Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(7):646-653
06-01-2022
This study aims to describe the behavior of chromosomopathy screenings in euploid fetuses.
This is a prospective descriptive study with 566 patients at 11 to 14 weeks of gestation. The associations between ultrasound scans and serological variables were studied. For the quantitative variables we used the Spearman test; for the qualitative with quantitative variables the of Mann-Whitney U-test; and for qualitative variables, the X2 test was applied. Significance was set at p ≤ 0.05.
We have found that gestational age has correlation with ductus venosus, nuchal translucency, free fraction of β subunit of human chorionic gonadotropin, pregnancy-associated plasma protein-A and placental growth factor; there is also a correlation between history of miscarriages and nasal bone. Furthermore, we correlated body mass index with nuchal translucency, free fraction of β subunit of human chorionic gonadotropin, and pregnancy-associated plasma protein-A. Maternal age was associated with free fraction of β subunit of human chorionic gonadotropin and pregnancy-associated plasma protein-A.
Our study demonstrates for the first time the behavior of the biochemical and ultrasonographic markers of chromosomopathy screenings during the first trimester in euploid fetuses in Colombia. Our information is consistent with international reference values. Moreover, we have shown the correlation of different variables with maternal characteristics to determine the variables that could help with development of a screening process during the first trimester with high detection rates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(7):646-653
06-01-2022
This study aims to describe the behavior of chromosomopathy screenings in euploid fetuses.
This is a prospective descriptive study with 566 patients at 11 to 14 weeks of gestation. The associations between ultrasound scans and serological variables were studied. For the quantitative variables we used the Spearman test; for the qualitative with quantitative variables the of Mann-Whitney U-test; and for qualitative variables, the X2 test was applied. Significance was set at p ≤ 0.05.
We have found that gestational age has correlation with ductus venosus, nuchal translucency, free fraction of β subunit of human chorionic gonadotropin, pregnancy-associated plasma protein-A and placental growth factor; there is also a correlation between history of miscarriages and nasal bone. Furthermore, we correlated body mass index with nuchal translucency, free fraction of β subunit of human chorionic gonadotropin, and pregnancy-associated plasma protein-A. Maternal age was associated with free fraction of β subunit of human chorionic gonadotropin and pregnancy-associated plasma protein-A.
Our study demonstrates for the first time the behavior of the biochemical and ultrasonographic markers of chromosomopathy screenings during the first trimester in euploid fetuses in Colombia. Our information is consistent with international reference values. Moreover, we have shown the correlation of different variables with maternal characteristics to determine the variables that could help with development of a screening process during the first trimester with high detection rates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):231-237
02-09-2022
To analyze whether acetylsalicylic (ASA) intake modifies the mean uterine arteries pulsatility index (UtA-PI) at the 2nd or 3rd trimester in a cohort of pregnant women with abnormal mean UtA-PI at between 11 and 14 weeks of gestation.
This is a retrospective cohort study. Singleton pregnancies with abnormal mean UtA-PI at between 11 and 14 weeks of gestation were studied. The participants were divided into 3 groups: 1) If the participant did not take ASA during pregnancy; 2) If the participant took ASA before 14 weeks of gestation; and 3) If the participant took ASA after 14 weeks of gestation. The mean UtA-PI was evaluated at the 2nd and 3rd trimesters, and it was considered to improve when it decreased below the 95th percentile. The prevalence ratio (PR) and the number needed to treat (NNT) werecalculated.
A total of 72 participants with a mean UtA-PI>95th percentile at the 1st trimester of gestation were evaluated. Out of the 18 participants who took ASA, 8 participants started it before 14 weeks of gestation and 10 after. A total of 33.3% of these participants had improved the mean UtA-PI at the 2nd and 3rd trimesters of gestation, although it was not statistically significant (p=0.154). The prevalence ratio was 0.95 (95% confidence interval [CI]: 0.31-1.89), but between the 1st and 2nd trimesters of gestation, the PR was 0.92 (95%CI: 0.21-0.99) and it was statistically significant.
The present work demonstrates a modification of the mean UtA-PI in participants who took ASA compared with those who did not. It is important to check if ASA can modify the normal limits of uterine arteries because this could have an impact on surveillance.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):231-237
02-09-2022
To analyze whether acetylsalicylic (ASA) intake modifies the mean uterine arteries pulsatility index (UtA-PI) at the 2nd or 3rd trimester in a cohort of pregnant women with abnormal mean UtA-PI at between 11 and 14 weeks of gestation.
