Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):476-485
DOI 10.1590/S0100-72032010001000002
PURPOSE: to analyze the characteristics of viral infection and the risk factors for high-grade squamous intraepithelial lesion and cervical carcinoma in women with cervical HPV infection. METHODS: a case-control study was conducted on women with cervical HPV at a Gynecology reference service enrolled at the Public Health System, located in Recife, Northeastern Brazil. The groups of cases (72 women with high-grade squamous intraepithelial lesion or cervical cancer) and controls (176 women with normal Pap smear or benign alterations) were investigated for six viral genotypes (HPV 16, 18, 31, 33, 6, 11) in ecto- and endocervical material using MY09/MY11 primers. The independent variables were ranked in three levels of determination: distal (sociodemographic), intermediate (behavioral) and proximal (previous Pap smear). The homogeneity of proportions was tested (χ2), unadjusted Odds Ratios (OR) were obtained and hierarchical logistic regression was applied to the final model, with adjustment of the effect of each variable to the outcome based on the variables in the same and previous levels of causality. RESULTS: the viral genotype of cervical infection was identified in 76.6% of the 248 women participating in the study. High-risk HPV genotypes (83.4% of cases and 67.1% of controls) were predominant, especially HPV 16 and 31. The distal risk factors identified were: living in a rural area (OR=2.71, 95%CI: 1.18-6.23), less than three years of study (OR=3.97, 95%CI: 2.09-7.54) and family income below two minimum wages (OR=3.30, 95%CI: 1.04-10.51); intermediate: four or more pregnancies (OR=2.00, 95%CI: 1.06-3.76); and proximal: absence of a previous Pap smear (OR=9.74, 95%CI: 2.48-38.28). CONCLUSIONS: genotypes 16 and 31 of cervical HPV infection are predominant among women assisted by the Public Health System in Northeastern Brazil. Socioeconomic and reproductive factors, as well as the absence of cytological screening, represent risk factors for the progression of infection to high-grade squamous intraepithelial lesion and cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):476-485
DOI 10.1590/S0100-72032010001000002
PURPOSE: to analyze the characteristics of viral infection and the risk factors for high-grade squamous intraepithelial lesion and cervical carcinoma in women with cervical HPV infection. METHODS: a case-control study was conducted on women with cervical HPV at a Gynecology reference service enrolled at the Public Health System, located in Recife, Northeastern Brazil. The groups of cases (72 women with high-grade squamous intraepithelial lesion or cervical cancer) and controls (176 women with normal Pap smear or benign alterations) were investigated for six viral genotypes (HPV 16, 18, 31, 33, 6, 11) in ecto- and endocervical material using MY09/MY11 primers. The independent variables were ranked in three levels of determination: distal (sociodemographic), intermediate (behavioral) and proximal (previous Pap smear). The homogeneity of proportions was tested (χ2), unadjusted Odds Ratios (OR) were obtained and hierarchical logistic regression was applied to the final model, with adjustment of the effect of each variable to the outcome based on the variables in the same and previous levels of causality. RESULTS: the viral genotype of cervical infection was identified in 76.6% of the 248 women participating in the study. High-risk HPV genotypes (83.4% of cases and 67.1% of controls) were predominant, especially HPV 16 and 31. The distal risk factors identified were: living in a rural area (OR=2.71, 95%CI: 1.18-6.23), less than three years of study (OR=3.97, 95%CI: 2.09-7.54) and family income below two minimum wages (OR=3.30, 95%CI: 1.04-10.51); intermediate: four or more pregnancies (OR=2.00, 95%CI: 1.06-3.76); and proximal: absence of a previous Pap smear (OR=9.74, 95%CI: 2.48-38.28). CONCLUSIONS: genotypes 16 and 31 of cervical HPV infection are predominant among women assisted by the Public Health System in Northeastern Brazil. Socioeconomic and reproductive factors, as well as the absence of cytological screening, represent risk factors for the progression of infection to high-grade squamous intraepithelial lesion and cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(8):476-484
Labor induction does not always result in vaginal delivery, and can expose both the mother and the fetus to the risks inherent to the induction procedure or a possible cesarean section. Transvaginal sonography (TVS) of the cervix is a useful tool to predict prematurity; in the present study, this tool was used to evaluate postterm induction.
