You searched for:"Rosiane Mattar"
We found (43) results for your search.Summary
Rev Bras Ginecol Obstet. 2011;33(5):219-224
DOI 10.1590/S0100-72032011000500003
To compare the sexual function of healthy adult pregnant women with that of gestational diabetes patients (GDM) in the third trimester. METHODS: This cross-sectional study enrolled two groups of women managed antenatal care clinics. Inclusion criteria were: maternal age .20 years, gestational age at least 28 weeks, being in a heterosexual relationship with the same partner for at least 6 months, and being able to read. We excluded women with a medical recommendation for sexual abstinence due to clinical or obstetric disorders; hypertension controlled through medications; pregnancy resulting from rape; absent or sexually unavailable partner in the last month; hospital admission in the last month; use of vaginal creams in the last 30 days; multiple pregnancy, regular use of alcohol or illicit drugs or use of medications that can interfere with sexual function. Eighty-seven patients fulfilled the selection criteria and were included in the study. The Sexual Quotient . Feminine Version (QS-F) questionnaire was used to assess sexual function. Student's t and X² tests were used to compare differences between groups and p<0.05 was considered significant. RESULTS: The mean gestational age of the participants was 34 weeks. There were no significant differences in the mean QS-F scores between groups (62.5 healthy vs 62.8 GDM women, p=0.9). Approximately half the participants (47 and 47.5% of the healthy and GDM women, respectively, p=0.9) had total scores up to 60, indicative of dysfunction in one of the assessed domains (desire, sexual satisfaction, arousal, orgasm, dyspareunia and vaginismus). CONCLUSIONS: The prevalence of sexual dysfunction was high among women in the third trimester of pregnancy and did not differ significantly between healthy women and women with GDM.
Summary
Rev Bras Ginecol Obstet. 2011;33(5):219-224
DOI 10.1590/S0100-72032011000500003
To compare the sexual function of healthy adult pregnant women with that of gestational diabetes patients (GDM) in the third trimester. METHODS: This cross-sectional study enrolled two groups of women managed antenatal care clinics. Inclusion criteria were: maternal age .20 years, gestational age at least 28 weeks, being in a heterosexual relationship with the same partner for at least 6 months, and being able to read. We excluded women with a medical recommendation for sexual abstinence due to clinical or obstetric disorders; hypertension controlled through medications; pregnancy resulting from rape; absent or sexually unavailable partner in the last month; hospital admission in the last month; use of vaginal creams in the last 30 days; multiple pregnancy, regular use of alcohol or illicit drugs or use of medications that can interfere with sexual function. Eighty-seven patients fulfilled the selection criteria and were included in the study. The Sexual Quotient . Feminine Version (QS-F) questionnaire was used to assess sexual function. Student's t and X² tests were used to compare differences between groups and p<0.05 was considered significant. RESULTS: The mean gestational age of the participants was 34 weeks. There were no significant differences in the mean QS-F scores between groups (62.5 healthy vs 62.8 GDM women, p=0.9). Approximately half the participants (47 and 47.5% of the healthy and GDM women, respectively, p=0.9) had total scores up to 60, indicative of dysfunction in one of the assessed domains (desire, sexual satisfaction, arousal, orgasm, dyspareunia and vaginismus). CONCLUSIONS: The prevalence of sexual dysfunction was high among women in the third trimester of pregnancy and did not differ significantly between healthy women and women with GDM.
Summary
Rev Bras Ginecol Obstet. 2010;32(5):229-233
DOI 10.1590/S0100-72032010000500005
PURPOSE: to assess a possible association between polymorphism of the progesterone receptor gene (PROGINS) and recurrent spontaneous abortion (RSA). METHODS: in this case-control study, 85 women with at least three previous spontaneous abortions without an identifiable cause (RSA Group) and 157 women with at least two previous term pregnancies without pathologies and no previous miscarriage (Control Group) were selected. An amount of 10 mL of peripheral blood was collected by venipuncture and genomic DNA was extracted by the DTAB/CTAB method, followed by the polymerase chain reaction (PCR) under specific conditions for this polymorphism and by amplification by 2% agarose gel electrophoresis. The bands were visualized with an ultraviolet light transilluminator and the gels were photographed. Differences in the PROGINS genotype and allele frequencies between groups were analyzed by the χ2 test, with the level of significance set at p<0.05. The Odds Ratio (OR) was also used, with 95% confidence intervals 95%CI. RESULTS: PROGINS genotypic frequencies were 72.3% T1T1 and 27.7% T1T2 for the RSA group and 764% T1T1, 22.3% T1T2 and 1.3% T2T2 for the control group. There were no differecnes between groups when the genotype and allele frequencies were analyzed: respectively p=0.48 (OR: 0.8) and p=0.65 (OR: 0.9). CONCLUSIONS: our results suggest that PROGINS polymorphism is not associated with RSA.
