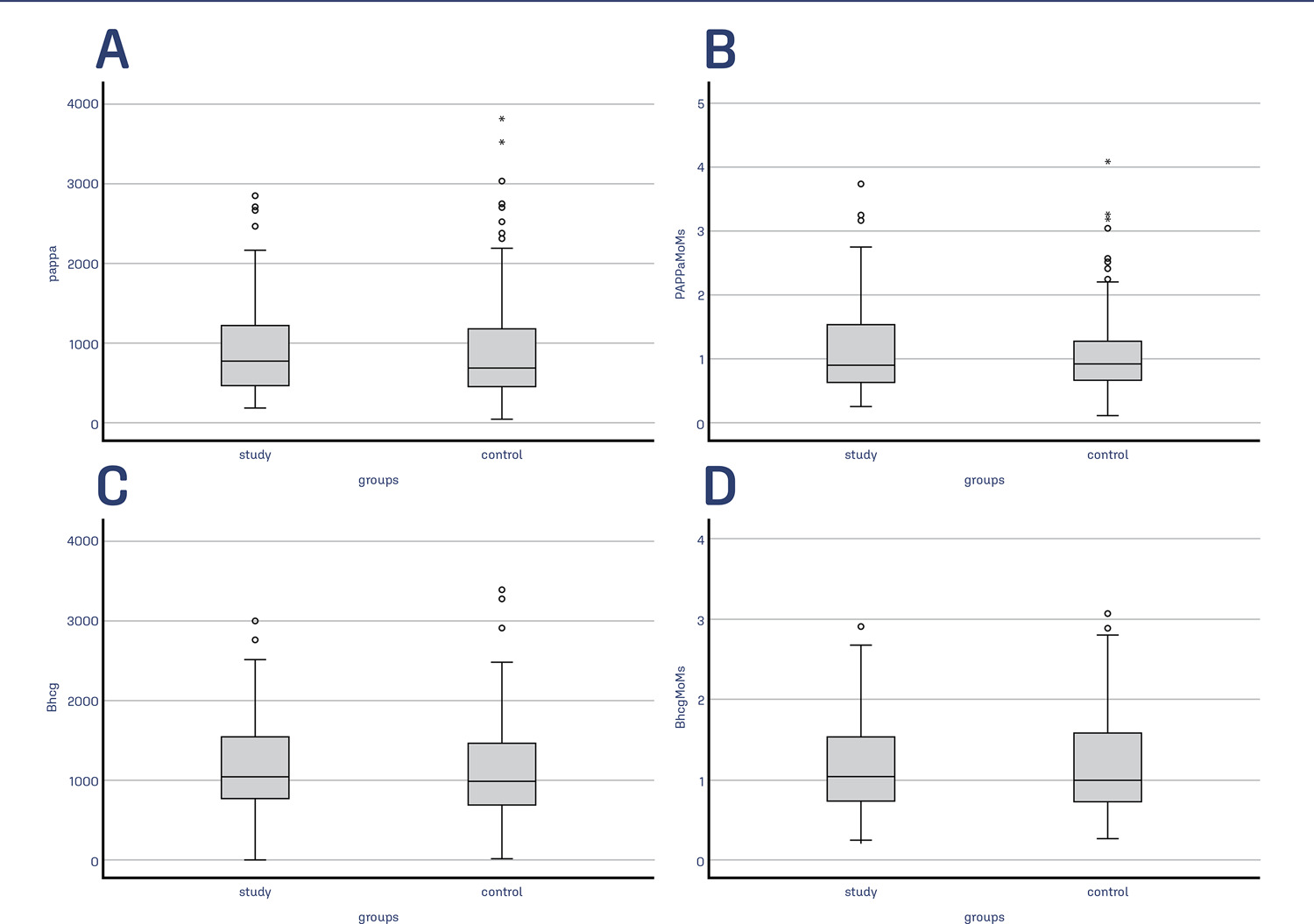
This study aimed to investigate the effects of the presence of subchorionic hematoma (SH) in early pregnancies with threatened miscarriage (TM) on levels of first-trimester maternal serum markers, pregnancy-associated plasma protein-A (PAPP-A), and free β-human chorionic gonadotropin (β-hCG) levels.
