Summary
Summary
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(10):511-518
DOI 10.1590/S0100-72032007001000004
PURPOSE: to analyze the association between maternal pre-gestational nutritional status and maternal outcomes - hypertensive disorders of pregnancy, gestational diabetes, vitamin A deficiency, and anemia - and the newborn outcome - low birth weight. METHODS: cross-sectional study, with 433 adult puerperal women (> 20 years old) and their newborns, attending the Maternidade Escola of Universidade Federal do Rio de Janeiro (UFRJ). Data was collected through interviews and access to their medical records. Maternal pre-gestational nutritional status was established through pre-gestational body mass index according to the cut-offs for adult women defined by the World Health Organization (WHO), in 1995. The association between gestational outcomes and pre-gestational nutritional status was estimated through odds ratio (OR) and a 95% confidence interval (95%CI). RESULTS: frequency of pre-gestational weight deviation (low weight, overweight and obesity) was 31.6%. Considering the pre-gestational nutritional status, overweight and obese women presented a lower weight gain than eutrophic and low-weight women (p<0.05). Women with pre-gestational obesity presented a higher risk of developing hypertensive disordens of pregnancy (OR=6.3; 95%CI=1.9-20.5) and those with low pre-gestational weight were more likely to give birth to low birth weigh infants (OR=7.1; 95%CI=1.9-27.5). There was no evidence of the association between pre-gestational nutritional status and the development of anemia, vitamin A deficiency and gestational diabetes. The mean weight gain among overweight and obese pregnant women was significantly lower when compared to eutrophic and low-weight pregnant women (p=0.002, p=0.049, p=0.002, p=0.009). CONCLUSIONS: the high number of women with pre-gestational weight deviation reinforces the importance of a nutritional guidance that favors a good nutritional state and reduces the risks of maternal and newborn adverse outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(10):511-518
DOI 10.1590/S0100-72032007001000004
PURPOSE: to analyze the association between maternal pre-gestational nutritional status and maternal outcomes - hypertensive disorders of pregnancy, gestational diabetes, vitamin A deficiency, and anemia - and the newborn outcome - low birth weight. METHODS: cross-sectional study, with 433 adult puerperal women (> 20 years old) and their newborns, attending the Maternidade Escola of Universidade Federal do Rio de Janeiro (UFRJ). Data was collected through interviews and access to their medical records. Maternal pre-gestational nutritional status was established through pre-gestational body mass index according to the cut-offs for adult women defined by the World Health Organization (WHO), in 1995. The association between gestational outcomes and pre-gestational nutritional status was estimated through odds ratio (OR) and a 95% confidence interval (95%CI). RESULTS: frequency of pre-gestational weight deviation (low weight, overweight and obesity) was 31.6%. Considering the pre-gestational nutritional status, overweight and obese women presented a lower weight gain than eutrophic and low-weight women (p<0.05). Women with pre-gestational obesity presented a higher risk of developing hypertensive disordens of pregnancy (OR=6.3; 95%CI=1.9-20.5) and those with low pre-gestational weight were more likely to give birth to low birth weigh infants (OR=7.1; 95%CI=1.9-27.5). There was