Summary
Rev Bras Ginecol Obstet. 2010;32(5):229-233
DOI 10.1590/S0100-72032010000500005
PURPOSE: to assess a possible association between polymorphism of the progesterone receptor gene (PROGINS) and recurrent spontaneous abortion (RSA). METHODS: in this case-control study, 85 women with at least three previous spontaneous abortions without an identifiable cause (RSA Group) and 157 women with at least two previous term pregnancies without pathologies and no previous miscarriage (Control Group) were selected. An amount of 10 mL of peripheral blood was collected by venipuncture and genomic DNA was extracted by the DTAB/CTAB method, followed by the polymerase chain reaction (PCR) under specific conditions for this polymorphism and by amplification by 2% agarose gel electrophoresis. The bands were visualized with an ultraviolet light transilluminator and the gels were photographed. Differences in the PROGINS genotype and allele frequencies between groups were analyzed by the χ2 test, with the level of significance set at p<0.05. The Odds Ratio (OR) was also used, with 95% confidence intervals 95%CI. RESULTS: PROGINS genotypic frequencies were 72.3% T1T1 and 27.7% T1T2 for the RSA group and 764% T1T1, 22.3% T1T2 and 1.3% T2T2 for the control group. There were no differecnes between groups when the genotype and allele frequencies were analyzed: respectively p=0.48 (OR: 0.8) and p=0.65 (OR: 0.9). CONCLUSIONS: our results suggest that PROGINS polymorphism is not associated with RSA.
Summary
Rev Bras Ginecol Obstet. 2017;39(5):235-248
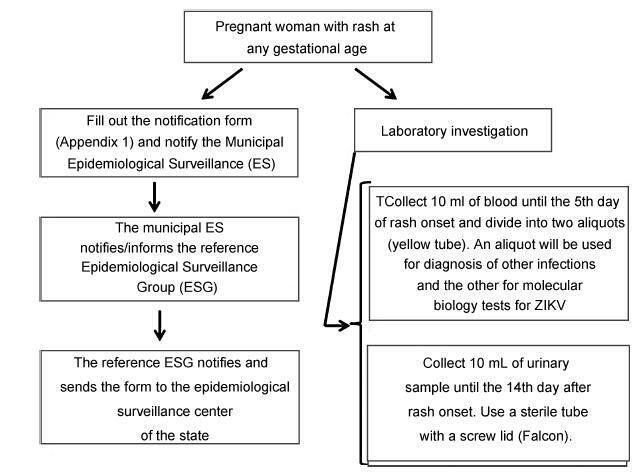
From the discovery of the Zika virus (ZIKV) in 1947 in Uganda (Africa), until its arrival in South America, it was not known that it would affect human reproductive life so severely. Today, damagetothe central nervous system is known to be multiple, and microcephaly is considered the tip of the iceberg. Microcephaly actually represents the epilogue of this infection’s devastating process on the central nervous system of embryos and fetuses. As a result of central nervous system aggression by the ZIKV, this infection brings the possibility of arthrogryposis, dysphagia, deafness and visual impairment. All of these changes of varying severity directly or indirectly compromise the future life of these children, and are already considered a congenital syndrome linked to the ZIKV. Diagnosis is one of the main difficulties in the approach of this infection. Considering the clinical part, it has manifestations common to infections by the dengue virus and the chikungunya fever, varying only in subjective intensities. The most frequent clinical variables are rash, febrile state, non-purulent conjunctivitis and arthralgia, among others. In terms of laboratory resources, there are also limitations to the subsidiary diagnosis. Molecular biology tests are based on polymerase chain reaction (PCR)with reverse transcriptase (RT) action, since the ZIKV is a ribonucleic acid (RNA) virus. The RT-PCR shows serum or plasma positivity for a short period of time, no more than five days after the onset of the signs and symptoms. The ZIKVurine test is positive for a longer period, up to 14 days. There are still no reliable techniques for the serological diagnosis of this infection. If there are no complications (meningoencephalitis or Guillain-Barré syndrome), further examination is unnecessary to assess systemic impairment. However, evidence is needed to rule out other infections that also cause rashes, such as dengue, chikungunya, syphilis, toxoplasmosis, cytomegalovirus, rubella, and herpes. There is no specific antiviral therapy against ZIKV, and the therapeutic approach to infected pregnant women is limited to the use of antipyretics and analgesics. Anti-inflammatory drugs should be avoided until the diagnosis of dengue is discarded. There is no need to modify the schedule of prenatal visits for pregnant women infected by ZIKV, but it is necessary to guarantee three ultrasound examinations during pregnancy for low-risk pregnancies, and monthly for pregnant women with confirmed ZIKV infection. Vaginal delivery and natural breastfeeding are advised.