This is a retrospective cohort study. Singleton pregnancies with abnormal mean UtA-PI at between 11 and 14 weeks of gestation were studied. The participants were divided into 3 groups: 1) If the participant did not take ASA during pregnancy; 2) If the participant took ASA before 14 weeks of gestation; and 3) If the participant took ASA after 14 weeks of gestation. The mean UtA-PI was evaluated at the 2nd and 3rd trimesters, and it was considered to improve when it decreased below the 95th percentile. The prevalence ratio (PR) and the number needed to treat (NNT) werecalculated.
A total of 72 participants with a mean UtA-PI>95th percentile at the 1st trimester of gestation were evaluated. Out of the 18 participants who took ASA, 8 participants started it before 14 weeks of gestation and 10 after. A total of 33.3% of these participants had improved the mean UtA-PI at the 2nd and 3rd trimesters of gestation, although it was not statistically significant (p=0.154). The prevalence ratio was 0.95 (95% confidence interval [CI]: 0.31-1.89), but between the 1st and 2nd trimesters of gestation, the PR was 0.92 (95%CI: 0.21-0.99) and it was statistically significant.
The present work demonstrates a modification of the mean UtA-PI in participants who took ASA compared with those who did not. It is important to check if ASA can modify the normal limits of uterine arteries because this could have an impact on surveillance.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(12):911-918
01-24-2021
Currently, there are up to three different classifications for diagnosing septate uterus. The interobserver agreement among them has been poorly assessed.
A total of 50 three-dimensional (3D) volumes of a nonconsecutive series of women with suspected uterine malformation were used. Two nonexpert examiners evaluated a single 3D volume of the uterus of each woman, blinded to each other. The following measurements were performed: indentation depth, indentation angle, uterine fundal wall thickness, external fundal indentation, and indentation-to-wall-thickness (I:WT) ratio. Each observer had to assign a diagnosis in each case, according to the three classification systems (ESHRE/ESGE, ASRM, and CUME). The interobserver agreement regarding the ESHRE/ESGE, ASRM, and CUME classifications was assessed using the Cohen weighted kappa index (k). Agreement regarding the three classifications (ASRM versus ESHRE/ESGE, ASRM versus CUME, ESHRE/ESGE versus CUME) was also assessed.
The interobserver agreement between the 2 nonexpert examiners was good for the ESHRE/ESGE (k = 0.74; 95% confidence interval [CI]: 0.55–0.92) and very good for the ASRM and CUME classification systems (k = 0.95; 95%CI: 0.86–1.00; and k = 0.91; 95%CI: 0.79–1.00, respectively). Agreement between the ESHRE/ESGE and ASRM classifications was moderate for both examiners. Agreement between the ESHRE/ESGE and CUME classifications was moderate for examiner 1 and good for examiner 2. Agreement between the ASRM and CUME classifications was good for both examiners.
The three classifications have good (ESHRE/ESGE) or very good (ASRM and CUME) interobserver agreement. Agreement between the ASRM and CUME classifications was higher than that for the ESHRE/ESGE and ASRM and ESHRE/ESGE and CUME classifications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(12):911-918
01-24-2021
Currently, there are up to three different classifications for diagnosing septate uterus. The interobserver agreement among them has been poorly assessed.
A total of 50 three-dimensional (3D) volumes of a nonconsecutive series of women with suspected uterine malformation were used. Two nonexpert examiners evaluated a single 3D volume of the uterus of each woman, blinded to each other. The following measurements were performed: indentation depth, indentation angle, uterine fundal wall thickness, external fundal indentation, and indentation-to-wall-thickness (I:WT) ratio. Each observer had to assign a diagnosis in each case, according to the three classification systems (ESHRE/ESGE, ASRM, and CUME). The interobserver agreement regarding the ESHRE/ESGE, ASRM, and CUME classifications was assessed using the Cohen weighted kappa index (k). Agreement regarding the three classifications (ASRM versus ESHRE/ESGE, ASRM versus CUME, ESHRE/ESGE versus CUME) was also assessed.