The data of TM cases with SH in the first trimester between 2015 and 2021 were evaluated retrospectively. The data of age and gestational age-matched TM cases without SH were also assessed to constitute a control group. Demographic characteristics, obstetric histories, ultrasonographic findings, and free β-hCG and PAPP-A levels of the groups were compared.
There were 119 cases in the study group and 153 cases in the control group. The median vertical and longitudinal lengths of the SH were 31 mm and 16 mm. The median age of both groups was similar (p=0.422). The MoM value of PAPP-A was 0.088 (.93) in the study group and 0.9 (0.63) in the control group (p=0.519). Similarly, the MoM value of free β-hCG was 1.04 (0.78) in the study group and 0.99 (0.86) in the control group (p=0.66). No significant relationship was found in the multivariate analysis between free β-hCG MoM, PAPP-A MoM, age, gravida, and vertical and longitudinal lengths of the hematoma (p>0.05).
The level of PAPP-A and free β-hCG were not affected by the SH. Therefore, these markers can be used reliably in TM cases with SH for the first-trimester fetal aneuploidy screening test.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo66
This study aimed to investigate the effects of the presence of subchorionic hematoma (SH) in early pregnancies with threatened miscarriage (TM) on levels of first-trimester maternal serum markers, pregnancy-associated plasma protein-A (PAPP-A), and free β-human chorionic gonadotropin (β-hCG) levels.
The data of TM cases with SH in the first trimester between 2015 and 2021 were evaluated retrospectively. The data of age and gestational age-matched TM cases without SH were also assessed to constitute a control group. Demographic characteristics, obstetric histories, ultrasonographic findings, and free β-hCG and PAPP-A levels of the groups were compared.
There were 119 cases in the study group and 153 cases in the control group. The median vertical and longitudinal lengths of the SH were 31 mm and 16 mm. The median age of both groups was similar (p=0.422). The MoM value of PAPP-A was 0.088 (.93) in the study group and 0.9 (0.63) in the control group (p=0.519). Similarly, the MoM value of free β-hCG was 1.04 (0.78) in the study group and 0.99 (0.86) in the control group (p=0.66). No significant relationship was found in the multivariate analysis between free β-hCG MoM, PAPP-A MoM, age, gravida, and vertical and longitudinal lengths of the hematoma (p>0.05).
The level of PAPP-A and free β-hCG were not affected by the SH. Therefore, these markers can be used reliably in TM cases with SH for the first-trimester fetal aneuploidy screening test.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo51
To assess the prevalence and type of chromosomal abnormalities in Brazilian couples with recurrent pregnancy loss (RPL) and compare the clinical characteristics of couples with and without chromosome abnormalities.
We assessed the medical records of 127 couples with a history of two or more miscarriages, referred to a tertiary academic hospital in Belo Horizonte, Brazil, from January 2014 to May 2023. Karyotype was generated from peripheral blood lymphocyte cultures, and cytogenetic analysis was performed according to standard protocols by heat-denatured Giemsa (RHG) banding.
Abnormal karyotypes were detected in 10 couples (7.8%). The prevalence of chromosomal abnormalities was higher among females (6.3%) compared to males (2.0%), but this difference was not statistically significant (p=0.192). The mean number of miscarriages was. 3.3 ± 1.1 in couples with chromosome abnormalities and 3.1 ± 1.5 in couples without chromosome abnormalities (p=0.681). Numerical chromosomal anomalies (6 cases) were more frequent than structural anomalies. Four women presented low-grade Turner mosaicism. No differences were found between couples with and without karyotype alterations, except for maternal age, which was higher in the group with chromosome alterations.
The prevalence of parental chromosomal alterations in our study was higher than in most series described in the literature and was associated with increased maternal age. These findings suggest that karyotyping should be part of the investigation for Brazilian couples with RPL, as identifying the genetic etiology may have implications for subsequent pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo51
To assess the prevalence and type of chromosomal abnormalities in Brazilian couples with recurrent pregnancy loss (RPL) and compare the clinical characteristics of couples with and without chromosome abnormalities.