Summary
Rev Bras Ginecol Obstet. 2017;39(5):235-248
From the discovery of the Zika virus (ZIKV) in 1947 in Uganda (Africa), until its arrival in South America, it was not known that it would affect human reproductive life so severely. Today, damagetothe central nervous system is known to be multiple, and microcephaly is considered the tip of the iceberg. Microcephaly actually represents the epilogue of this infection’s devastating process on the central nervous system of embryos and fetuses. As a result of central nervous system aggression by the ZIKV, this infection brings the possibility of arthrogryposis, dysphagia, deafness and visual impairment. All of these changes of varying severity directly or indirectly compromise the future life of these children, and are already considered a congenital syndrome linked to the ZIKV. Diagnosis is one of the main difficulties in the approach of this infection. Considering the clinical part, it has manifestations common to infections by the dengue virus and the chikungunya fever, varying only in subjective intensities. The most frequent clinical variables are rash, febrile state, non-purulent conjunctivitis and arthralgia, among others. In terms of laboratory resources, there are also limitations to the subsidiary diagnosis. Molecular biology tests are based on polymerase chain reaction (PCR)with reverse transcriptase (RT) action, since the ZIKV is a ribonucleic acid (RNA) virus. The RT-PCR shows serum or plasma positivity for a short period of time, no more than five days after the onset of the signs and symptoms. The ZIKVurine test is positive for a longer period, up to 14 days. There are still no reliable techniques for the serological diagnosis of this infection. If there are no complications (meningoencephalitis or Guillain-Barré syndrome), further examination is unnecessary to assess systemic impairment. However, evidence is needed to rule out other infections that also cause rashes, such as dengue, chikungunya, syphilis, toxoplasmosis, cytomegalovirus, rubella, and herpes. There is no specific antiviral therapy against ZIKV, and the therapeutic approach to infected pregnant women is limited to the use of antipyretics and analgesics. Anti-inflammatory drugs should be avoided until the diagnosis of dengue is discarded. There is no need to modify the schedule of prenatal visits for pregnant women infected by ZIKV, but it is necessary to guarantee three ultrasound examinations during pregnancy for low-risk pregnancies, and monthly for pregnant women with confirmed ZIKV infection. Vaginal delivery and natural breastfeeding are advised.
Summary
Rev Bras Ginecol Obstet. 2007;29(5):267-275
DOI 10.1590/S0100-72032007000500008
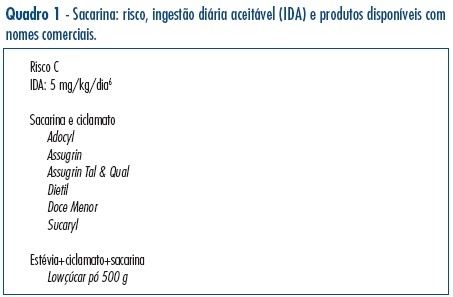
Sweeteners are frequently used by women of reproductive age. This is a narrative review about the sweeteners currently sold in the Brazilian commerce. There is a few information on the use of saccharin and cyclamates in pregnancy and their effects on the fetus. Due to the limited information available and their carcinogenic potential in animal species, saccharin and cyclamates should be avoided during pregnancy (risk C). Aspartame has been extensively studied in animals and it is considered safe for use during pregnancy (risk B), except by women homozygous for phenylketonuria (risk C). Sucralose and acessulfame-K are not toxic, carcinogenic or mutagenic in animals, but there are no controlled studies in humans. However, since these two sweeteners are not metabolized, it is unlikely that their use during pregnancy could be harmful (risk B). Stevia, a substance extracted from a native Brazilian plant, is innocuous in animal pregnancies, but there are no controlled studies in humans (risk B). Body agents found in the composition of artificial sweeteners (mannitol, sorbitol, xylitol, erithrol, lactilol, isomalt, maltilol, lactose, fructose, maltodextrin, dextrin, and inverted sugar) are substances generally regarded as safe for human consumption. In conclusion, according to the currently available evidence, aspartame, sucralose, acessulfame-K and stevia can be safely used during pregnancy.
