You searched for:"Melania Maria Ramos Amorim"
We found (14) results for your search.Summary
Rev Bras Ginecol Obstet. 2020;42(8):445-447
Summary
Rev Bras Ginecol Obstet. 2020;42(8):445-447
Summary
Rev Bras Ginecol Obstet. 2010;32(9):459-468
DOI 10.1590/S0100-72032010000900008
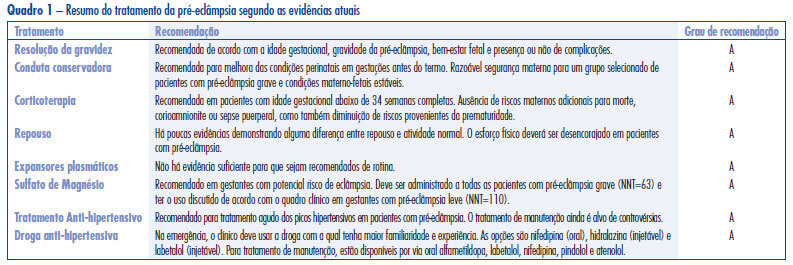
Hypertensive disorders in pregnancy deserve special attention in the setting of global public health. Currently, they represent the third cause of maternal mortality in the world and first in Brazil. From a practical standpoint, pre-eclampsia remains a syndrome that leads to serious repercussions on maternal and fetal mortality and its etiology is not well known. Currently, the best treatment for forms of pre-eclampsia is being discussed at different times in pregnancy and puerperium, with the objective to reduce the high rates of maternal and fetal morbidity and mortality. Considering the pathophysiology of the event, anticipation of delivery is the best treatment for pre-eclampsia. The use of magnesium sulfate is recommended in all cases of severe pre-eclampsia and eclampsia for prevention and treatment of seizures. Likewise, treatment of hypertensive crises is recommended. Hydralazine, nifedipine and labetalol have been the most commonly used drugs for this purpose, but their use depends on the familiarity of the treating physician. Antenatal corticoid therapy is indicated whenever there is an imminent risk of preterm delivery between 24 and 34 weeks. In contrast, there is insufficient evidence to recommend bed rest and routine plasma volume expansion, and there is an urgent need for randomized clinical trials to determine whether maintenance antihypertensive treatment in pregnant women has benefits or risks for mothers and fetuses in all clinical forms of disease, particularly in cases of pure pre-eclampsia.
Summary
Rev Bras Ginecol Obstet. 2010;32(9):459-468
DOI 10.1590/S0100-72032010000900008
Hypertensive disorders in pregnancy deserve special attention in the setting of global public health. Currently, they represent the third cause of maternal mortality in the world and first in Brazil. From a practical standpoint, pre-eclampsia remains a syndrome that leads to serious repercussions on maternal and fetal mortality and its etiology is not well known. Currently, the best treatment for forms of pre-eclampsia is being discussed at different times in pregnancy and puerperium, with the objective to reduce the high rates of maternal and fetal morbidity and mortality. Considering the pathophysiology of the event, anticipation of delivery is the best treatment for pre-eclampsia. The use of magnesium sulfate is recommended in all cases of severe pre-eclampsia and eclampsia for prevention and treatment of seizures. Likewise, treatment of hypertensive crises is recommended. Hydralazine, nifedipine and labetalol have been the most commonly used drugs for this purpose, but their use depends on the familiarity of the treating physician. Antenatal corticoid therapy is indicated whenever there is an imminent risk of preterm delivery between 24 and 34 weeks. In contrast, there is insufficient evidence to recommend bed rest and routine plasma volume expansion, and there is an urgent need for randomized clinical trials to determine whether maintenance antihypertensive treatment in pregnant women has benefits or risks for mothers and fetuses in all clinical forms of disease, particularly in cases of pure pre-eclampsia.