We evaluated the ultrasound characteristics of the cervix (cervical length, cervical funneling, internal os dilation, the presence or absence of the cervical gland area [CGA], and the morphological changes of the cervix as a result of applying fundal pressure) before the onset of labor induction among women with postterm pregnancy to identify the possible predictors of failed labor induction. The Bishop score (BS) was used for comparison purposes. Three groups were evaluated: successful versus unsuccessful induction; vaginal delivery versus cesarean delivery (excluding cases of acute fetal distress [AFD]); and vaginal delivery versus cesarean delivery (including cases of AFD). A fourth group including only the primiparous women from the three previous groups was also evaluated.
Based on the studied characteristics and combinations of variables, a cervical length ≥ 3.0 cm and a BS ≤ 2 were the best predictors of induction failure.
Although TVS is useful for screening for induction failure, this tool should not be used as an indication for cesarean section.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(8):476-484
Labor induction does not always result in vaginal delivery, and can expose both the mother and the fetus to the risks inherent to the induction procedure or a possible cesarean section. Transvaginal sonography (TVS) of the cervix is a useful tool to predict prematurity; in the present study, this tool was used to evaluate postterm induction.
We evaluated the ultrasound characteristics of the cervix (cervical length, cervical funneling, internal os dilation, the presence or absence of the cervical gland area [CGA], and the morphological changes of the cervix as a result of applying fundal pressure) before the onset of labor induction among women with postterm pregnancy to identify the possible predictors of failed labor induction. The Bishop score (BS) was used for comparison purposes. Three groups were evaluated: successful versus unsuccessful induction; vaginal delivery versus cesarean delivery (excluding cases of acute fetal distress [AFD]); and vaginal delivery versus cesarean delivery (including cases of AFD). A fourth group including only the primiparous women from the three previous groups was also evaluated.
Based on the studied characteristics and combinations of variables, a cervical length ≥ 3.0 cm and a BS ≤ 2 were the best predictors of induction failure.
Although TVS is useful for screening for induction failure, this tool should not be used as an indication for cesarean section.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(8):476-485
To evaluate the factors associated with complete myomectomy in a single surgical procedure and the aspects related to the early complications.
A cross-sectional study with women with submucous myomas. The dependent variables were the complete myomectomy performed in a single hysteroscopic procedure, and the presence of early complications related to the procedure.
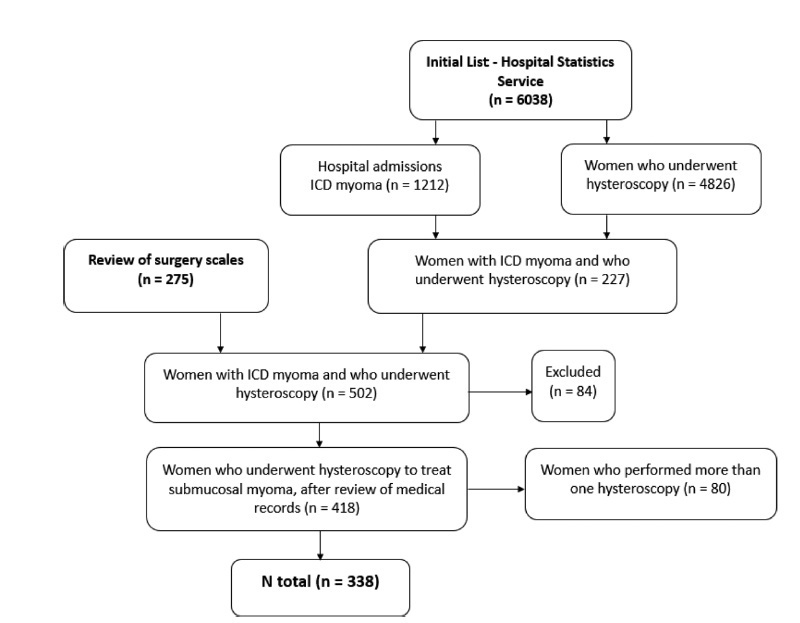
We identified 338 women who underwent hysteroscopic myomectomy. In 89.05% of the cases, there was a single fibroid to be treated. According to the classification of the International Federation of Gynecology and Obstetrics (Fédération Internationale de Gynécologie et d’Obstétrique, FIGO, in French),most fibroids were of grade 0 (66.96%), followed by grade 1 (20.54%), and grade 2 (12.50%). The myomectomies were complete in 63.31% of the cases, and the factors independently associated with complete myomectomy were the diameter of the largest fibroid (prevalence ratio [PR]: 0.97; 95% confidence interval [95%CI]: 0.96-0.98) and the classification 0 of the fibroid according to the FIGO (PR: 2.04; 95%CI: 1.18-3.52). We observed early complications in 13.01% of the hysteroscopic procedures (4.44% presented excessive bleeding during the procedure, 4.14%, uterine perforation, 2.66%, false route, 1.78%, fluid overload, 0.59%, exploratory laparotomy, and 0.3%, postoperative infection). The only independent factor associated with the occurrence of early complications was incomplete myomectomy (PR: 2.77; 95%CI: 1.43-5.38).