no evidence of the association between pre-gestational nutritional status and the development of anemia, vitamin A deficiency and gestational diabetes. The mean weight gain among overweight and obese pregnant women was significantly lower when compared to eutrophic and low-weight pregnant women (p=0.002, p=0.049, p=0.002, p=0.009). CONCLUSIONS: the high number of women with pre-gestational weight deviation reinforces the importance of a nutritional guidance that favors a good nutritional state and reduces the risks of maternal and newborn adverse outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(8):511-518
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(8):511-518
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(8):511-517
DOI 10.1590/S0100-72032000000800007
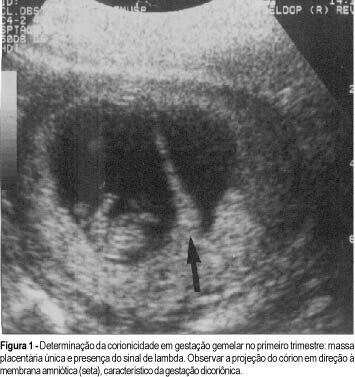
Purpose: to demonstrate the types of fetal malformations in multiple pregnancy and their relation to chorionicity. Methods: one hundred and sixty-nine multiple pregnancies were evaluated. In all cases prenatal ultrasound examination was performed during antenatal care. Chorionicity was defined by: first trimester ultrasound evaluation (absence of lambda sign); presence of two separate placentas; different fetal sex; pathological placental examination. Results: twenty-four (14.2%) fetal malformations were observed, 22 in twin and 2 in triplet pregnancy. In the group with fetal malformations 13 were monochorionic, 4 dichorionic and in 5 the chorionicity was unknown. Some malformations were unique to twins (conjoined twins n = 5, acardiac twin n = 3) and others were nonunique to twins. The gestational age at delivery was lower in the group with fetal malformations compared to the group without fetal malformations. Conclusion: the majority of malformations occurred in the monochorionic pregnancies. In multiple pregnancies early determination of chorionicity is helpful to establish the prognosis and to plan the management of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(8):511-517
DOI 10.1590/S0100-72032000000800007
Purpose: to demonstrate the types of fetal malformations in multiple pregnancy and their relation to chorionicity. Methods: one hundred and sixty-nine multiple pregnancies were evaluated. In all cases prenatal ultrasound examination was performed during antenatal care. Chorionicity was defined by: first trimester ultrasound evaluation (absence of lambda sign); presence of two separate placentas; different fetal sex; pathological placental examination. Results: twenty-four (14.2%) fetal malformations were observed, 22 in twin and 2 in triplet pregnancy. In the group with fetal malformations 13 were monochorionic, 4 dichorionic and in 5 the chorionicity was unknown. Some malformations were unique to twins (conjoined twins n = 5, acardiac twin n = 3) and others were nonunique to twins. The gestational age at delivery was lower in the group with fetal malformations compared to the group without fetal malformations. Conclusion: the majority of malformations occurred in the monochorionic pregnancies. In multiple pregnancies early determination of chorionicity is helpful to establish the prognosis and to plan the management of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(9):511-516
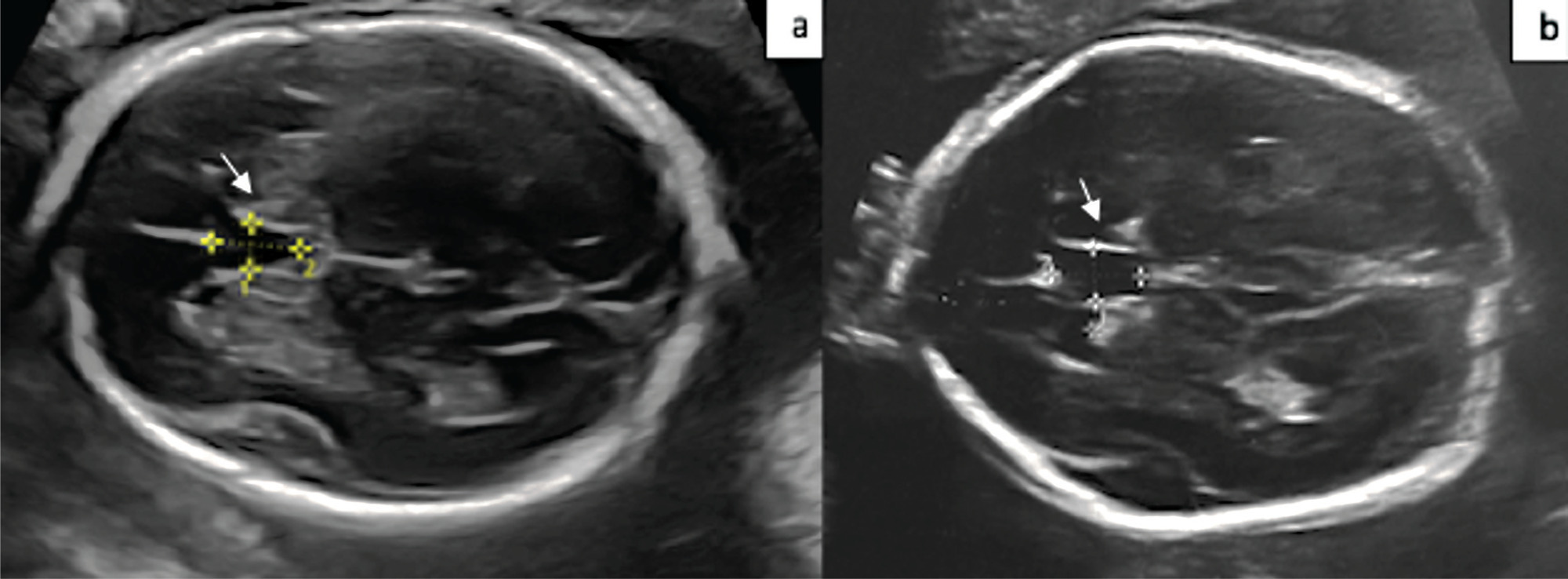
The aim of the present study is to compare the cavum septum pellucidi (CSP) z-score in euploid and aneuploid fetuses and to investigate the performance of the CSP width/length and CSP width/biparietal diameter (BPD) ratios as a diagnostic marker in aneuploidy.
