Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):554-561
DOI 10.1590/S0100-72032013001200005
PURPOSE: To investigate the etiology and the epidemiological profile of patients with vulvovaginal candidiasis (VVC) and predisposing factors. METHODS: Vaginal secretions were streaked in Sabouraud agar and yeast samples were isolated and identified by Polymerase Chain Reaction (PCR). Demographic and clinical data were obtained with a questionnaire. For statistical analysis, the Student's t-test, the χ² and Fischer tests were applied as needed using the Statistical Package for Social Sciences (SPSS) software, with the level of significance set at 5%. RESULTS: Sixty-nine patients aged from 15 to 52 years were evaluated. They were predominantly white (79.7%), with higher education (58%), married (56.5%) and sexually active (97.1%). Among them, 34.8% were pregnant, 7.2% diabetic, 1.4% seropositive for AIDS, and 36.2% were using oral contraceptives. Recent antibiotic therapy was mentioned by 13% of the patients, and antifungal or anti-trichomonas therapy was mentioned by 5.8 and 1.4% of the patients, respectively. Corticosteroid use was reported by 2.9% and antineoplastic by 1.4%. Vaginal discharge and itching were the main complaints (97.1 and 73.9%), followed by burning (63.8%) and erythema (63.8%). When present, the vaginal flow was predominantly white (88.1%) or lumpy (86.6%). The diagnosis was confirmed by culture in 55 (79.7%) patients, with mixed infections in 4 patients. The most prevalent species was C. albicans, followed by C. glabrata (one monoinfection and two mixed infections with C. albicans). C. lusitaniae and C. albicans were also identified in mixed infections (two patients). CONCLUSION: Despite the high culture positivity and clinical data characteristic of VVC, the symptoms were not pathognomonic. C. albicans is the most prevalent species, but other species are also involved in VVC etiology, such as the emergence of C. lusitaniae.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):554-561
DOI 10.1590/S0100-72032013001200005
PURPOSE: To investigate the etiology and the epidemiological profile of patients with vulvovaginal candidiasis (VVC) and predisposing factors. METHODS: Vaginal secretions were streaked in Sabouraud agar and yeast samples were isolated and identified by Polymerase Chain Reaction (PCR). Demographic and clinical data were obtained with a questionnaire. For statistical analysis, the Student's t-test, the χ² and Fischer tests were applied as needed using the Statistical Package for Social Sciences (SPSS) software, with the level of significance set at 5%. RESULTS: Sixty-nine patients aged from 15 to 52 years were evaluated. They were predominantly white (79.7%), with higher education (58%), married (56.5%) and sexually active (97.1%). Among them, 34.8% were pregnant, 7.2% diabetic, 1.4% seropositive for AIDS, and 36.2% were using oral contraceptives. Recent antibiotic therapy was mentioned by 13% of the patients, and antifungal or anti-trichomonas therapy was mentioned by 5.8 and 1.4% of the patients, respectively. Corticosteroid use was reported by 2.9% and antineoplastic by 1.4%. Vaginal discharge and itching were the main complaints (97.1 and 73.9%), followed by burning (63.8%) and erythema (63.8%). When present, the vaginal flow was predominantly white (88.1%) or lumpy (86.6%). The diagnosis was confirmed by culture in 55 (79.7%) patients, with mixed infections in 4 patients. The most prevalent species was C. albicans, followed by C. glabrata (one monoinfection and two mixed infections with C. albicans). C. lusitaniae and C. albicans were also identified in mixed infections (two patients). CONCLUSION: Despite the high culture positivity and clinical data characteristic of VVC, the symptoms were not pathognomonic. C. albicans is the most prevalent species, but other species are also involved in VVC etiology, such as the emergence of C. lusitaniae.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):549-553
DOI 10.1590/S0100-72032013001200004
PURPOSE: To analyze the perinatal mortality rate in cases of gastroschisis and possible associated factors. METHODS: A retrospective cohort study was conducted between 1992 and 2012. All cases of gastroschisis born in Hospital de Clínicas de Porto Alegre (HCPA) during that period were included. The diagnosis of gastroschisis was obtained by morphological ultrasound examination or clinical examination at birth in prenatally unknown cases. The variables of birth (birthweight, gestational age and Apgar score, mode of delivery, type of gastroschisis and associated anomalies) and the surgical ones (type of surgical closure, reintervention and sepsis) were compared between surviving cases and deaths. The results of this comparison were analyzed according to the type of variable using parametric and non-parametric tests (Mann-Whitney or Student's t-test, χ² or Fisher's exact test), with the level of significance