We assessed the medical records of 127 couples with a history of two or more miscarriages, referred to a tertiary academic hospital in Belo Horizonte, Brazil, from January 2014 to May 2023. Karyotype was generated from peripheral blood lymphocyte cultures, and cytogenetic analysis was performed according to standard protocols by heat-denatured Giemsa (RHG) banding.
Abnormal karyotypes were detected in 10 couples (7.8%). The prevalence of chromosomal abnormalities was higher among females (6.3%) compared to males (2.0%), but this difference was not statistically significant (p=0.192). The mean number of miscarriages was. 3.3 ± 1.1 in couples with chromosome abnormalities and 3.1 ± 1.5 in couples without chromosome abnormalities (p=0.681). Numerical chromosomal anomalies (6 cases) were more frequent than structural anomalies. Four women presented low-grade Turner mosaicism. No differences were found between couples with and without karyotype alterations, except for maternal age, which was higher in the group with chromosome alterations.
The prevalence of parental chromosomal alterations in our study was higher than in most series described in the literature and was associated with increased maternal age. These findings suggest that karyotyping should be part of the investigation for Brazilian couples with RPL, as identifying the genetic etiology may have implications for subsequent pregnancies.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo53
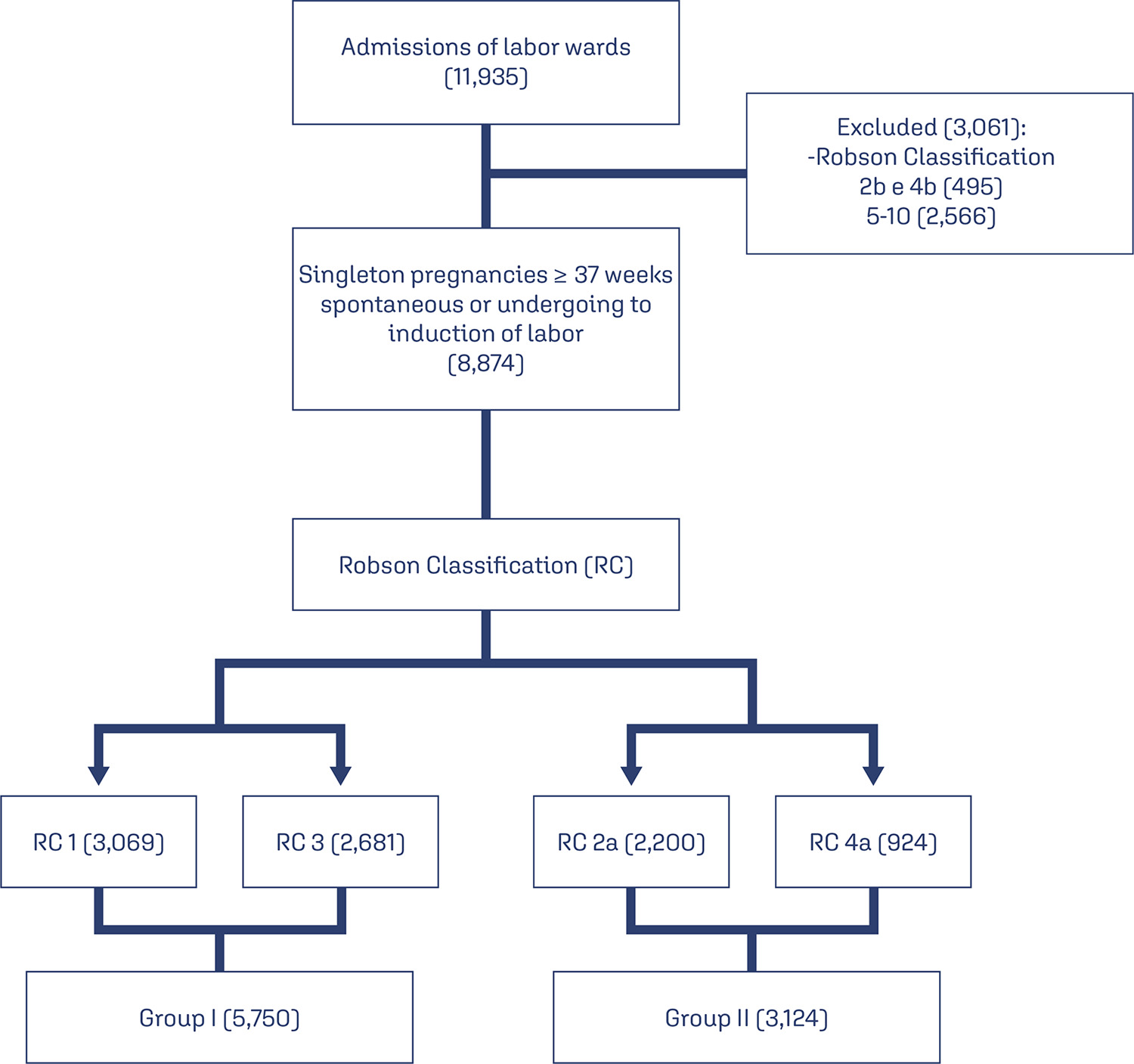
To evaluate the risk factors for postpartum hemorrhage (PPH) according to the Robson Classification in a low-risk maternity hospital.
We conducted retrospective cohort study by analyzing the medical records of pregnant women attended in a low-risk maternity hospital, during from November 2019 to November 2021. Variables analyzed were: maternal age, type of delivery, birth weight, parity, Robson Classification, and causes of PPH. We compared the occurrence of PPH between pregnant women with spontaneous (Groups 1 and 3) and with induction of labor (2a and 4a). Chi-square and Student t-tests were performed. Variables were compared using binary logistic regression.