A total of 54 patients, 20 aneuploid and 35 euploid fetuses, between 18 and 37 weeks of gestation, were included in this retrospective study. The CSP width z-score was compared between the two groups. Receiver operating characteristic (ROC) curves were calculated for the CSP width/length and CSP width/BPD ratios to predict aneuploidy.
The median CSP width was 4.8 mm (range, 1.8 to 8.5 mm) in the euploid group, and 5.4 mm (range 3.1 to 8.4 mm) in the aneuploid group. Cavum septum pellucidi width z-score, CSP width/length ratio, and CSP width/BPD ratio were significantly higher in fetuses with aneuploidy than in fetuses with normal karyotype (p = 0.001; p = 0.013; p = 0.028). In the ROC analysis, the CSP width/length ratio had the optimal cutoff value of 0.59, with 72.0% sensitivity and 58.0% specificity, and for the CSP width/BPD ratio, the cutoff value was 0.081 with 83.0% sensitivity and 61.0% specificity for detection of aneuploidy.
CSP width z-score was found to be increased in aneuploid fetuses. The CSP width /BPD ratio can be used as a new marker for predicting aneuploidy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(9):511-516
The aim of the present study is to compare the cavum septum pellucidi (CSP) z-score in euploid and aneuploid fetuses and to investigate the performance of the CSP width/length and CSP width/biparietal diameter (BPD) ratios as a diagnostic marker in aneuploidy.
A total of 54 patients, 20 aneuploid and 35 euploid fetuses, between 18 and 37 weeks of gestation, were included in this retrospective study. The CSP width z-score was compared between the two groups. Receiver operating characteristic (ROC) curves were calculated for the CSP width/length and CSP width/BPD ratios to predict aneuploidy.
The median CSP width was 4.8 mm (range, 1.8 to 8.5 mm) in the euploid group, and 5.4 mm (range 3.1 to 8.4 mm) in the aneuploid group. Cavum septum pellucidi width z-score, CSP width/length ratio, and CSP width/BPD ratio were significantly higher in fetuses with aneuploidy than in fetuses with normal karyotype (p = 0.001; p = 0.013; p = 0.028). In the ROC analysis, the CSP width/length ratio had the optimal cutoff value of 0.59, with 72.0% sensitivity and 58.0% specificity, and for the CSP width/BPD ratio, the cutoff value was 0.081 with 83.0% sensitivity and 61.0% specificity for detection of aneuploidy.
CSP width z-score was found to be increased in aneuploid fetuses. The CSP width /BPD ratio can be used as a new marker for predicting aneuploidy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(5):511-518
The Burch procedure (1961) was considered the gold standard treatment for stress urinary incontinence (SUI) before the midurethral slings (MUSs) were introduced, in 2001.
This historical perspective of the Burch’s timeline can encourage urogynecological surgeons to master the Burch technique as one of the options for surgical treatment of SUI.
Criteria A bibliographic search was performed in the PubMed and National Library of Medicine (NIH) databases with the terms Burch colposuspension AND history AND stress urinary incontinence in the last 20 years. The original article by Burch (1961) was included. The references were read by three authors. The exclusion criterion was studies in non-English languages. Biomedical Library Special Collections were included as historical relevant search.
Some modifications of the technique have been made since the Burch procedure was first described. The interest in this technique has been increasing due to the negative publicity associated with vaginal synthetic mesh products. Twenty-nine relevant articles were included in the present review article, and numerous trials have compared Burch colposuspension with MUS.
This historical perspective enables the scientific community to review a standardized technique for SUI. Burch colposuspension should be considered an appropriate surgical treatment for women with SUI, and an option in urogynecological training programs worldwide.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(5):511-518
The Burch procedure (1961) was considered the gold standard treatment for stress urinary incontinence (SUI) before the midurethral slings (MUSs) were introduced, in 2001.
This historical perspective of the Burch’s timeline can encourage urogynecological surgeons to master the Burch technique as one of the options for surgical treatment of SUI.
Criteria A bibliographic search was performed in the PubMed and National Library of Medicine (NIH) databases with the terms Burch colposuspension AND history AND stress urinary incontinence in the last 20 years. The original article by Burch (1961) was included. The references were read by three authors. The exclusion criterion was studies in non-English languages. Biomedical Library Special Collections were included as historical relevant search.
Some modifications of the technique have been made since the Burch procedure was first described. The interest in this technique has been increasing due to the negative publicity associated with vaginal synthetic mesh products. Twenty-nine relevant articles were included in the present review article, and numerous trials have compared Burch colposuspension with MUS.