The interobserver agreement between the 2 nonexpert examiners was good for the ESHRE/ESGE (k = 0.74; 95% confidence interval [CI]: 0.55–0.92) and very good for the ASRM and CUME classification systems (k = 0.95; 95%CI: 0.86–1.00; and k = 0.91; 95%CI: 0.79–1.00, respectively). Agreement between the ESHRE/ESGE and ASRM classifications was moderate for both examiners. Agreement between the ESHRE/ESGE and CUME classifications was moderate for examiner 1 and good for examiner 2. Agreement between the ASRM and CUME classifications was good for both examiners.
The three classifications have good (ESHRE/ESGE) or very good (ASRM and CUME) interobserver agreement. Agreement between the ASRM and CUME classifications was higher than that for the ESHRE/ESGE and ASRM and ESHRE/ESGE and CUME classifications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(7):545-559
10-18-2021
Fetal growth restriction (FGR) occurswhen the fetus does not reach its intrauterine potential for growth and development as a result of compromise in placental function. It is a condition that affects 5 to 10% of pregnancies and is the second most common cause of perinatal morbidity and mortality. Children born with FGR are at risk of impaired neurological and cognitive development and cardiovascular or endocrine diseases in adulthood. The purpose of the present revision is to perform a literature search for evidence on the detection and assessment by ultrasound of brain injury linked to FGR during fetal life. Using a systematic approach and quantitative evaluation as study methodology, we reviewed ultrasound studies of the fetal brain structure of growth-restricted fetuses with objective quality measures. A total of eight studies were identified. High quality studies were identified for measurement of brain volumes; corpus callosum; brain fissure depth measurements, and cavum septi pellucidi width measurement. A low-quality study was available for transverse cerebellar diameter measurement in FGR. Further prospective randomized studies are needed to understand the changes that occur in the brain of fetuseswith restricted growth, as well as their correlation with the changes in cognitive development observed.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(7):545-559
10-18-2021
Fetal growth restriction (FGR) occurswhen the fetus does not reach its intrauterine potential for growth and development as a result of compromise in placental function. It is a condition that affects 5 to 10% of pregnancies and is the second most common cause of perinatal morbidity and mortality. Children born with FGR are at risk of impaired neurological and cognitive development and cardiovascular or endocrine diseases in adulthood. The purpose of the present revision is to perform a literature search for evidence on the detection and assessment by ultrasound of brain injury linked to FGR during fetal life. Using a systematic approach and quantitative evaluation as study methodology, we reviewed ultrasound studies of the fetal brain structure of growth-restricted fetuses with objective quality measures. A total of eight studies were identified. High quality studies were identified for measurement of brain volumes; corpus callosum; brain fissure depth measurements, and cavum septi pellucidi width measurement. A low-quality study was available for transverse cerebellar diameter measurement in FGR. Further prospective randomized studies are needed to understand the changes that occur in the brain of fetuseswith restricted growth, as well as their correlation with the changes in cognitive development observed.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):181-187
05-18-2020
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):181-187
05-18-2020
To evaluate the ability of the pubic arch angle (PAA) as measured by transperineal ultrasonography during labor to predict the delivery type and cephalic pole disengagement mode.
The present prospective cross-sectional study included 221 women in singleton-gestational labor ≥ 37 weeks with cephalic fetuses who underwent PAA measurement using transperineal ultrasonography. These measurements were correlated with the delivery type, cephalic pole disengagement mode, and fetal and maternal characteristics.
Out of the subjects, 153 (69.2%) had spontaneous vaginal delivery, 7 (3.2%) gave birth by forceps, and 61 (27.6%) delivered by cesarean section. For the analysis, deliveries were divided into two groups: vaginal and surgical (forceps and cesarean). The mean PAA was 102 ± 7.5º (range, 79.3-117.7º). No statistically significant difference was observed in delivery type (102.6 ± 7.2º versus 100.8 ± 7.9º, p = 0.105). The occipitoanterior position was seen in 94.1% of the fetuses and the occipitoposterior position in 5.8%. A narrower PAA was found in the group of surgical deliveries (97.9 ± 9.6º versus 102.6 ± 7.3º, p = 0.049). Multivariate regression analysis showed that PAA was a predictive variable for the occurrence of head disengagement in occipital varieties after birth (odds ratio, 0.9; 95% confidence interval, 0.82-0.99; p = 0.026).