There were 11,935 deliveries during the study period. According to Robson’s Classification, 48.2% were classified as 1 and 3 (Group I: 5,750/11,935) and 26.1% as 2a and 4a (Group II: 3,124/11,935). Group II had higher prevalence of PPH than Group I (3.5 vs. 2.7%, p=0.028). Labor induction increased the occurrence of PPH by 18.8% (RR: 1.188, 95% CI: 1.02-1.36, p=0.030). Model including forceps delivery [x2(3)=10.6, OR: 7.26, 95%CI: 3.32-15.84, R2 Nagelkerke: 0.011, p<0.001] and birth weight [x2(4)=59.0, OR: 1.001, 95%CI:1.001-1.001, R2 Nagelkerke: 0.033, p<0.001] was the best for predicting PPH in patients classified as Robson 1, 3, 2a, and 4a. Birth weight was poor predictor of PPH (area under ROC curve: 0.612, p<0.001, 95%CI: 0.572-0.653).
Robson Classification 2a and 4a showed the highest rates of postpartum hemorrhage. The model including forceps delivery and birth weight was the best predictor for postpartum hemorrhage in Robson Classification 1, 3, 2a, and 4a.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo53
To evaluate the risk factors for postpartum hemorrhage (PPH) according to the Robson Classification in a low-risk maternity hospital.
We conducted retrospective cohort study by analyzing the medical records of pregnant women attended in a low-risk maternity hospital, during from November 2019 to November 2021. Variables analyzed were: maternal age, type of delivery, birth weight, parity, Robson Classification, and causes of PPH. We compared the occurrence of PPH between pregnant women with spontaneous (Groups 1 and 3) and with induction of labor (2a and 4a). Chi-square and Student t-tests were performed. Variables were compared using binary logistic regression.
