Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(10):504-510
DOI 10.1590/S0100-72032008001000005
PURPOSE: to translate from English into Portuguese, adapt culturally and validate the Female Sexual Function Index (FSFI). METHODS: knowing the objectives of this research, two Brazilian translators have prepared a version each from the FSFI into Portuguese. Both versions have then been retro-translated into English by two English translators. After harmonizing the differences, they have been pre-tested in a pilot study. The final versions from the FSFI and from another questionnaire, the Short-Form Health Survey, which had already been translated and published in Portuguese, have then been simultaneously administered to one hundred patients, to test the FSFI psychometric proprieties concerning reliability (internal consistency and testing-retesting) and construct validity. Retesting was done after four weeks from the first interview. RESULTS: the process of cultural adaptation has not altered the Portuguese version of the FSFI, as compared to the original. The FSFI standardized Cronbach alpha was 0.96, and the evaluation by domains has varied from 0.31 to 0.97. As a measure of test-retest confidentiality, it was applied the intra-class coefficient, which has been considered strong and identical (1.0). Pearson's correlation coefficient between the FSFI and the Short-Form Health Survey was positive, but weak in most of the interrelated domains, varying from 0.017 to 0.036. CONCLUSIONS: the FSFI English version has been translated into Portuguese and culturally adapted, being reliable to evaluate the sexual response of Brazilian women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(10):504-510
DOI 10.1590/S0100-72032008001000005
PURPOSE: to translate from English into Portuguese, adapt culturally and validate the Female Sexual Function Index (FSFI). METHODS: knowing the objectives of this research, two Brazilian translators have prepared a version each from the FSFI into Portuguese. Both versions have then been retro-translated into English by two English translators. After harmonizing the differences, they have been pre-tested in a pilot study. The final versions from the FSFI and from another questionnaire, the Short-Form Health Survey, which had already been translated and published in Portuguese, have then been simultaneously administered to one hundred patients, to test the FSFI psychometric proprieties concerning reliability (internal consistency and testing-retesting) and construct validity. Retesting was done after four weeks from the first interview. RESULTS: the process of cultural adaptation has not altered the Portuguese version of the FSFI, as compared to the original. The FSFI standardized Cronbach alpha was 0.96, and the evaluation by domains has varied from 0.31 to 0.97. As a measure of test-retest confidentiality, it was applied the intra-class coefficient, which has been considered strong and identical (1.0). Pearson's correlation coefficient between the FSFI and the Short-Form Health Survey was positive, but weak in most of the interrelated domains, varying from 0.017 to 0.036. CONCLUSIONS: the FSFI English version has been translated into Portuguese and culturally adapted, being reliable to evaluate the sexual response of Brazilian women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(1):12-18
DOI 10.1590/S0100-72032008000100003
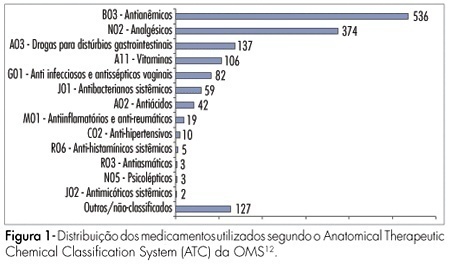
PURPOSE: to study the use of medicines by pregnant women during prenatal care in clinics of the national public health system in the city of Natal, Brazil. METHODS: a total of 610 pregnant women between the first and the third trimesters of pregnancy were interviewed in the public clinics of the four sanitary districts of Natal, from May to July 2006. The data were collected by a structured questionnaire, based in use-oriented and medicine-oriented questions. The drugs were classified according to the Anatomical Therapeutic Chemical Classification System (ATC), in agreement with the gestation risk criteria from the Food and Drugs Administration (FDA). The statistical analysis was made by the chi2 test. RESULTS: a total of 1,505 drugs were used, with an average of 2.4 medications per woman. The use of at least one drug was found in 86.6% of the women. The most frequently used drugs were anti-anemics (35.6%), analgesics (24.9%), drugs for gastrointestinal disorders (9.1%) and vitamins (7%). According to the FDA classification, 