Summary
Rev Bras Ginecol Obstet. 2007;29(5):267-275
DOI 10.1590/S0100-72032007000500008
Sweeteners are frequently used by women of reproductive age. This is a narrative review about the sweeteners currently sold in the Brazilian commerce. There is a few information on the use of saccharin and cyclamates in pregnancy and their effects on the fetus. Due to the limited information available and their carcinogenic potential in animal species, saccharin and cyclamates should be avoided during pregnancy (risk C). Aspartame has been extensively studied in animals and it is considered safe for use during pregnancy (risk B), except by women homozygous for phenylketonuria (risk C). Sucralose and acessulfame-K are not toxic, carcinogenic or mutagenic in animals, but there are no controlled studies in humans. However, since these two sweeteners are not metabolized, it is unlikely that their use during pregnancy could be harmful (risk B). Stevia, a substance extracted from a native Brazilian plant, is innocuous in animal pregnancies, but there are no controlled studies in humans (risk B). Body agents found in the composition of artificial sweeteners (mannitol, sorbitol, xylitol, erithrol, lactilol, isomalt, maltilol, lactose, fructose, maltodextrin, dextrin, and inverted sugar) are substances generally regarded as safe for human consumption. In conclusion, according to the currently available evidence, aspartame, sucralose, acessulfame-K and stevia can be safely used during pregnancy.
Summary
Rev Bras Ginecol Obstet. 2003;25(1):29-34
DOI 10.1590/S0100-72032003000100005
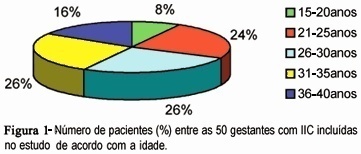
PURPOSE: to identify characteristics common to women who suffer from cervical incompetence (CI) allowing their early identification and helping in the follow-up of the gestational-postdelivery cycle. PATIENTS AND METHODS: fifty pregnant women suffering from CI and submitted to uterine cerclage according to modified McDonald's technique were analyzed in an observational descriptive study. The following variables of the medical records were evaluated: age, preceding obstetrical aspects, time of CI diagnosis, cerclage-related aspects and preterm delivery incidence. RESULTS: the average age of the mothers was 29.28 years and mean number of previous gestations was 3.76. As to the preceding obstetrical aspects, 189 gestations with a CI diagnosis were reported and cerclage had been applied to 18 of them, resulting in 18 babies who were born alive (8 preterm deliveries and 10 term deliveries). Of the 171 previous pregnancies in which CI diagnosis was not reported, 90 progressed to abortion, 68 were preterm and 13 were term deliveries. In 30 (60%) patients, CI was diagnosed during the intergestational interval, and 20 (40%) during gestation. The average gestational period in which patients were submitted to cerclage was 18.29 weeks; 40% of the cerclages were emergency procedures and 60% were elective. The incidence of prematurity was 30% (15/50). CONCLUSION: careful obstetrical evaluation of multiparous women, presenting recurrent miscarriages, during the intergestational interval and/or during the first trimester of pregnancy, may allow the early diagnosis and adequate treatment of CI, avoiding prematurity.