Our results show that hysteroscopic myomectomy may result in up to 13% of complications, and the chance of complete resection is greater in small and completely intracavitary fibroids; women with larger fibroids and with a high degree of myometrial penetration have a greater chance of developing complications from hysteroscopic myomectomy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(8):476-485
To evaluate the factors associated with complete myomectomy in a single surgical procedure and the aspects related to the early complications.
A cross-sectional study with women with submucous myomas. The dependent variables were the complete myomectomy performed in a single hysteroscopic procedure, and the presence of early complications related to the procedure.
We identified 338 women who underwent hysteroscopic myomectomy. In 89.05% of the cases, there was a single fibroid to be treated. According to the classification of the International Federation of Gynecology and Obstetrics (Fédération Internationale de Gynécologie et d’Obstétrique, FIGO, in French),most fibroids were of grade 0 (66.96%), followed by grade 1 (20.54%), and grade 2 (12.50%). The myomectomies were complete in 63.31% of the cases, and the factors independently associated with complete myomectomy were the diameter of the largest fibroid (prevalence ratio [PR]: 0.97; 95% confidence interval [95%CI]: 0.96-0.98) and the classification 0 of the fibroid according to the FIGO (PR: 2.04; 95%CI: 1.18-3.52). We observed early complications in 13.01% of the hysteroscopic procedures (4.44% presented excessive bleeding during the procedure, 4.14%, uterine perforation, 2.66%, false route, 1.78%, fluid overload, 0.59%, exploratory laparotomy, and 0.3%, postoperative infection). The only independent factor associated with the occurrence of early complications was incomplete myomectomy (PR: 2.77; 95%CI: 1.43-5.38).
Our results show that hysteroscopic myomectomy may result in up to 13% of complications, and the chance of complete resection is greater in small and completely intracavitary fibroids; women with larger fibroids and with a high degree of myometrial penetration have a greater chance of developing complications from hysteroscopic myomectomy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(8):477-490
To compare surgical treatments for stress urinary incontinence in terms of efficiency and complications.
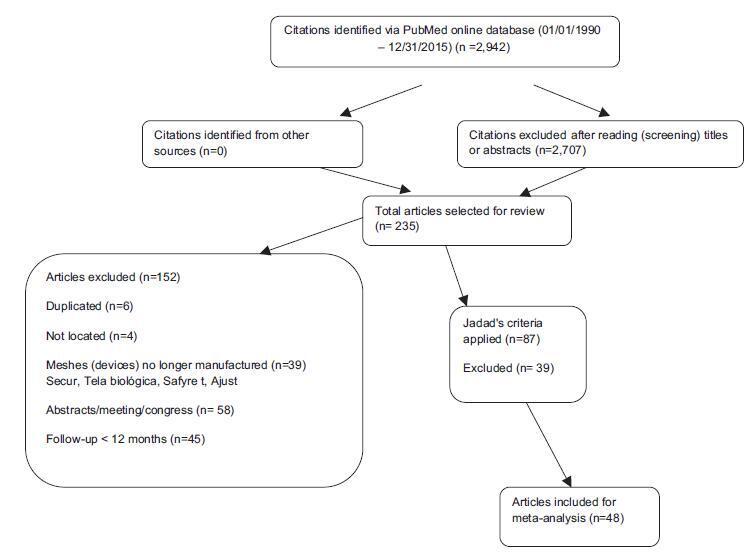
We searched the MEDLINE and COCHRANE databases using the terms stress urinary incontinence, surgical treatment for stress urinary incontinence and sling. Selection of Studies Forty-eight studies were selected, which amounted to a total of 6,881 patients with scores equal to or higher than 3 in the Jadad scale.