42.7% belonged to category A risk, 27.1% to category B, 29.3% to category C, 0.3% to category D and none to category X. The use of medicines during the first trimester of pregnancy amounted to 43.6%. The rate of drug use increased with higher schooling level and family income. Self-medication was found in 12.2% of the drug intake and this rate was higher in the first trimester of gestation and with women with low education level and previous gestations. CONCLUSIONS: pregnant women from Natal are being exposed to a variety of medicines with uncertain safety in pregnancy. Therefore, more careful prescription is needed, to avoid possible fetal damage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(1):12-18
DOI 10.1590/S0100-72032008000100003
PURPOSE: to study the use of medicines by pregnant women during prenatal care in clinics of the national public health system in the city of Natal, Brazil. METHODS: a total of 610 pregnant women between the first and the third trimesters of pregnancy were interviewed in the public clinics of the four sanitary districts of Natal, from May to July 2006. The data were collected by a structured questionnaire, based in use-oriented and medicine-oriented questions. The drugs were classified according to the Anatomical Therapeutic Chemical Classification System (ATC), in agreement with the gestation risk criteria from the Food and Drugs Administration (FDA). The statistical analysis was made by the chi2 test. RESULTS: a total of 1,505 drugs were used, with an average of 2.4 medications per woman. The use of at least one drug was found in 86.6% of the women. The most frequently used drugs were anti-anemics (35.6%), analgesics (24.9%), drugs for gastrointestinal disorders (9.1%) and vitamins (7%). According to the FDA classification, 42.7% belonged to category A risk, 27.1% to category B, 29.3% to category C, 0.3% to category D and none to category X. The use of medicines during the first trimester of pregnancy amounted to 43.6%. The rate of drug use increased with higher schooling level and family income. Self-medication was found in 12.2% of the drug intake and this rate was higher in the first trimester of gestation and with women with low education level and previous gestations. CONCLUSIONS: pregnant women from Natal are being exposed to a variety of medicines with uncertain safety in pregnancy. Therefore, more careful prescription is needed, to avoid possible fetal damage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(8):396-401
DOI 10.1590/S0100-72032007000800003
PURPOSE: to translate and to validate the Female Sexual Function Index (FSFI) for Brazilian pregnant women. METHODS: ninety-two pregnant women attended at a low risk prenatal clinic, with diagnosis of the pregnancy confirmed by precocious ultrasonography, participated in the research. Initially, we translated the FSFI questionnaire for Portuguese language (of Brazil) in agreement with the international criteria. Cultural, conceptual and semantics adaptations of FSFI were accomplished, because of the differences of the language, so that the pregnant women understood the subjects. All the patients answered FSFI twice, in the same day, with two different interviewers, with an hour interval from one to other interview. After 7 to 14 days, the questionnaire was applied again in a second interview. Reliability (internal intra and interobserver consistence) and the validity of the constructo (to demonstrate that questionnaire measures the sexual function) were appraised. RESULTS: Cultural adaptations were necessary for us to obtain the final version. The internal intra-observer (alpha of Chronbach) consistence of the several domains oscillated from moderate to strong (0,791 to 0,911) and the interobserver consistence varied from 0,791 to 0,914. In the validation of the constructo, were obtained moderate correlations to fort among the final scores (general) of FSFI and of Female Sexual Quotient (QS-F) that has the capacity to evaluate the feminine sexual function. CONCLUSIONS: FSFI was adapted to the Portuguese language and to the Brazilian culture, presenting significant reliability and validity; it could be included and used in future studies of the Brazilian pregnant sexual function.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(8):396-401
DOI 10.1590/S0100-72032007000800003