Ultrasonographic measurement of the PAA was not a predictor of delivery type, but was associated with the persistence of occipital varieties after birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(9):525-530
09-30-2019
The etiology of embryonic demise is multifactorial, with chromosomal abnormalities being the most common (40%). The purpose of the present study is to evaluate the correlation between a serum biomarker, progesterone, and an ultrasonographic parameter, the distance between yolk sac and embryo (DYSE) in assessing the prognosis of pregnancy outcome in the 1st trimester.
The present study is a prospective case-control analysis that includes 2 groups of patients: 81 patients with first-trimester normal evolutive pregnancy and 89 patients with embryonic demise, all of the patients having between 6 and 11 weeks of amenorrhea. Endovaginal ultrasonographic exploration was performed to evaluate the distance between the lower pole of the embryo and the yolk sac. From each subject enrolled in the study, 20ml of blood was collected for progesterone serum level measurement.
Regarding the DYSE in the case group, lower values were observed compared with the control group, the difference being statistically significant. In the statistical analysis of serum progesterone values, statistically significant differences were observed between the 2 groups (p<0.05).
The DYSE has a high positive predictive value in identifying pregnancies with potentially reserved outcome, with the present study demonstrating that a DYSE<3mm causes an unfavorable evolution of the pregnancy. Low serum levels of progesterone are associated with an increased rate of nonviable embryos. The correlation between these two parameters increases the effectiveness of screening methods in prenatal monitoring and improves the diagnostic methods for the firsttrimester pregnancies whose outcome potential can be reserved.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(9):525-530
09-30-2019
The etiology of embryonic demise is multifactorial, with chromosomal abnormalities being the most common (40%). The purpose of the present study is to evaluate the correlation between a serum biomarker, progesterone, and an ultrasonographic parameter, the distance between yolk sac and embryo (DYSE) in assessing the prognosis of pregnancy outcome in the 1st trimester.
The present study is a prospective case-control analysis that includes 2 groups of patients: 81 patients with first-trimester normal evolutive pregnancy and 89 patients with embryonic demise, all of the patients having between 6 and 11 weeks of amenorrhea. Endovaginal ultrasonographic exploration was performed to evaluate the distance between the lower pole of the embryo and the yolk sac. From each subject enrolled in the study, 20ml of blood was collected for progesterone serum level measurement.
Regarding the DYSE in the case group, lower values were observed compared with the control group, the difference being statistically significant. In the statistical analysis of serum progesterone values, statistically significant differences were observed between the 2 groups (p<0.05).
The DYSE has a high positive predictive value in identifying pregnancies with potentially reserved outcome, with the present study demonstrating that a DYSE<3mm causes an unfavorable evolution of the pregnancy. Low serum levels of progesterone are associated with an increased rate of nonviable embryos. The correlation between these two parameters increases the effectiveness of screening methods in prenatal monitoring and improves the diagnostic methods for the firsttrimester pregnancies whose outcome potential can be reserved.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):596-601
11-01-2017
To investigate the clinical and sonographic parameters associated with adverse fetal outcomes in patients with congenital parvovirus B19 infection managed by intrauterine transfusion.
This was a single-center retrospective study conducted from January 2005 to December 2016 that assessed patients with singleton pregnancies with fetal parvovirus infection confirmed by a polymerase chain reaction of the amniotic fluid or fetal blood samples who underwent at least one intrauterine transfusion. The maternal characteristics, sonographic findings and parameters related to intrauterine transfusion were compared between the two groups (recovery/non-recovery), who were categorized based on fetal response after in-utero transfusions. Progression to fetal death or delivery without fetal recovery after the transfusions was considered nonrecovery and categorized as an adverse outcome.
The final analysis included ten singleton pregnancies: seven of which were categorized into the recovery group and three of which into the non-recovery group. The baseline characteristics were similar between the groups. All fetuses were hydropic at the time of diagnosis. No significant differences related to sonographic or intrauterine transfusion parameters were identified between the groups; however, the nonrecovery group tended to have an increased number of sonographic markers and lower fetal hemoglobin and platelet levels before the transfusion.