There were 11,935 deliveries during the study period. According to Robson’s Classification, 48.2% were classified as 1 and 3 (Group I: 5,750/11,935) and 26.1% as 2a and 4a (Group II: 3,124/11,935). Group II had higher prevalence of PPH than Group I (3.5 vs. 2.7%, p=0.028). Labor induction increased the occurrence of PPH by 18.8% (RR: 1.188, 95% CI: 1.02-1.36, p=0.030). Model including forceps delivery [x2(3)=10.6, OR: 7.26, 95%CI: 3.32-15.84, R2 Nagelkerke: 0.011, p<0.001] and birth weight [x2(4)=59.0, OR: 1.001, 95%CI:1.001-1.001, R2 Nagelkerke: 0.033, p<0.001] was the best for predicting PPH in patients classified as Robson 1, 3, 2a, and 4a. Birth weight was poor predictor of PPH (area under ROC curve: 0.612, p<0.001, 95%CI: 0.572-0.653).
Robson Classification 2a and 4a showed the highest rates of postpartum hemorrhage. The model including forceps delivery and birth weight was the best predictor for postpartum hemorrhage in Robson Classification 1, 3, 2a, and 4a.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo42
To evaluate the effects of surgical treatment of deep endometriosis on the metabolic profile, quality of life and psychological aspects.
Prospective observational study, carried out with women of reproductive age diagnosed with deep endometriosis, treated in a specialized outpatient clinic, from October/2020 to September/2022, at a University Hospital in Fortaleza - Brazil. Standardized questionnaires were applied to collect data on quality of life and mental health, in addition to laboratory tests to evaluate dyslipidemia and dysglycemia, at two moments, preoperatively and six months after surgery. The results were presented using tables, averages and percentages.
Thirty women with an average age of 38.5 years were evaluated. Seven quality of life domains showed improved scores: pain, control and impotence, well-being, social support, self-image, work life and sexual relations after surgery (ES ≥ 0.80). There was an improvement in mental health status with a significant reduction in anxiety and depression postoperatively. With the metabolic profile, all average levels were lower after surgery: total cholesterol 8.2% lower, LDL 12.8% lower, triglycerides 10.9% lower, and fasting blood glucose 7.3% lower (p < 0.001).
Surgical treatment of deep endometriosis improved the quality of life and psychological aspects of patients. The lipid profile of patients after laparoscopy was favorable when compared to the preoperative lipid profile.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo42
To evaluate the effects of surgical treatment of deep endometriosis on the metabolic profile, quality of life and psychological aspects.
Prospective observational study, carried out with women of reproductive age diagnosed with deep endometriosis, treated in a specialized outpatient clinic, from October/2020 to September/2022, at a University Hospital in Fortaleza - Brazil. Standardized questionnaires were applied to collect data on quality of life and mental health, in addition to laboratory tests to evaluate dyslipidemia and dysglycemia, at two moments, preoperatively and six months after surgery. The results were presented using tables, averages and percentages.
Thirty women with an average age of 38.5 years were evaluated. Seven quality of life domains showed improved scores: pain, control and impotence, well-being, social support, self-image, work life and sexual relations after surgery (ES ≥ 0.80). There was an improvement in mental health status with a significant reduction in anxiety and depression postoperatively. With the metabolic profile, all average levels were lower after surgery: total cholesterol 8.2% lower, LDL 12.8% lower, triglycerides 10.9% lower, and fasting blood glucose 7.3% lower (p < 0.001).