PURPOSE: to translate and to validate the Female Sexual Function Index (FSFI) for Brazilian pregnant women. METHODS: ninety-two pregnant women attended at a low risk prenatal clinic, with diagnosis of the pregnancy confirmed by precocious ultrasonography, participated in the research. Initially, we translated the FSFI questionnaire for Portuguese language (of Brazil) in agreement with the international criteria. Cultural, conceptual and semantics adaptations of FSFI were accomplished, because of the differences of the language, so that the pregnant women understood the subjects. All the patients answered FSFI twice, in the same day, with two different interviewers, with an hour interval from one to other interview. After 7 to 14 days, the questionnaire was applied again in a second interview. Reliability (internal intra and interobserver consistence) and the validity of the constructo (to demonstrate that questionnaire measures the sexual function) were appraised. RESULTS: Cultural adaptations were necessary for us to obtain the final version. The internal intra-observer (alpha of Chronbach) consistence of the several domains oscillated from moderate to strong (0,791 to 0,911) and the interobserver consistence varied from 0,791 to 0,914. In the validation of the constructo, were obtained moderate correlations to fort among the final scores (general) of FSFI and of Female Sexual Quotient (QS-F) that has the capacity to evaluate the feminine sexual function. CONCLUSIONS: FSFI was adapted to the Portuguese language and to the Brazilian culture, presenting significant reliability and validity; it could be included and used in future studies of the Brazilian pregnant sexual function.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(5):310-315
DOI 10.1590/S0100-72032006000500008
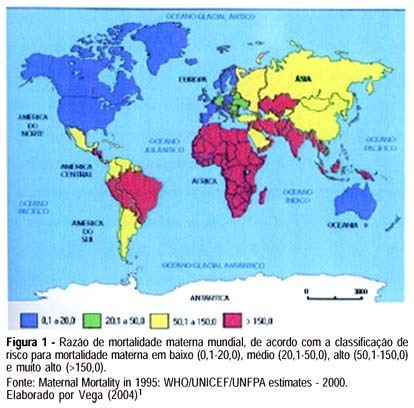
Maternal mortality rate (MM) is a health quality indicator that is directly influenced by the economic, cultural and technological level of a country. Official data of MM in Brazil, although underestimated, point to the lack of quality in pregnancy, childbirth and puerperium care services. This characteristic is common in developing countries, where poorer pregnant women as well as those facing greater difficulty to quality care access are found. Prenatal care cannot prevent major childbirth complications, which are important causes of MM; however, some interventions during the prenatal period can favor maternal prognosis and prevent MM. In this setting, this study brings a scientifically based update concerning effective interventions for maternal mortality prevention during the prenatal period. The most important strategies consist of a tripod with specific interventions related to maternal health promotion, risk prevention and assurance of nutritional support during gestation, in addition to criteria to investigate gestational risk and inclusion of the pregnant woman in the basic component of the prenatal care model. It ends with the definition of priorities in the prevention of MM related to eclampsia/preeclampsia and reinforces the importance of normalization of reference systems for obstetric emergency cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(5):310-315
DOI 10.1590/S0100-72032006000500008
Maternal mortality rate (MM) is a health quality indicator that is directly influenced by the economic, cultural and technological level of a country. Official data of MM in Brazil, although underestimated, point to the lack of quality in pregnancy, childbirth and puerperium care services. This characteristic is common in developing countries, where poorer pregnant women as well as those facing greater difficulty to quality care access are found. Prenatal care cannot prevent major childbirth complications, which are important causes of MM; however, some interventions during the prenatal period can favor maternal prognosis and prevent MM. In this setting, this study brings a scientifically based update concerning effective interventions for maternal mortality prevention during the prenatal period. The most important strategies consist of a tripod with specific interventions related to maternal health promotion, risk prevention and assurance of nutritional support during gestation, in addition to criteria to investigate gestational risk and inclusion of the pregnant woman in the basic component of the prenatal care model. It ends with the definition of priorities in the prevention of MM related to eclampsia/preeclampsia and reinforces the importance of normalization of reference systems for obstetric emergency cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(5):271-277