Each study was read by one of the authors, added to a standardized table and checked by a second author. We extracted data on intervention details, follow-up time, the results of treatment and adverse events.
Comparing retropubic versus transobturator slings, the former was superior for both objective (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.05-1.54) and subjective (OR, 1.23; 95% CI, 1.02-1.48) cures. Between minislings versus other slings, there was a difference favoring other slings for subjective cure (OR, 0.58; 95% CI, 0.39- 0.86). Between pubovaginal sling versus Burch surgery, there was a difference for both objective (OR, 2.04; 95% CI, 1.50-2.77) and subjective (OR, 1.64; 95% CI, 1.10-2.44) cures, favoring pubovaginal sling. Therewas no difference in the groups: midurethral slings versus Burch, pubovaginal sling versus midurethral slings, transobturator slings, minislings versus other slings (objective cure). Retropubic and pubovaginal slings are more retentionist. Retropubic slings have more bladder perforation, and transobturator slings, more leg and groin pain, neurological lesion and vaginal perforation.
Pubovaginal slings are superior to Burch colposuspension surgery but exhibit more retention. Retropubic slings are superior to transobturator slings, with more adverse events. Other slings are superior to minislings in the subjective aspect. There was no difference in the comparisons between midurethral slings versus Burch colposuspension surgery, pubovaginal versus midurethral slings, and inside-out versus outside-in transobturator slings.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(8):477-490
To compare surgical treatments for stress urinary incontinence in terms of efficiency and complications.
We searched the MEDLINE and COCHRANE databases using the terms stress urinary incontinence, surgical treatment for stress urinary incontinence and sling. Selection of Studies Forty-eight studies were selected, which amounted to a total of 6,881 patients with scores equal to or higher than 3 in the Jadad scale.
Each study was read by one of the authors, added to a standardized table and checked by a second author. We extracted data on intervention details, follow-up time, the results of treatment and adverse events.
Comparing retropubic versus transobturator slings, the former was superior for both objective (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.05-1.54) and subjective (OR, 1.23; 95% CI, 1.02-1.48) cures. Between minislings versus other slings, there was a difference favoring other slings for subjective cure (OR, 0.58; 95% CI, 0.39- 0.86). Between pubovaginal sling versus Burch surgery, there was a difference for both objective (OR, 2.04; 95% CI, 1.50-2.77) and subjective (OR, 1.64; 95% CI, 1.10-2.44) cures, favoring pubovaginal sling. Therewas no difference in the groups: midurethral slings versus Burch, pubovaginal sling versus midurethral slings, transobturator slings, minislings versus other slings (objective cure). Retropubic and pubovaginal slings are more retentionist. Retropubic slings have more bladder perforation, and transobturator slings, more leg and groin pain, neurological lesion and vaginal perforation.
Pubovaginal slings are superior to Burch colposuspension surgery but exhibit more retention. Retropubic slings are superior to transobturator slings, with more adverse events. Other slings are superior to minislings in the subjective aspect. There was no difference in the comparisons between midurethral slings versus Burch colposuspension surgery, pubovaginal versus midurethral slings, and inside-out versus outside-in transobturator slings.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(9):477-478
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(9):477-478
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(10):477-479
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(10):477-479
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(6):477-482
DOI 10.1590/S0100-72032004000600009
OBJECTIVE: to evaluate the neonatal morbidity and mortality related to mothers at the age of 35 or older than that. METHODS: in 2377 births in a year, 316 newborns (13.26%) from mothers at the age of 35 or more were selected for the study. These women were compared to pregnant controls aged 20 to 29, randomly selected among the 1170 women in the same age group (49,2%). For the inclusion criteria, pregnancies should have been over 22 weeks and the newborns should have weighted 500g or more at birth. Fourteen twin cases were excluded. To evaluate mortality and morbidity the following variables were considered: Apgar Index, birth weight, newborn health conditions, fetal malformations and neonatal mortality until hospital discharge. RESULTS: when analyzed as a whole, nulliparous and multiparous women showed significantly less favorable perinatal results for the selected group of women at 35 or more years old as compared with pregnant controls, what was not sustained when the nulliparous were excluded. Multiparous at the age of 35 or over presented a higher rate of low Apgar index in the 1st minute: 21.3 and 13.1%: (p<0,0033); small NB for the gestational age: 15.2% and 6.7% (p<0,02); big NB for the gestational age: 5.7 and 0.0% (p<0,02); low weight at birth: 23.8 and 14,5% (p<0,01), and prematurity, 16,7 and 6,7%, (p<0,005). Significant differences were not found for the Apgar index in the 5th minute, fetal malformations, newborn health conditions at hospital discharge and neonatal mortality. CONCLUSIONS: Neonatal morbidity increased among pregnant women at the age of 35 and older, but not the neonatal mortality.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(6):477-482