Summary
Rev Bras Ginecol Obstet. 2003;25(1):29-34
DOI 10.1590/S0100-72032003000100005
PURPOSE: to identify characteristics common to women who suffer from cervical incompetence (CI) allowing their early identification and helping in the follow-up of the gestational-postdelivery cycle. PATIENTS AND METHODS: fifty pregnant women suffering from CI and submitted to uterine cerclage according to modified McDonald's technique were analyzed in an observational descriptive study. The following variables of the medical records were evaluated: age, preceding obstetrical aspects, time of CI diagnosis, cerclage-related aspects and preterm delivery incidence. RESULTS: the average age of the mothers was 29.28 years and mean number of previous gestations was 3.76. As to the preceding obstetrical aspects, 189 gestations with a CI diagnosis were reported and cerclage had been applied to 18 of them, resulting in 18 babies who were born alive (8 preterm deliveries and 10 term deliveries). Of the 171 previous pregnancies in which CI diagnosis was not reported, 90 progressed to abortion, 68 were preterm and 13 were term deliveries. In 30 (60%) patients, CI was diagnosed during the intergestational interval, and 20 (40%) during gestation. The average gestational period in which patients were submitted to cerclage was 18.29 weeks; 40% of the cerclages were emergency procedures and 60% were elective. The incidence of prematurity was 30% (15/50). CONCLUSION: careful obstetrical evaluation of multiparous women, presenting recurrent miscarriages, during the intergestational interval and/or during the first trimester of pregnancy, may allow the early diagnosis and adequate treatment of CI, avoiding prematurity.
Summary
Rev Bras Ginecol Obstet. 2021;43(4):323-328
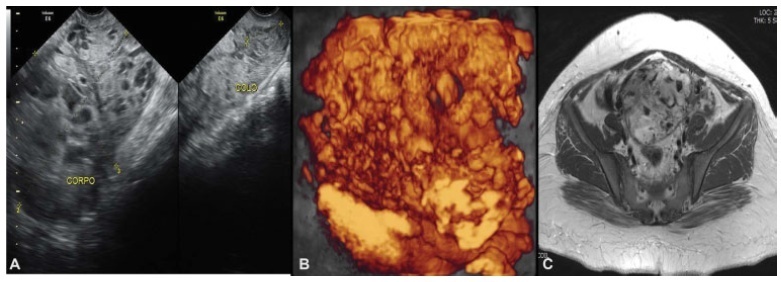
Complete hydatidiform mole (CHM) is a rare type of pregnancy, in which 15 to 20% of the cases may develop into gestational trophoblastic neoplasia (GTN). The diagnostic of GTN must be done as early as possible through weekly surveillance of serum hCG after uterine evacuation.We report the case of 23-year-old primigravida, with CHM but without surveillance of hCG after uterine evacuation. Two months later, the patient presented to the emergency with vaginal bleeding and was referred to the Centro de Doenças Trofoblásticas do Hospital São Paulo. She was diagnosed with high risk GTN stage/score III:7 as per The International Federation of Gynecology and Obstetrics/World Health Organization (FIGO/WHO). The sonographic examination revealed enlarged uterus with a heterogeneous mass constituted of multiple large vessels invading and causing disarrangement of the myometrium. The patient evolved with progressive worsening of vaginal bleeding after chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine (EMA-CO) regimen. She underwent blood transfusion and embolization of uterine arteries due to severe vaginal hemorrhage episodes, with complete control of bleeding. The hCG reached a negative value after the third cycle, and there was a complete regression of the anomalous vascularization of the uterus as well as full recovery of the uterine anatomy. The treatment in a reference center was essential for the appropriate management, especially regarding the uterine arteries embolization trough percutaneous femoral
Summary
Rev Bras Ginecol Obstet. 2021;43(4):323-328
Complete hydatidiform mole (CHM) is a rare type of pregnancy, in which 15 to 20% of the cases may develop into gestational trophoblastic neoplasia (GTN). The diagnostic of GTN must be done as early as possible through weekly surveillance of serum hCG after uterine evacuation.We report the case of 23-year-old primigravida, with CHM but without surveillance of hCG after uterine evacuation. Two months later, the patient presented to the emergency with vaginal bleeding and was referred to the Centro de Doenças Trofoblásticas do Hospital São Paulo. She was diagnosed with high risk GTN stage/score III:7 as per The International Federation of Gynecology and Obstetrics/World Health Organization (FIGO/WHO). The sonographic examination revealed enlarged uterus with a heterogeneous mass constituted of multiple large vessels invading and causing disarrangement of the myometrium. The patient evolved with progressive worsening of vaginal bleeding after chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine (EMA-CO) regimen. She underwent blood transfusion and embolization of uterine arteries due to severe vaginal hemorrhage episodes, with complete control of bleeding. The hCG reached a negative value after the third cycle, and there was a complete regression of the anomalous vascularization of the uterus as well as full recovery of the uterine anatomy. The treatment in a reference center was essential for the appropriate management, especially regarding the uterine arteries embolization trough percutaneous femoral