set at 5% (p=0.05). RESULTS: Sixty-four newborns with gastroschisis were included, 59 of them (92.2%) diagnosed during the prenatal period. Twenty-six patients (40.6%) had only exposed intestines, classified as simple gastroschisis, 22 had exposure of the intestines and stomach (34.4%) and 16 had exposure of the intestine and other organs (25%), for a total of 38 cases of complex gastroschisis. Primary surgical repair was performed in 44 cases (68.8%). The mortality rate was 23.4% (15 deaths). Babies who died had significantly lower birth weight (p=0.001), gestational age (p=0.03) and Apgar score (p=0.03) than survivors. There was no difference in mode of delivery (p=0.8) and, with respect to gut contents, there was no difference between the cases of simple and complex gastroschisis (p=0.06). Mortality was significantly higher in patients with sepsis (p=0.008) and reintervention (p=0.001). CONCLUSION: in the present study, perinatal mortality due to gastroschisis seemed to depend mainly on prematurity, low birth weight, and surgical complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):549-553
DOI 10.1590/S0100-72032013001200004
PURPOSE: To analyze the perinatal mortality rate in cases of gastroschisis and possible associated factors. METHODS: A retrospective cohort study was conducted between 1992 and 2012. All cases of gastroschisis born in Hospital de Clínicas de Porto Alegre (HCPA) during that period were included. The diagnosis of gastroschisis was obtained by morphological ultrasound examination or clinical examination at birth in prenatally unknown cases. The variables of birth (birthweight, gestational age and Apgar score, mode of delivery, type of gastroschisis and associated anomalies) and the surgical ones (type of surgical closure, reintervention and sepsis) were compared between surviving cases and deaths. The results of this comparison were analyzed according to the type of variable using parametric and non-parametric tests (Mann-Whitney or Student's t-test, χ² or Fisher's exact test), with the level of significance set at 5% (p=0.05). RESULTS: Sixty-four newborns with gastroschisis were included, 59 of them (92.2%) diagnosed during the prenatal period. Twenty-six patients (40.6%) had only exposed intestines, classified as simple gastroschisis, 22 had exposure of the intestines and stomach (34.4%) and 16 had exposure of the intestine and other organs (25%), for a total of 38 cases of complex gastroschisis. Primary surgical repair was performed in 44 cases (68.8%). The mortality rate was 23.4% (15 deaths). Babies who died had significantly lower birth weight (p=0.001), gestational age (p=0.03) and Apgar score (p=0.03) than survivors. There was no difference in mode of delivery (p=0.8) and, with respect to gut contents, there was no difference between the cases of simple and complex gastroschisis (p=0.06). Mortality was significantly higher in patients with sepsis (p=0.008) and reintervention (p=0.001). CONCLUSION: in the present study, perinatal mortality due to gastroschisis seemed to depend mainly on prematurity, low birth weight, and surgical complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):541-548
DOI 10.1590/S0100-72032013001200003
PURPOSE: To determine the prevalence of low back pain in pregnant women and to describe its characteristics and associated factors. METHODS: The participants were 269 pregnant women in the first to the third trimester of pregnancy, seen at the obstetrics outpatient clinic of a University Hospital in the Brazilian Northeast. We applied a questionnaire in order to obtain data regarding socio-demographic variables, obstetric history and characteristics of low back pain, as well as the Oswestry and Rolland Morris questionnaires to assess disability and a visual analog pain scale to measure pain intensity. RESULTS: The prevalence of low back pain was 73%, with the following characteristics: stabbing (62/31.6%), irradiation (162/82.6%), of daily frequency (105/53.5%), usually starting at night (83/42.3%) when it was also more intense (122/62.2%), and lasting about 1 hour in 118 women (60.2%). Pain improved with rest (100/51%), worsened when the women stood or sat for a long time (86/43.9%) and when they did housework (85/43.4%). The level of disability ranged from "mild" to "moderate" in most cases. Urinary tract infection (p=0.02) and the scores of the Oswestry and Rolland Morris questionnaires showed significant association with the visual analogue pain scale. CONCLUSION: The prevalence of back pain among pregnant women is high, with varying characteristics. The degree of disability is usually moderate and the presence of urinary infection and higher disability scores were associated with greater intensity of low back pain.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):541-548
DOI 10.1590/S0100-72032013001200003