This historical perspective enables the scientific community to review a standardized technique for SUI. Burch colposuspension should be considered an appropriate surgical treatment for women with SUI, and an option in urogynecological training programs worldwide.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):511-515
DOI 10.1590/S0100-72032013001100006
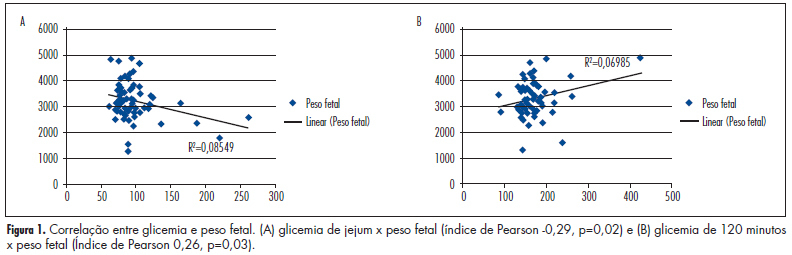
PURPOSE: To evaluate the incidence of maternal and fetal repercussions and glycemic control in women with Gestational Diabetes Mellitus (GDM) using a fasting glucose of 85 mg/dL in the first trimester as a cut-off point and to correlate it with risk factors. METHODS: The medical records of pregnant women followed in the outpatient antenatal high-risk service (PNAR) of HRAN from January 2011 to March 2012 were reviewed and those women diagnosed with GDM were selected for contact and for prenatal card verification. We collected data of age, parity, fasting glucose during the first quarter, the value of the Oral Glucose Tolerance Test (OGTT), Body Mass Index (BMI), mode of delivery, form of control, effects and fetal risk factors for GDM. Statistical analysis was performed using the PSPP 0.6.2 software and consisted of descriptive analysis of frequencies, χ2 test for categorical variables, Student's t-test for independent samples, and Pearson test for correlations, with the level of significance set at 5%. RESULTS: From 408 pregnant women enrolled, 105 were diagnosed with GDM and 71 had complete records or answered to the contact in order to provide the missing information. The GDM-fasting <85 (fasting glucose <85 mg/dL at the first prenatal visit, in the first trimester) group consisted of 29 (40.8%) women and the GDM-fasting >85 (fasting glucose >85 mg/dL at the first prenatal visit, in the first trimester) consisted of 42 (59.1%) women. It was observed that few patients (five in the GDM-fasting <85 group and three in the GDM-fasting >85 group) had no risk factors for GDM. There was a major need for control with insulin in patients of the GDM-fasting >85 group. There was no significant difference related to fetal impact or mode of delivery between the groups. CONCLUSIONS: The first trimester fasting glycemia, with a cut-off value of 85 mg/dL alone or associated with risk factors, does not seem to be a good single predictor of the maternal-fetal effects of GDM.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):511-515
DOI 10.1590/S0100-72032013001100006
PURPOSE: To evaluate the incidence of maternal and fetal repercussions and glycemic control in women with Gestational Diabetes Mellitus (GDM) using a fasting glucose of 85 mg/dL in the first trimester as a cut-off point and to correlate it with risk factors. METHODS: The medical records of pregnant women followed in the outpatient antenatal high-risk service (PNAR) of HRAN from January 2011 to March 2012 were reviewed and those women diagnosed with GDM were selected for contact and for prenatal card verification. We collected data of age, parity, fasting glucose during the first quarter, the value of the Oral Glucose Tolerance Test (OGTT), Body Mass Index (BMI), mode of delivery, form of control, effects and fetal risk factors for GDM. Statistical analysis was performed using the PSPP 0.6.2 software and consisted of descriptive analysis of frequencies, χ2 test for categorical variables, Student's t-test for independent samples, and Pearson test for correlations, with the level of significance set at 5%. RESULTS: From 408 pregnant women enrolled, 105 were diagnosed with GDM and 71 had complete records or answered to the contact in order to provide the missing information. The GDM-fasting <85 (fasting glucose <85 mg/dL at the first prenatal visit, in the first trimester) group consisted of 29 (40.8%) women and the GDM-fasting >85 (fasting glucose >85 mg/dL at the first prenatal visit, in the first trimester) consisted of 42 (59.1%) women. It was observed that few patients (five in the GDM-fasting <85 group and three in the GDM-fasting >85 group) had no risk factors for GDM. There was a major need for control with insulin in patients of the GDM-fasting >85 group. There was no significant difference related to fetal impact or mode of delivery between the groups. CONCLUSIONS: The first trimester fasting glycemia, with a cut-off value of 85 mg/dL alone or associated with risk factors, does not seem to be a good single predictor of the maternal-fetal effects of GDM.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):511-517