Summary
Rev Bras Ginecol Obstet. 2003;25(5):331-335
DOI 10.1590/S0100-72032003000500005
PURPOSE: to evaluate whether there is an association between recurrent spontaneous abortion and atopy. METHODS: this was a case-control study with 230 women: 71 with a history of recurrent spontaneous abortion (group A) and 159 with a history of successful pregnancy (group B). The evaluation included a questionnaire in order to investigate the personal history of atopy, considering symptoms of atopic dermatitis, urticaria, rhinitis, asthma, conjunctivitis and gastric or intestinal symptoms. The presence of specific IgE in response to a pool of inhalants, Phadiatop, detected by an enzymatic fluorescence reaction in blood was also investigated. The data were analyzed by Fisher's exact test and a p value < 0.05 was set as level of significance. RESULTS: a positive history of atopy was observed in 57.7% of group A patients and in 55.3% of group B patients. The incidence of positive IgE against Phadiatop was 38% and 33.9% in groups A and B, respectively. Association of allergy disease with positive Phadiatop (presence of specific IgE) was detected in 28.2% of group A and in 22% of group B patients. There was no significant difference between the groups. CONCLUSIONS: we did not observe any association between recurrent spontaneous abortion and atopy.
Summary
Rev Bras Ginecol Obstet. 2003;25(5):331-335
DOI 10.1590/S0100-72032003000500005
PURPOSE: to evaluate whether there is an association between recurrent spontaneous abortion and atopy. METHODS: this was a case-control study with 230 women: 71 with a history of recurrent spontaneous abortion (group A) and 159 with a history of successful pregnancy (group B). The evaluation included a questionnaire in order to investigate the personal history of atopy, considering symptoms of atopic dermatitis, urticaria, rhinitis, asthma, conjunctivitis and gastric or intestinal symptoms. The presence of specific IgE in response to a pool of inhalants, Phadiatop, detected by an enzymatic fluorescence reaction in blood was also investigated. The data were analyzed by Fisher's exact test and a p value < 0.05 was set as level of significance. RESULTS: a positive history of atopy was observed in 57.7% of group A patients and in 55.3% of group B patients. The incidence of positive IgE against Phadiatop was 38% and 33.9% in groups A and B, respectively. Association of allergy disease with positive Phadiatop (presence of specific IgE) was detected in 28.2% of group A and in 22% of group B patients. There was no significant difference between the groups. CONCLUSIONS: we did not observe any association between recurrent spontaneous abortion and atopy.
Summary
Rev Bras Ginecol Obstet. 1999;21(6):341-345
DOI 10.1590/S0100-72031999000600007
Objectives: to analyze the medical and legal aspects in order to contribute to the study and standardization of this obstetrical surgery in Brazil. Methods: our study was based on 11 cases of cesarean section performed in the imminence of maternal death or just after death. These cases were attended at UNIFESP - EPM from 1988 to 1998. Results: there were 7 live births, five of them with a gestational age over 26 weeks. Most deaths occurred within the first 48 hours after admission. The predominant age range was the third decade. Conclusions: although postmortem cesarean section is indicated to save the fetus, it is rarely performed. The conditions for its indication involve knowledge of the technique as well as of the ethical and legal principles.
Summary
Rev Bras Ginecol Obstet. 1999;21(6):341-345
DOI 10.1590/S0100-72031999000600007
Objectives: to analyze the medical and legal aspects in order to contribute to the study and standardization of this obstetrical surgery in Brazil. Methods: our study was based on 11 cases of cesarean section performed in the imminence of maternal death or just after death. These cases were attended at UNIFESP - EPM from 1988 to 1998. Results: there were 7 live births, five of them with a gestational age over 26 weeks. Most deaths occurred within the first 48 hours after admission. The predominant age range was the third decade. Conclusions: although postmortem cesarean section is indicated to save the fetus, it is rarely performed. The conditions for its indication involve knowledge of the technique as well as of the ethical and legal principles.