We were unable to firmly establish the clinical or sonographic parameters associated with adverse fetal outcomes in patients with parvovirus infection managed with intrauterine transfusions; however, edema, placental thickening and oligohydramnios may indicate greater fetal compromise and, subsequently, adverse outcomes. However, further studies are necessary, mainly due to the small number of cases analyzed in the present study.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(11):596-601
11-01-2017
To investigate the clinical and sonographic parameters associated with adverse fetal outcomes in patients with congenital parvovirus B19 infection managed by intrauterine transfusion.
This was a single-center retrospective study conducted from January 2005 to December 2016 that assessed patients with singleton pregnancies with fetal parvovirus infection confirmed by a polymerase chain reaction of the amniotic fluid or fetal blood samples who underwent at least one intrauterine transfusion. The maternal characteristics, sonographic findings and parameters related to intrauterine transfusion were compared between the two groups (recovery/non-recovery), who were categorized based on fetal response after in-utero transfusions. Progression to fetal death or delivery without fetal recovery after the transfusions was considered nonrecovery and categorized as an adverse outcome.
The final analysis included ten singleton pregnancies: seven of which were categorized into the recovery group and three of which into the non-recovery group. The baseline characteristics were similar between the groups. All fetuses were hydropic at the time of diagnosis. No significant differences related to sonographic or intrauterine transfusion parameters were identified between the groups; however, the nonrecovery group tended to have an increased number of sonographic markers and lower fetal hemoglobin and platelet levels before the transfusion.
We were unable to firmly establish the clinical or sonographic parameters associated with adverse fetal outcomes in patients with parvovirus infection managed with intrauterine transfusions; however, edema, placental thickening and oligohydramnios may indicate greater fetal compromise and, subsequently, adverse outcomes. However, further studies are necessary, mainly due to the small number of cases analyzed in the present study.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(9):471-479
09-01-2017
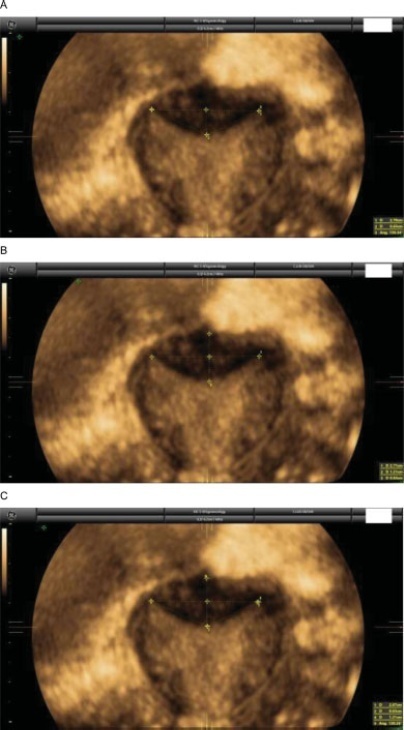
Using three-dimensional ultrasound (3D-US), we aimed to compare the tape position and the angle formed by the sling arms in different techniques of midurethral sling insertion for the surgical treatment of stress urinary incontinence, three years after surgery. In addition, we examined the correlations between the US findings and the clinical late postoperative results.
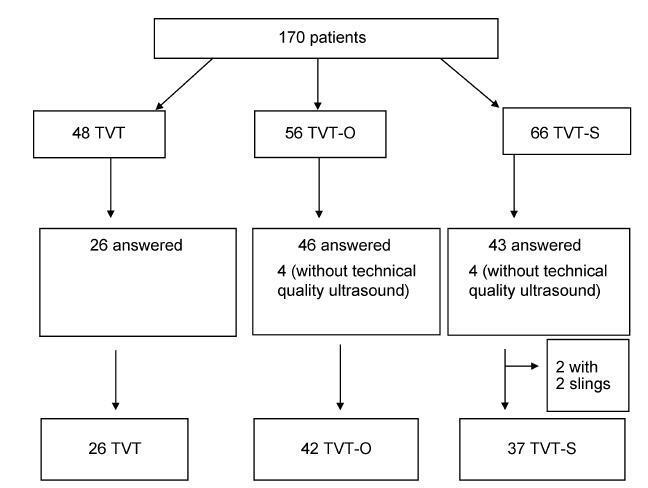
A prospective cross-sectional cohort study of 170 patients who underwent a sling procedure between May 2009 and December 2011 was performed. The final sample, with US images of sufficient quality, included 26 retropubic slings (tension-free vaginal tape, TVT), 42 transobturator slings (tension-free vaginal tape-obturator, TVTO), and 37 single-incision slings (tension-free vaginal tape-Secur, TVT-S). The images (at rest, during the Valsalva maneuver, and during pelvic floor contraction) were analyzed offline by 2 different observers blinded against the surgical and urinary continence status. Group comparisons were performed using the Student t-test, the chi-squared and the Kruskal-Wallis tests, and analyses of variance with Tukey multiple comparisons.