PURPOSE: To determine the prevalence of low back pain in pregnant women and to describe its characteristics and associated factors. METHODS: The participants were 269 pregnant women in the first to the third trimester of pregnancy, seen at the obstetrics outpatient clinic of a University Hospital in the Brazilian Northeast. We applied a questionnaire in order to obtain data regarding socio-demographic variables, obstetric history and characteristics of low back pain, as well as the Oswestry and Rolland Morris questionnaires to assess disability and a visual analog pain scale to measure pain intensity. RESULTS: The prevalence of low back pain was 73%, with the following characteristics: stabbing (62/31.6%), irradiation (162/82.6%), of daily frequency (105/53.5%), usually starting at night (83/42.3%) when it was also more intense (122/62.2%), and lasting about 1 hour in 118 women (60.2%). Pain improved with rest (100/51%), worsened when the women stood or sat for a long time (86/43.9%) and when they did housework (85/43.4%). The level of disability ranged from "mild" to "moderate" in most cases. Urinary tract infection (p=0.02) and the scores of the Oswestry and Rolland Morris questionnaires showed significant association with the visual analogue pain scale. CONCLUSION: The prevalence of back pain among pregnant women is high, with varying characteristics. The degree of disability is usually moderate and the presence of urinary infection and higher disability scores were associated with greater intensity of low back pain.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):536-540
DOI 10.1590/S0100-72032013001200002
PURPOSE: To evaluate weight retention 12 months postpartum and factors associated among women who had received prenatal care at Health Care Centers in Porto Alegre, southern Brazil. METHODS: Pregnant women in the last trimester were identified at 20 Health Care Centers. Socioeconomic, demographic and anthropometrics data were obtained. Six and 12 months after delivery, the women received home visits for anthropometric measures. The gestational weight gain was defined by pre-pregnancy Body Mass Index (BMI). Weight retention was defined as the difference between pre-gestational weight and weight at postpartum. Data were analyzed using McNemar's Test, ANOVA with Bonferroni correction and multiple linear regression. RESULTS: Of the 715 pregnant women recruited, 545 were assessed 12 months after delivery. Women were more likely to be overweight 12 months postpartum compared to the pre-pregnancy period (52.9 versus 36.7%) and weight retention during the 12 months postpartum was more than 10 kg in 30.7% of the women. Weight retention in the postpartum period was higher among women who were overweight (9.9±7.7 kg) compared to those who were of normal weight during the pre-pregnancy period (7.6±6.2 kg). Pre-pregnancy BMI, gestational weight gain, and maternal age were associated with gestational weight retention 12 months postpartum (p<0.001). CONCLUSION: Adequate prenatal care is necessary to minimize the adverse effects of excessive weight gain during pregnancy on women's health.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(12):536-540
DOI 10.1590/S0100-72032013001200002
PURPOSE: To evaluate weight retention 12 months postpartum and factors associated among women who had received prenatal care at Health Care Centers in Porto Alegre, southern Brazil. METHODS: Pregnant women in the last trimester were identified at 20 Health Care Centers. Socioeconomic, demographic and anthropometrics data were obtained. Six and 12 months after delivery, the women received home visits for anthropometric measures. The gestational weight gain was defined by pre-pregnancy Body Mass Index (BMI). Weight retention was defined as the difference between pre-gestational weight and weight at postpartum. Data were analyzed using McNemar's Test, ANOVA with Bonferroni correction and multiple linear regression. RESULTS: Of the 715 pregnant women recruited, 545 were assessed 12 months after delivery. Women were more likely to be overweight 12 months postpartum compared to the pre-pregnancy period (52.9 versus 36.7%) and weight retention during the 12 months postpartum was more than 10 kg in 30.7% of the women. Weight retention in the postpartum period was higher among women who were overweight (9.9±7.7 kg) compared to those who were of normal weight during the pre-pregnancy period (7.6±6.2 kg). Pre-pregnancy BMI, gestational weight gain, and maternal age were associated with gestational weight retention 12 months postpartum (p<0.001). CONCLUSION: Adequate prenatal care is necessary to minimize the adverse effects of excessive weight gain during pregnancy on women's health.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):84-89
DOI 10.1590/S0100-72032014000200007
To identify and relate body fat percentage (skin fold measures), body mass index
(BMI) and age at menarcheto aerobic capacity using the indirect VO2
maximum value (VO2 max) of girls in the second cycle of primary school.