Surgical treatment of deep endometriosis improved the quality of life and psychological aspects of patients. The lipid profile of patients after laparoscopy was favorable when compared to the preoperative lipid profile.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo47
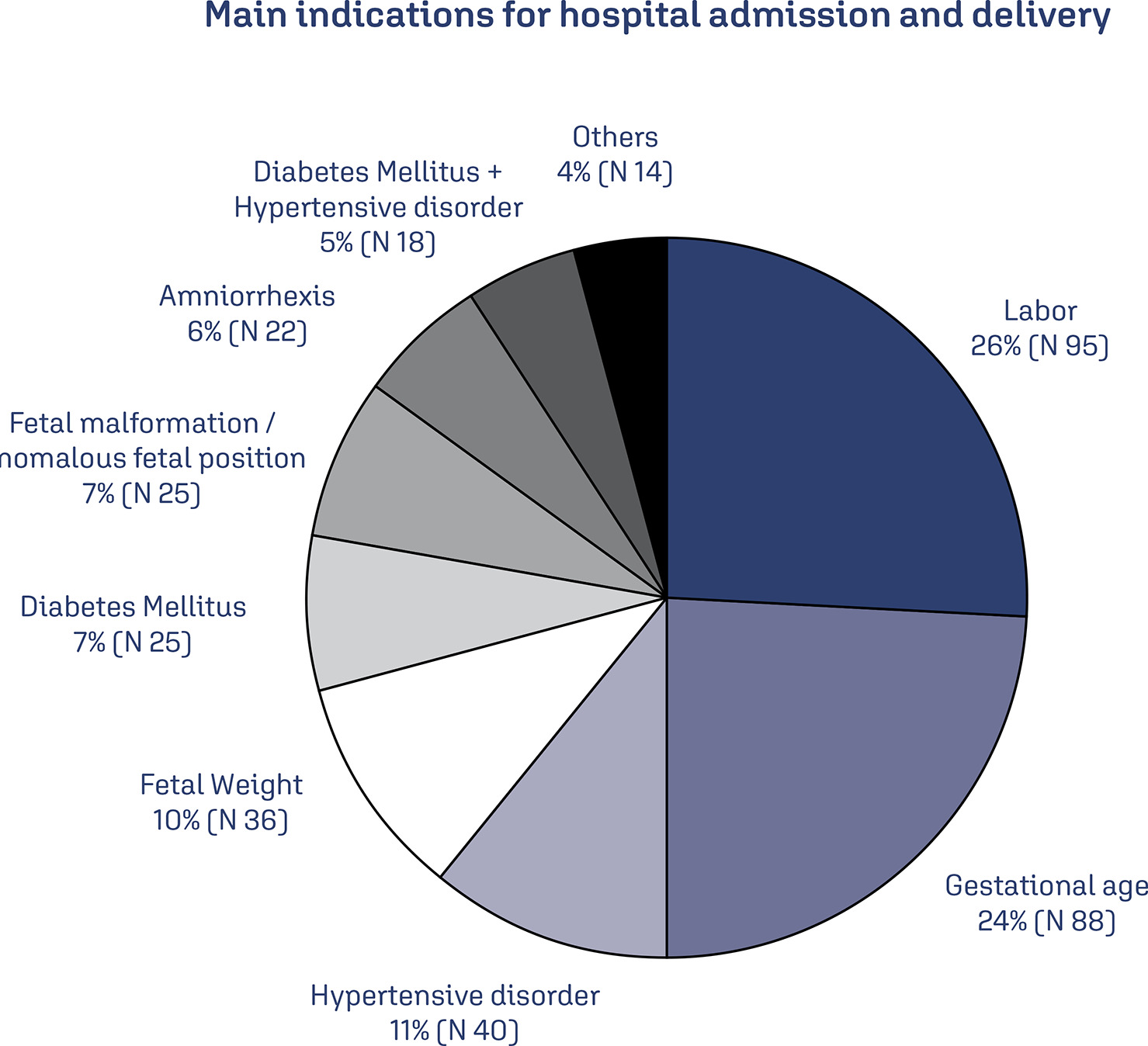
In Brazil, postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality. Data on the profile of women and risk factors associated with PPH are sparse. This study aimed to describe the profile and management of patients with PPH, and the association of risk factors for PPH with severe maternal outcomes (SMO).
A cross-sectional study was conducted in Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) obstetric intensive care unit (ICU) between January 2012 and March 2020, including patients who gave birth at the hospital and that were admitted with PPH to the ICU.
The study included 358 patients, of whom 245 (68.4%) delivered in the IMIP maternity, and 113 (31.6%) in other maternity. The mean age of the patients was 26.7 years, with up to eight years of education (46.1%) and a mean of six prenatal care. Uterine atony (72.9%) was the most common cause, 1.6% estimated blood loss, 2% calculated shock index (SI), 63.9% of patients received hemotransfusion, and 27% underwent hysterectomy. 136 cases of SMO were identified, 35.5% were classified as maternal near miss and 3.0% maternal deaths. Multiparity was associated with SMO as an antepartum risk factor (RR=1.83, 95% CI1.42-2.36). Regarding intrapartum risk factors, abruptio placentae abruption was associated with SMO (RR=2.2 95% CI1.75-2.81). Among those who had hypertension (49.6%) there was a lower risk of developing SMO.