DOI 10.1590/S0100-72032006000500002
PURPOSE: to evaluate the contraceptive methods adopted by the public health system of Maringá County, Paraná, regarding the orientations for using them, indications, contraindications and reasons for interrupting these methods, as well as the profile of the female users. METHODS: transversal descriptive study, performed through 284 home interviews with women selected from the 62 groups of the Family Health Program, after their free and informed consent, and after the questionnaire had been approved by the Ethics in Research Committee involving human beings of the State University of Maringá (Universidade Estadual de Maringá - UEM). Before applying the questionnaires, they were pretested, focusing on the following sections: characterization of the interviewee, socioeconomical factors and contraceptive methods. Results were analyzed using the Statistical Package for the Social Sciences software 12.0 version. RESULTS: most women were white, married, between 35 and 49 years old, with high school education, working without salary, and from D and E economical classes. Of them, 22.5% were smokers and 4.9% alcohol users. Contraceptive pills were adopted by 50.3% of the women; condom by 28.1% and tubal ligature by 32%, following, in general, the health professional orientation. Reasons for interrupting the contraceptive methods were the wish to get pregnant, preference for a permanent method, and also because of the side effects of the pill. Smoking was the most prevalent risk factor for pill use. Only 35.9% of the interviewed women started using the pill after a previous medical visit, and almost in the same proportion, 33.6%, without visit before starting to use it. CONCLUSIONS: it was observed that the indications of the contraceptive method to be used, and the orientations accomplished by the health professionals were satisfactory, despite the high levels of tubal ligature and the detection of relative contraindications for pill users with more than 5 years of use.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(5):271-277
DOI 10.1590/S0100-72032006000500002
PURPOSE: to evaluate the contraceptive methods adopted by the public health system of Maringá County, Paraná, regarding the orientations for using them, indications, contraindications and reasons for interrupting these methods, as well as the profile of the female users. METHODS: transversal descriptive study, performed through 284 home interviews with women selected from the 62 groups of the Family Health Program, after their free and informed consent, and after the questionnaire had been approved by the Ethics in Research Committee involving human beings of the State University of Maringá (Universidade Estadual de Maringá - UEM). Before applying the questionnaires, they were pretested, focusing on the following sections: characterization of the interviewee, socioeconomical factors and contraceptive methods. Results were analyzed using the Statistical Package for the Social Sciences software 12.0 version. RESULTS: most women were white, married, between 35 and 49 years old, with high school education, working without salary, and from D and E economical classes. Of them, 22.5% were smokers and 4.9% alcohol users. Contraceptive pills were adopted by 50.3% of the women; condom by 28.1% and tubal ligature by 32%, following, in general, the health professional orientation. Reasons for interrupting the contraceptive methods were the wish to get pregnant, preference for a permanent method, and also because of the side effects of the pill. Smoking was the most prevalent risk factor for pill use. Only 35.9% of the interviewed women started using the pill after a previous medical visit, and almost in the same proportion, 33.6%, without visit before starting to use it. CONCLUSIONS: it was observed that the indications of the contraceptive method to be used, and the orientations accomplished by the health professionals were satisfactory, despite the high levels of tubal ligature and the detection of relative contraindications for pill users with more than 5 years of use.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(2):91-100
DOI 10.1590/S0100-72032006000200004
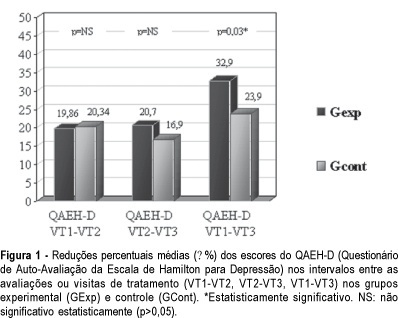