A total of 197 girls aged 13.0±1.2 years on average, students from two public
schools in the city of Atibaia in São Paulo, were evaluated. Anthropometric
evaluation of skin folds was performed using the Slaughter protocol for teenage
girls, and BMI (kg/m2) was based on "Z score" (graphic of percentile)
according to WHO recommendations. The Léger protocol was used to determine
VO2 max. Pearson linear regression and the Student t-test were used
for statistical analysis.
22.3% of the girls were overweight and 3.5% were obese according to the
classification proposed by the WHO; 140 (71.1%) girls reported menarche. The
average age at menarche was 12.0±1.0 years and was significantly higher in the
group with normal BMI (12.2±0.9 years) than in the overweight or obese groups
(11.6±1.0 years). The average indirect VO2 max value was 39.6±3.7
mL/kg/min, ranging from 30.3 to 50.5 mL/kg/min. The advance of chronological age
and early age at menarche were positively correlated with lower VO2 max
values.
This study showed that 25.8% of the girls had aBMI value above WHO
recommendations. Girls with higher BMI and higher body fat percentage had lower
VO2 max. The earlier age at menarche and the advance of
chronological age were the most important factors for the reduction of aerobic
capacity. The ageat menarche was higher in girls with adequate BMI compared
tooverweight or obese girls.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):84-89
DOI 10.1590/S0100-72032014000200007
To identify and relate body fat percentage (skin fold measures), body mass index
(BMI) and age at menarcheto aerobic capacity using the indirect VO2
maximum value (VO2 max) of girls in the second cycle of primary school.
A total of 197 girls aged 13.0±1.2 years on average, students from two public
schools in the city of Atibaia in São Paulo, were evaluated. Anthropometric
evaluation of skin folds was performed using the Slaughter protocol for teenage
girls, and BMI (kg/m2) was based on "Z score" (graphic of percentile)
according to WHO recommendations. The Léger protocol was used to determine
VO2 max. Pearson linear regression and the Student t-test were used
for statistical analysis.
22.3% of the girls were overweight and 3.5% were obese according to the
classification proposed by the WHO; 140 (71.1%) girls reported menarche. The
average age at menarche was 12.0±1.0 years and was significantly higher in the
group with normal BMI (12.2±0.9 years) than in the overweight or obese groups
(11.6±1.0 years). The average indirect VO2 max value was 39.6±3.7
mL/kg/min, ranging from 30.3 to 50.5 mL/kg/min. The advance of chronological age
and early age at menarche were positively correlated with lower VO2 max
values.
This study showed that 25.8% of the girls had aBMI value above WHO
recommendations. Girls with higher BMI and higher body fat percentage had lower
VO2 max. The earlier age at menarche and the advance of
chronological age were the most important factors for the reduction of aerobic
capacity. The ageat menarche was higher in girls with adequate BMI compared
tooverweight or obese girls.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):79-83
DOI 10.1590/S0100-72032014000200006
To investigate the presence of depressive symptoms in women with chronic pelvic
pain.
This descriptive cross-sectional study was performed with women aged 18 years or
older, diagnosed with chronic pelvic pain, with no pregnancy history in the
previous year, and with no cancer history. The sample was established by
calculating the representative sample, estimated as 50 women. All women were
undergoing treatment at a gynecology outpatient clinic, referred by the primary
health care network of the Brazilian national health system. Data collection was
performed from October2009 to May 2010. The women's sociodemographic, economic and
clinical characteristics were analyzed. Pain intensity was evaluated using a
visual analogue scale. The depressive symptoms were investigated using Beck's
Depression Inventory. Statistical analysis was performed using position measures
(mean, median), dispersion (standard deviation) and the χ2 test. Values
of p≤ .05 were considered statistically significant.
The participants' mean age was 41.6±9.4 years. The following features
predominated: secondary education level; pardo (brown) skin color; Catholic
religion; and living with a steady partner. Most (98%) were economically active
and worked with general domestic services. Regarding the participants' subjective
perception of pain, 52% reported experiencing intense pain, while 48% reported
experiencing moderate pain. Most women (52%) had been living with pain for five
years or less, and 30%, for over 11 years. The mean BDI score was 17.4 (±9.4). It
was observed that 58% of the women presented mild, moderate and severe depressive
symptoms according to the BDI. The most frequent depressive symptoms were
fatigability, loss of libido, irritability, difficulty to work, somatic
preoccupations, crying, dissatisfaction, sadness, and insomnia.