DOI 10.1590/S0100-72032004000600009
OBJECTIVE: to evaluate the neonatal morbidity and mortality related to mothers at the age of 35 or older than that. METHODS: in 2377 births in a year, 316 newborns (13.26%) from mothers at the age of 35 or more were selected for the study. These women were compared to pregnant controls aged 20 to 29, randomly selected among the 1170 women in the same age group (49,2%). For the inclusion criteria, pregnancies should have been over 22 weeks and the newborns should have weighted 500g or more at birth. Fourteen twin cases were excluded. To evaluate mortality and morbidity the following variables were considered: Apgar Index, birth weight, newborn health conditions, fetal malformations and neonatal mortality until hospital discharge. RESULTS: when analyzed as a whole, nulliparous and multiparous women showed significantly less favorable perinatal results for the selected group of women at 35 or more years old as compared with pregnant controls, what was not sustained when the nulliparous were excluded. Multiparous at the age of 35 or over presented a higher rate of low Apgar index in the 1st minute: 21.3 and 13.1%: (p<0,0033); small NB for the gestational age: 15.2% and 6.7% (p<0,02); big NB for the gestational age: 5.7 and 0.0% (p<0,02); low weight at birth: 23.8 and 14,5% (p<0,01), and prematurity, 16,7 and 6,7%, (p<0,005). Significant differences were not found for the Apgar index in the 5th minute, fetal malformations, newborn health conditions at hospital discharge and neonatal mortality. CONCLUSIONS: Neonatal morbidity increased among pregnant women at the age of 35 and older, but not the neonatal mortality.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):477-482
DOI 10.1590/S0100-72032013001100001
PURPOSE: To evaluate the methodological and statistical design evolution of the publications in the Brazilian Journal of Gynecology and Obstetrics (RBGO) from resolution 196/96. METHODS: A review of 133 articles published in 1999 (65) and 2009 (68) was performed by two independent reviewers with training in clinical epidemiology and methodology of scientific research. We included all original clinical articles, case and series reports and excluded editorials, letters to the editor, systematic reviews, experimental studies, opinion articles, besides abstracts of theses and dissertations. Characteristics related to the methodological quality of the studies were analyzed in each article using a checklist that evaluated two criteria: methodological aspects and statistical procedures. We used descriptive statistics and the χ2 test for comparison of the two years. RESULTS: There was a difference between 1999 and 2009 regarding the study and statistical design, with more accuracy in the procedures and the use of more robust tests between 1999 and 2009. CONCLUSIONS: In RBGO, we observed an evolution in the methods of published articles and a more in-depth use of the statistical analyses, with more sophisticated tests such as regression and multilevel analyses, which are essential techniques for the knowledge and planning of health interventions, leading to fewer interpretation errors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(11):477-482
DOI 10.1590/S0100-72032013001100001
PURPOSE: To evaluate the methodological and statistical design evolution of the publications in the Brazilian Journal of Gynecology and Obstetrics (RBGO) from resolution 196/96. METHODS: A review of 133 articles published in 1999 (65) and 2009 (68) was performed by two independent reviewers with training in clinical epidemiology and methodology of scientific research. We included all original clinical articles, case and series reports and excluded editorials, letters to the editor, systematic reviews, experimental studies, opinion articles, besides abstracts of theses and dissertations. Characteristics related to the methodological quality of the studies were analyzed in each article using a checklist that evaluated two criteria: methodological aspects and statistical procedures. We used descriptive statistics and the χ2 test for comparison of the two years. RESULTS: There was a difference between 1999 and 2009 regarding the study and statistical design, with more accuracy in the procedures and the use of more robust tests between 1999 and 2009. CONCLUSIONS: In RBGO, we observed an evolution in the methods of published articles and a more in-depth use of the statistical analyses, with more sophisticated tests such as regression and multilevel analyses, which are essential techniques for the knowledge and planning of health interventions, leading to fewer interpretation errors.