PURPOSE: to evaluate the efficacy of the use of isoflavones in the treatment of depressive symptoms in climacteric women. METHODS: placebo-controlled, randomized double-blind experimental study with 84 climacteric women who were assisted at the Lauro Wanderley University Hospital Ambulatory, in João Pessoa, Paraíba, Brazil. In the evaluation of the depressive symptoms the Self-evaluation questionnare of Hamilton's rating scale for depresion (QAEH-D) was used in the pretreatment visit (VT1), and in the 8th (VT2) and 16th (VT3) week after treatment. The experimental group (GExp) received soy extract with isoflavones, 120 mg per day, and the control group (GCont), placebo. The comparison of the scores of the QAEH-D between the VT1, VT2 and VT3 groups constituted the primary measure of efficacy (t test, p<0.05). Secondary analysis included the estimate of the "domino hypothesis" and the clinical and laboratory evaluation of side effects. RESULTS: there was a significant reduction of the QAEH-D scores in the GExp (VT2
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2006;28(2):91-100
DOI 10.1590/S0100-72032006000200004
PURPOSE: to evaluate the efficacy of the use of isoflavones in the treatment of depressive symptoms in climacteric women. METHODS: placebo-controlled, randomized double-blind experimental study with 84 climacteric women who were assisted at the Lauro Wanderley University Hospital Ambulatory, in João Pessoa, Paraíba, Brazil. In the evaluation of the depressive symptoms the Self-evaluation questionnare of Hamilton's rating scale for depresion (QAEH-D) was used in the pretreatment visit (VT1), and in the 8th (VT2) and 16th (VT3) week after treatment. The experimental group (GExp) received soy extract with isoflavones, 120 mg per day, and the control group (GCont), placebo. The comparison of the scores of the QAEH-D between the VT1, VT2 and VT3 groups constituted the primary measure of efficacy (t test, p<0.05). Secondary analysis included the estimate of the "domino hypothesis" and the clinical and laboratory evaluation of side effects. RESULTS: there was a significant reduction of the QAEH-D scores in the GExp (VT2
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(6):357-365
DOI 10.1590/S0100-72032005000600011
The multiple factors involved in maternal complications and maternal mortality make the task of their long-term control difficult and time-consuming. Professional care for pregnant women and/or those in labor certainly represents a key point for obtaining good outcomes, either maternal or perinatal. From the starting point that an adequate professional medical care for delivery has the capacity of decreasing the occurrence of complications associated with maternal morbidity and mortality, the evidence regarding some interventions included in this care is summarily presented. The evidence derived from studies performed with a strong methodological and scientific approach, mainly randomized controlled trials, on interventions to reduce complications and maternal mortality. These main interventions basically refer to: institutional care to is focused delivery, skilled professional care, use of traditional birth attendants in some contexts, use of appropriate technologies including partograph, place of birth, position for delivery, use of episiotomy, type of delivery, use of oxytocin during the active phase of labor, performance of push efforts during the second stage, active management of the third stage, and prophylaxis for post-partum hemorrhage. Although the effect of avoiding maternal death is difficult to be evaluated due to its low frequency, its rational and standardized use, through manuals and guidelines for intervention care, has a positive effect on the quality of care for childbirth. This is part of the human and technical context of the right that every woman has to the best possible care in this so special moment of her life.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(6):357-365
DOI 10.1590/S0100-72032005000600011
The multiple factors involved in maternal complications and maternal mortality make the task of their long-term control difficult and time-consuming. Professional care for pregnant women and/or those in labor certainly represents a key point for obtaining good outcomes, either maternal or perinatal. From the starting point that an adequate professional medical care for delivery has the capacity of decreasing the occurrence of complications associated with maternal morbidity and mortality, the evidence regarding some interventions included in this care is summarily presented. The evidence derived from studies performed with a strong methodological and scientific approach, mainly