Depressive symptoms were frequent among these women suffering with chronic pelvic
pain.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):79-83
DOI 10.1590/S0100-72032014000200006
To investigate the presence of depressive symptoms in women with chronic pelvic
pain.
This descriptive cross-sectional study was performed with women aged 18 years or
older, diagnosed with chronic pelvic pain, with no pregnancy history in the
previous year, and with no cancer history. The sample was established by
calculating the representative sample, estimated as 50 women. All women were
undergoing treatment at a gynecology outpatient clinic, referred by the primary
health care network of the Brazilian national health system. Data collection was
performed from October2009 to May 2010. The women's sociodemographic, economic and
clinical characteristics were analyzed. Pain intensity was evaluated using a
visual analogue scale. The depressive symptoms were investigated using Beck's
Depression Inventory. Statistical analysis was performed using position measures
(mean, median), dispersion (standard deviation) and the χ2 test. Values
of p≤ .05 were considered statistically significant.
The participants' mean age was 41.6±9.4 years. The following features
predominated: secondary education level; pardo (brown) skin color; Catholic
religion; and living with a steady partner. Most (98%) were economically active
and worked with general domestic services. Regarding the participants' subjective
perception of pain, 52% reported experiencing intense pain, while 48% reported
experiencing moderate pain. Most women (52%) had been living with pain for five
years or less, and 30%, for over 11 years. The mean BDI score was 17.4 (±9.4). It
was observed that 58% of the women presented mild, moderate and severe depressive
symptoms according to the BDI. The most frequent depressive symptoms were
fatigability, loss of libido, irritability, difficulty to work, somatic
preoccupations, crying, dissatisfaction, sadness, and insomnia.
Depressive symptoms were frequent among these women suffering with chronic pelvic
pain.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):65-71
DOI 10.1590/S0100-72032014000200004
To analyze the relationships among gestational risk, type of delivery and
immediate maternal and neonatal repercussions.
A retrospective cohort study based on secondary data was conducted in a
university maternity hospital. A total of 1606 births were analyzed over a 9-month
period. Epidemiological, clinical, obstetric and neonatal characteristics were
compared according to the route of delivery and the gestational risk characterized
on the basis of the eligibility criteria for high clinical risk. The occurrence of
maternal and neonatal complications during hospitalization was analyzed according
to gestational risk and cesarean section delivery using univariate and
multivariate logistic analysis.
The overall rate of cesarean sections was 38.3%. High gestational risk was
present in 50.2% of births, mainly represented by hypertensive disorders and fetal
malformations. The total incidence of cesarean section, planned cesarean section
or emergency cesarean section was more frequent in pregnant women at gestational
high risk (p<0.001). Cesarean section alone did not influence maternal outcome,
but was associated with poor neonatal outcome (OR 3.4; 95%CI 2.7-4.4). Gestational
high risk was associated with poor maternal and neonatal outcome (OR 3.8; 95%CI
1.3-8.7 and OR 17.5; 95%CI 11.6-26.3, respectively). In multivariate analysis, the
ratios were maintained, although the effect of gestational risk has determined a
reduction in the OR of the type of delivery alone from 3.4 (95%CI 2.7-4.4) to 1.99
(95%CI 1.5-2.6) for adverse neonatal outcome.
Gestational risk was the main factor associated with poor maternal and neonatal
outcome. Cesarean delivery was not directly associated with poor maternal outcome
but increased the chances of unfavorable neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):65-71
DOI 10.1590/S0100-72032014000200004
To analyze the relationships among gestational risk, type of delivery and
immediate maternal and neonatal repercussions.
A retrospective cohort study based on secondary data was conducted in a
university maternity hospital. A total of 1606 births were analyzed over a 9-month
period. Epidemiological, clinical, obstetric and neonatal characteristics were
compared according to the route of delivery and the gestational risk characterized
on the basis of the eligibility criteria for high clinical risk. The occurrence of
maternal and neonatal complications during hospitalization was analyzed according
to gestational risk and cesarean section delivery using univariate and
multivariate logistic analysis.