The principal factors associated with poor maternal outcome were being multiparous and placental abruption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo47
In Brazil, postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality. Data on the profile of women and risk factors associated with PPH are sparse. This study aimed to describe the profile and management of patients with PPH, and the association of risk factors for PPH with severe maternal outcomes (SMO).
A cross-sectional study was conducted in Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) obstetric intensive care unit (ICU) between January 2012 and March 2020, including patients who gave birth at the hospital and that were admitted with PPH to the ICU.
The study included 358 patients, of whom 245 (68.4%) delivered in the IMIP maternity, and 113 (31.6%) in other maternity. The mean age of the patients was 26.7 years, with up to eight years of education (46.1%) and a mean of six prenatal care. Uterine atony (72.9%) was the most common cause, 1.6% estimated blood loss, 2% calculated shock index (SI), 63.9% of patients received hemotransfusion, and 27% underwent hysterectomy. 136 cases of SMO were identified, 35.5% were classified as maternal near miss and 3.0% maternal deaths. Multiparity was associated with SMO as an antepartum risk factor (RR=1.83, 95% CI1.42-2.36). Regarding intrapartum risk factors, abruptio placentae abruption was associated with SMO (RR=2.2 95% CI1.75-2.81). Among those who had hypertension (49.6%) there was a lower risk of developing SMO.
The principal factors associated with poor maternal outcome were being multiparous and placental abruption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo48
Evaluate the prevalence of macrosomic newborns (birth weight above 4000 grams) in a high-risk maternity from 2014 to 2019, as well as the maternal characteristics involved, risk factors, mode of delivery and associated outcomes, comparing newborns weighing 4000-4500 grams and those weighing above 4500 grams.
This is an observational study, case-control type, carried out by searching for data in hospital’s own system and clinical records. The criteria for inclusion in the study were all patients monitored at the service who had newborns with birth weight equal than or greater than 4000 grams in the period from January 2014 to December 2019, being subsequently divided into two subgroups (newborns with 4000 to 4500 grams and newborns above 4500 grams). After being collected, the variables were transcribed into a database, arranged in frequency tables. For treatment and statistical analysis of the data, Excel and R software were used. This tool was used to create graphs and tables that helped in the interpretation of the results. The statistical analysis of the variables collected included both simple descriptive analyzes as well as inferential statistics, with univariate, bivariate and multivariate analysis.
From 2014 to 2019, 3.3% of deliveries were macrosomic newborns. The average gestational age in the birth was 39.4 weeks. The most common mode of delivery (65%) was cesarean section. Diabetes mellitus was present in 30% of the deliveries studied and glycemic control was absent in most patients. Among the vaginal deliveries, only 6% were instrumented and there was shoulder dystocia in 21% of the cases. The majority (62%) of newborns had some complication, with jaundice (35%) being the most common.
Birth weight above 4000 grams had a statistically significant impact on the occurrence of neonatal complications, such as hypoglycemia, respiratory distress and 5th minute APGAR less than 7, especially if birth weight was above 4500 grams. Gestational age was also shown to be statistically significant associated with neonatal complications, the lower, the greater the risk. Thus, macrosomia is strongly linked to complications, especially neonatal complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo48
Evaluate the prevalence of macrosomic newborns (birth weight above 4000 grams) in a high-risk maternity from 2014 to 2019, as well as the maternal characteristics involved, risk factors, mode of delivery and associated outcomes, comparing newborns weighing 4000-4500 grams and those weighing above 4500 grams.