Differences among the groups were found in themean angle of the tape arms (TVT = 119.94°, TVT-O = 141.93°, TVT-S = 121.06°; p < 0.001) and in the distance between the bladder neck and the tape at rest (TVT = 1.65 cm, TVT-O = 1.93 cm, TVTS = 1.95 cm; p = 0.010). The global objective cure rate was of 87.8% (TVT = 88.5%, TVT-O = 90.5%, TVT-S = 83.8%; p = 0.701). The overall subjective cure rate was of 83.8% (TVT = 88.5%, TVT-O = 88.5% and TVT-S = 78.4%; p = 0.514). The slings were located in the mid-urethra in 85.7% of the patients (TVT = 100%, TVT-O = 73.8%, TVTS = 89.2%; p = 0.001), with a more distal location associated with obesity (distal: 66.7% obese; mid-urethra: 34% obese; p = 0.003). Urgency-related symptoms were observed in 23.8% of the patients (TVT = 30.8%, TVT-O = 21.4%, TVT-S = 21.6%; p = 0.630).
The angle formed by the arms of the sling tape was more obtuse for the transobturator slings compared with the angles for the retropubic or single-incision slings. Retropubic slings were more frequently located in the mid-urethra compared with the other slings, regardless of obesity. However, the analyzed sonographic measures did not correlate with the urinary symptoms three years after the surgery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(9):471-479
09-01-2017
Using three-dimensional ultrasound (3D-US), we aimed to compare the tape position and the angle formed by the sling arms in different techniques of midurethral sling insertion for the surgical treatment of stress urinary incontinence, three years after surgery. In addition, we examined the correlations between the US findings and the clinical late postoperative results.
A prospective cross-sectional cohort study of 170 patients who underwent a sling procedure between May 2009 and December 2011 was performed. The final sample, with US images of sufficient quality, included 26 retropubic slings (tension-free vaginal tape, TVT), 42 transobturator slings (tension-free vaginal tape-obturator, TVTO), and 37 single-incision slings (tension-free vaginal tape-Secur, TVT-S). The images (at rest, during the Valsalva maneuver, and during pelvic floor contraction) were analyzed offline by 2 different observers blinded against the surgical and urinary continence status. Group comparisons were performed using the Student t-test, the chi-squared and the Kruskal-Wallis tests, and analyses of variance with Tukey multiple comparisons.
Differences among the groups were found in themean angle of the tape arms (TVT = 119.94°, TVT-O = 141.93°, TVT-S = 121.06°; p < 0.001) and in the distance between the bladder neck and the tape at rest (TVT = 1.65 cm, TVT-O = 1.93 cm, TVTS = 1.95 cm; p = 0.010). The global objective cure rate was of 87.8% (TVT = 88.5%, TVT-O = 90.5%, TVT-S = 83.8%; p = 0.701). The overall subjective cure rate was of 83.8% (TVT = 88.5%, TVT-O = 88.5% and TVT-S = 78.4%; p = 0.514). The slings were located in the mid-urethra in 85.7% of the patients (TVT = 100%, TVT-O = 73.8%, TVTS = 89.2%; p = 0.001), with a more distal location associated with obesity (distal: 66.7% obese; mid-urethra: 34% obese; p = 0.003). Urgency-related symptoms were observed in 23.8% of the patients (TVT = 30.8%, TVT-O = 21.4%, TVT-S = 21.6%; p = 0.630).
The angle formed by the arms of the sling tape was more obtuse for the transobturator slings compared with the angles for the retropubic or single-incision slings. Retropubic slings were more frequently located in the mid-urethra compared with the other slings, regardless of obesity. However, the analyzed sonographic measures did not correlate with the urinary symptoms three years after the surgery.