DOI 10.1590/S0100-72032012001100006
PURPOSE: To assess the association between clinical symptoms and the diagnosis of malignancy in women with adnexal tumors who underwent surgery. METHODS: Cross-sectional study, in which 105 women with adnexal tumors and indication for laparotomy/laparoscopy were included. All women were treated at a teaching hospital in the state of São Paulo between November 2009 and March 2011. All patients underwent a structured interview about the occurrence of 18 symptoms associated with ovarian cancer. The interview included the severity, frequency, and duration of these symptoms in the 12 months prior to the first medical consultation. The CA125 levels and the ultrasound classification of the tumors were also evaluated. We calculated for each symptom the prevalence ratio with 95% confidence intervals. The golden-standard was the result of the pathological examination of the surgical specimens. RESULTS: Of the 105 women included, 75 (71.4%) had benign tumors and 30 (28.6%) had malignant ones. In women with malignant tumors, the most frequent symptoms were: abdominal bloating (70%), increased abdominal size (67%), pelvic pain (60%), menstrual irregularity (60%), swelling (53%), abdominal pain (50%), backache (50%), and early repletion (50%). Women with benign tumors showed essentially pelvic pain (61%), menstrual irregularities (61%), and abdominal swelling (47%). Symptoms significantly associated with malignancy were: bloating (PR=2.0; 95%CI 1.01 - 3.94), increased abdominal size (PR=2.16; 95%CI 1.12 - 4.16), backache (RP=1.97; 95%CI 1.09 - 3.55), swelling (PR=2.25; 95%CI 1.25 - 4.07), early repletion (RP=2.06; 95%CI 1.14 - 3.70), abdominal mass (PR=1.83; 95%CI 1.01 - 3.30), eating difficulties (PR=1.98; 95%CI 1.10 - 3.56), and postmenopausal bleeding (PR=2.91; 95%CI 1.55 - 5.44). The presence of pelvic pain, constipation, dyspareunia, fatigue, abdominal pain, nausea or vomiting, menstrual irregularity, weight loss, diarrhea, and bleeding after intercourse was similar in both groups. CONCLUSIONS: In women with adnexal tumors including indication of surgical treatment, the preoperative evaluation of symptoms may help predicting malignancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(11):511-517
DOI 10.1590/S0100-72032012001100006
PURPOSE: To assess the association between clinical symptoms and the diagnosis of malignancy in women with adnexal tumors who underwent surgery. METHODS: Cross-sectional study, in which 105 women with adnexal tumors and indication for laparotomy/laparoscopy were included. All women were treated at a teaching hospital in the state of São Paulo between November 2009 and March 2011. All patients underwent a structured interview about the occurrence of 18 symptoms associated with ovarian cancer. The interview included the severity, frequency, and duration of these symptoms in the 12 months prior to the first medical consultation. The CA125 levels and the ultrasound classification of the tumors were also evaluated. We calculated for each symptom the prevalence ratio with 95% confidence intervals. The golden-standard was the result of the pathological examination of the surgical specimens. RESULTS: Of the 105 women included, 75 (71.4%) had benign tumors and 30 (28.6%) had malignant ones. In women with malignant tumors, the most frequent symptoms were: abdominal bloating (70%), increased abdominal size (67%), pelvic pain (60%), menstrual irregularity (60%), swelling (53%), abdominal pain (50%), backache (50%), and early repletion (50%). Women with benign tumors showed essentially pelvic pain (61%), menstrual irregularities (61%), and abdominal swelling (47%). Symptoms significantly associated with malignancy were: bloating (PR=2.0; 95%CI 1.01 - 3.94), increased abdominal size (PR=2.16; 95%CI 1.12 - 4.16), backache (RP=1.97; 95%CI 1.09 - 3.55), swelling (PR=2.25; 95%CI 1.25 - 4.07), early repletion (RP=2.06; 95%CI 1.14 - 3.70), abdominal mass (PR=1.83; 95%CI 1.01 - 3.30), eating difficulties (PR=1.98; 95%CI 1.10 - 3.56), and postmenopausal bleeding (PR=2.91; 95%CI 1.55 - 5.44). The presence of pelvic pain, constipation, dyspareunia, fatigue, abdominal pain, nausea or vomiting, menstrual irregularity, weight loss, diarrhea, and bleeding after intercourse was similar in both groups. CONCLUSIONS: In women with adnexal tumors including indication of surgical treatment, the preoperative evaluation of symptoms may help predicting malignancy.