This is an observational study, case-control type, carried out by searching for data in hospital’s own system and clinical records. The criteria for inclusion in the study were all patients monitored at the service who had newborns with birth weight equal than or greater than 4000 grams in the period from January 2014 to December 2019, being subsequently divided into two subgroups (newborns with 4000 to 4500 grams and newborns above 4500 grams). After being collected, the variables were transcribed into a database, arranged in frequency tables. For treatment and statistical analysis of the data, Excel and R software were used. This tool was used to create graphs and tables that helped in the interpretation of the results. The statistical analysis of the variables collected included both simple descriptive analyzes as well as inferential statistics, with univariate, bivariate and multivariate analysis.
From 2014 to 2019, 3.3% of deliveries were macrosomic newborns. The average gestational age in the birth was 39.4 weeks. The most common mode of delivery (65%) was cesarean section. Diabetes mellitus was present in 30% of the deliveries studied and glycemic control was absent in most patients. Among the vaginal deliveries, only 6% were instrumented and there was shoulder dystocia in 21% of the cases. The majority (62%) of newborns had some complication, with jaundice (35%) being the most common.
Birth weight above 4000 grams had a statistically significant impact on the occurrence of neonatal complications, such as hypoglycemia, respiratory distress and 5th minute APGAR less than 7, especially if birth weight was above 4500 grams. Gestational age was also shown to be statistically significant associated with neonatal complications, the lower, the greater the risk. Thus, macrosomia is strongly linked to complications, especially neonatal complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo60
To analyze marital outcomes, divorce or separation, and its association with demographic, socioeconomic, and clinicopathological factors among breast cancer (BC) survivors after 2-years of diagnosis.
We performed a retrospective analysis of marital status at baseline and at years 1 and 2 of follow-up of women aged ≥ 18 years diagnosed with invasive BC participating in the AMAZONA III (GBECAM0115) study. The BC diagnosis occurred between January 2016 and March 2018 at 23 institutions in Brazil.
Of the 2974 women enrolled in AMAZONA III, 599 were married or living under common law at baseline. Divorce or separation occurred in 35 (5.8%) patients at 2 years of follow-up. In the multivariate analysis, public health insurance coverage was associated with a higher risk of marital status change (8.25% vs. 2.79%, RR 3.09, 95% CI 1.39 - 7.03, p = 0.007). Women who underwent mastectomy, adenomastectomy or skin-sparing mastectomy were associated with a higher risk of divorce or separation (8.1% vs. 4.49%, RR 1.97, 95 CI 1.04 – 3.72, p = 0.0366) than those who underwent breast-conserving surgery.
Women covered by the public health system and those who underwent mastectomy, adenomastectomy or skin-sparing mastectomy were associated with a higher risk of divorce or separation. This evidence further supports the idea that long-term marital stability is associated with a complex interplay between socioeconomic conditions and stressors, such as BC diagnosis and treatment. ClinicalTrials Registration: NCT02663973.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo60
To analyze marital outcomes, divorce or separation, and its association with demographic, socioeconomic, and clinicopathological factors among breast cancer (BC) survivors after 2-years of diagnosis.
We performed a retrospective analysis of marital status at baseline and at years 1 and 2 of follow-up of women aged ≥ 18 years diagnosed with invasive BC participating in the AMAZONA III (GBECAM0115) study. The BC diagnosis occurred between January 2016 and March 2018 at 23 institutions in Brazil.
Of the 2974 women enrolled in AMAZONA III, 599 were married or living under common law at baseline. Divorce or separation occurred in 35 (5.8%) patients at 2 years of follow-up. In the multivariate analysis, public health insurance coverage was associated with a higher risk of marital status change (8.25% vs. 2.79%, RR 3.09, 95% CI 1.39 - 7.03, p = 0.007). Women who underwent mastectomy, adenomastectomy or skin-sparing mastectomy were associated with a higher risk of divorce or separation (8.1% vs. 4.49%, RR 1.97, 95 CI 1.04 – 3.72, p = 0.0366) than those who underwent breast-conserving surgery.
Women covered by the public health system and those who underwent mastectomy, adenomastectomy or skin-sparing mastectomy were associated with a higher risk of divorce or separation. This evidence further supports the idea that long-term marital stability is associated with a complex interplay between socioeconomic conditions and stressors, such as BC diagnosis and treatment. ClinicalTrials Registration: NCT02663973.