The overall rate of cesarean sections was 38.3%. High gestational risk was
present in 50.2% of births, mainly represented by hypertensive disorders and fetal
malformations. The total incidence of cesarean section, planned cesarean section
or emergency cesarean section was more frequent in pregnant women at gestational
high risk (p<0.001). Cesarean section alone did not influence maternal outcome,
but was associated with poor neonatal outcome (OR 3.4; 95%CI 2.7-4.4). Gestational
high risk was associated with poor maternal and neonatal outcome (OR 3.8; 95%CI
1.3-8.7 and OR 17.5; 95%CI 11.6-26.3, respectively). In multivariate analysis, the
ratios were maintained, although the effect of gestational risk has determined a
reduction in the OR of the type of delivery alone from 3.4 (95%CI 2.7-4.4) to 1.99
(95%CI 1.5-2.6) for adverse neonatal outcome.
Gestational risk was the main factor associated with poor maternal and neonatal
outcome. Cesarean delivery was not directly associated with poor maternal outcome
but increased the chances of unfavorable neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):56-64
DOI 10.1590/S0100-72032014000200003
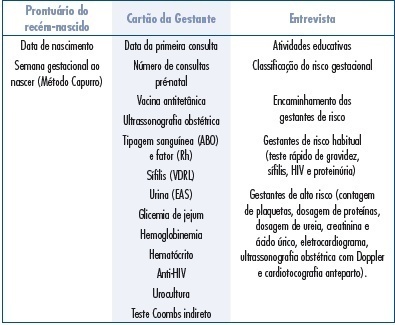
To evaluate the adequacy of the process of prenatal care according to the
parameters of the Program for the Humanization of Prenatal Care (PHPN) and of the
procedures provided by the Stork Network of Unified Health System (SUS) in the
microregion of Espirito Santo state, Brazil.
A cross-sectional study was conducted in 2012-2013 by interviewing and analyzing
the records of 742 women during the postpartum period and of their newborns in 7
hospitals in the region chosen for the research. The information was collected,
processed and analyzed by the χ2 and Fisher's exact test to determine
the difference in proportion between the criteria adopted by the PHPN and the
Stork Network and the place of residence, family income and type of coverage of
prenatal service. The level of significance was set at 5%.
The parameters showing the lowest adequacy rate were quick tests and repeated
exams, with frequencies around 10 and 30%, respectively, in addition to
educational activities (57.9%) and tetanus immunization (58.7%). In contrast, risk
management (92.6%) and the fasting plasma glucose test (91.3%) showed the best
results. Adequacy was 7.4% for the PHPN, 0.4% for the Stork Network, with respect
to the parameters of normal risk pregnancies, and 0 for high risk pregnancies.
There was a significant difference between puerperae according to housing location
regarding the execution of serology for syphilis (VDRL), anti-HIV and repeated
fasting glucose tests, and monthly income influenced the execution of blood
type/Rh factor tests, VDRL, hematocrit and anti-HIV test.
Prenatal care in the SUS proved to be inadequate regarding the procedures
required by the PHPN and Stork Network in the micro-region of a state in
southeastern Brazil, especially for women of lower income, PACS users and
residents of rural areas.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):56-64
DOI 10.1590/S0100-72032014000200003
To evaluate the adequacy of the process of prenatal care according to the
parameters of the Program for the Humanization of Prenatal Care (PHPN) and of the
procedures provided by the Stork Network of Unified Health System (SUS) in the
microregion of Espirito Santo state, Brazil.
A cross-sectional study was conducted in 2012-2013 by interviewing and analyzing
the records of 742 women during the postpartum period and of their newborns in 7
hospitals in the region chosen for the research. The information was collected,
processed and analyzed by the χ2 and Fisher's exact test to determine
the difference in proportion between the criteria adopted by the PHPN and the
Stork Network and the place of residence, family income and type of coverage of
prenatal service. The level of significance was set at 5%.
The parameters showing the lowest adequacy rate were quick tests and repeated
exams, with frequencies around 10 and 30%, respectively, in addition to
educational activities (57.9%) and tetanus immunization (58.7%). In contrast, risk
management (92.6%) and the fasting plasma glucose test (91.3%) showed the best
results. Adequacy was 7.4% for the PHPN, 0.4% for the Stork Network, with respect
to the parameters of normal risk pregnancies, and 0 for high risk pregnancies.
There was a significant difference between puerperae according to housing location
regarding the execution of serology for syphilis (VDRL), anti-HIV and repeated
fasting glucose tests, and monthly income influenced the execution of blood
type/Rh factor tests, VDRL, hematocrit and anti-HIV test.
Prenatal care in the SUS proved to be inadequate regarding the procedures
required by the PHPN and Stork Network in the micro-region of a state in
southeastern Brazil, especially for women of lower income, PACS users and
residents of rural areas.