randomized controlled trials, on interventions to reduce complications and maternal mortality. These main interventions basically refer to: institutional care to is focused delivery, skilled professional care, use of traditional birth attendants in some contexts, use of appropriate technologies including partograph, place of birth, position for delivery, use of episiotomy, type of delivery, use of oxytocin during the active phase of labor, performance of push efforts during the second stage, active management of the third stage, and prophylaxis for post-partum hemorrhage. Although the effect of avoiding maternal death is difficult to be evaluated due to its low frequency, its rational and standardized use, through manuals and guidelines for intervention care, has a positive effect on the quality of care for childbirth. This is part of the human and technical context of the right that every woman has to the best possible care in this so special moment of her life.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):235-242
DOI 10.1590/S0100-72032005000500002
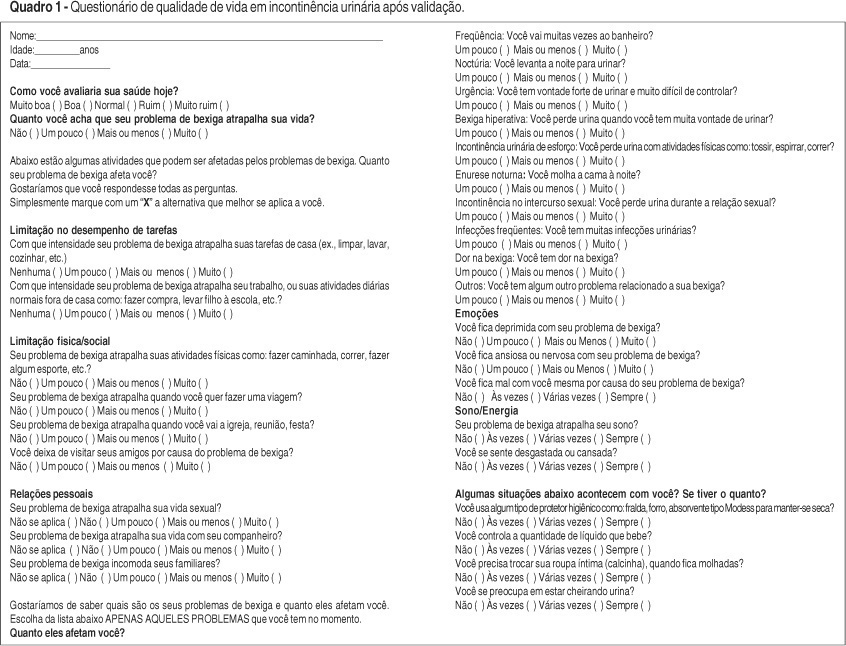
PURPOSE: the proposal of the present study was to translate and to validate King's Health Questionnaire (KHQ) for Brazilian women with urinary incontinence. METHODS: a hundred and thirty-four patients with urinary incontinence, confirmed by urodynamic study, were enrolled from the outpatient clinic of Uroginecology. Initially, we translated the KHQ into the Brazilian Portuguese language in agreement with international criteria. Due to language and cultural differences we performed a cultural, structural, conceptual, and semantic adaptation of the KHQ, in order to make sure that patients were able to fully understand the questions. All patients answered the KHQ twice on the same day, within an interval of 30 min, applied by two different interviewers. After 7 to 14 days, on a second visit, the questionnaire was applied again. Reliability (intra- and interobserver internal consistency), construct and discriminative validity were tested. RESULTS: several cultural adaptations were necessary until we reached the final version. The intra-observer internal consistency (alpha of Cronbach) of the several dimensions varied from moderate to high (0.77-0.90), and the interobserver internal consistency varied from 0.66 to 0.94. Moderate to strong correlation was detected among the specific KHQ urinary incontinence dominions and clinical urinary incontinence manifestations known to affect the quality of life of these patients. CONCLUSION: KHQ was adapted to the Portuguese language and to the Brazilian culture, showing great reliability and validity. It should be included and used in any Brazilian urinary incontinence clinical trial.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(5):235-242
DOI 10.1590/S0100-72032005000500002
PURPOSE: the proposal of the present study was to translate and to validate King's Health Questionnaire (KHQ) for Brazilian women with urinary incontinence. METHODS: a hundred and thirty-four patients with urinary incontinence, confirmed by urodynamic study, were enrolled from the outpatient clinic of Uroginecology. Initially, we translated the KHQ into the Brazilian Portuguese language in agreement with international criteria. Due to language and cultural differences we performed a cultural, structural, conceptual, and semantic adaptation of the KHQ, in order to make sure that patients were able to fully understand the questions. All patients answered the KHQ twice on the same day, within an interval of 30 min, applied by two different interviewers. After 7 to 14 days, on a second visit, the questionnaire was applied again. Reliability (intra- and interobserver internal consistency), construct and discriminative validity were tested. RESULTS: several cultural adaptations were necessary until we reached the final version. The intra-observer internal consistency (alpha of Cronbach) of the several dimensions varied from moderate to high (0.77-0.90), and the interobserver internal consistency varied from 0.66 to 0.94. Moderate to strong correlation was detected among the specific KHQ urinary incontinence dominions and clinical urinary incontinence manifestations known to affect the quality of life of these patients. CONCLUSION: KHQ was adapted to the Portuguese language and to the Brazilian culture, showing great reliability and validity. It should be included and used in any Brazilian urinary incontinence clinical trial.