Summary
Rev Bras Ginecol Obstet. 2015;37(10):480-485
DOI 10.1590/SO100-720320150005279
To determine the prevalence of HPV-induced lesions in the anal canal of women with cervical intraepithelial neoplasia (CIN) grade 2/3.
A cross-sectional study was carried out from December 2008 to June 2009, in Pernambuco, northeastern Brazil. Only women with grade 2/3 CIN were included, and those who could not undergo anoscopy during their first visit were excluded. A cyttobrush was used for sample collection in order to identify HPV DNA through PCR and anal cytology. An anal biopsy was obtained in cases of abnormal anal cytology or major alterations in high resolution anoscopy (HRA).
Thirty-two percent (n=37/115) of HRA were normal and 63.5% (n=73/115) showed acetowhite epithelium. Twenty-two percent (n=26/115) of anal cytologies were abnormal. Among the latter, 12.2% (n=14/26) were low-grade anal intraepithelial lesions and 3.4% (n=4/26) were high-grade anal intraepithelial lesions. Twenty-two anal biopsies were performed, 13.7% of which (n=3/22) were grade 2 anal intraepithelial neoplasia (AIN2) and 9% (n=2/22) were grade 3 AIN. Th HPV DNA was identified in 72.1% of cases (n=83/115).
Women with CIN grade 2/3 showed a high prevalence of anal HPV infection and HPV-induced lesions.
Summary
Rev Bras Ginecol Obstet. 2015;37(10):480-485
DOI 10.1590/SO100-720320150005279
To determine the prevalence of HPV-induced lesions in the anal canal of women with cervical intraepithelial neoplasia (CIN) grade 2/3.
A cross-sectional study was carried out from December 2008 to June 2009, in Pernambuco, northeastern Brazil. Only women with grade 2/3 CIN were included, and those who could not undergo anoscopy during their first visit were excluded. A cyttobrush was used for sample collection in order to identify HPV DNA through PCR and anal cytology. An anal biopsy was obtained in cases of abnormal anal cytology or major alterations in high resolution anoscopy (HRA).
Thirty-two percent (n=37/115) of HRA were normal and 63.5% (n=73/115) showed acetowhite epithelium. Twenty-two percent (n=26/115) of anal cytologies were abnormal. Among the latter, 12.2% (n=14/26) were low-grade anal intraepithelial lesions and 3.4% (n=4/26) were high-grade anal intraepithelial lesions. Twenty-two anal biopsies were performed, 13.7% of which (n=3/22) were grade 2 anal intraepithelial neoplasia (AIN2) and 9% (n=2/22) were grade 3 AIN. Th HPV DNA was identified in 72.1% of cases (n=83/115).
Women with CIN grade 2/3 showed a high prevalence of anal HPV infection and HPV-induced lesions.
Summary
Rev Bras Ginecol Obstet. 2019;41(9):531-538
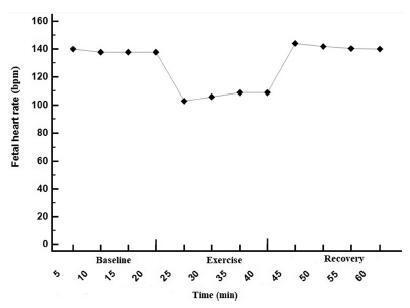
To determine the effect of treadmill walking on maternal heart rate (MHR) and cardiotocographic parameters (basal fetal heart rate [FHR], active fetal movements [AFM], number of accelerations and decelerations, and short-term variation [STV] and long-term variation [LTV] of fetal heart rate) in pregnant women at 36 weeks.
A nonrandomized, open clinical trial involving 88 healthy pregnant women submitted to moderate intensity walking and computed cardiotocography in 3 20- minute periods (resting, treadmill walking, and postexercise recovery).
The mean FHR decreased during walking (resting: 137 bpm; treadmill: 98 bpm; recovery: 140 bpm; p<0.001), with bradycardia occurring in 56% of the fetuses in the first 10minutes of exercise, and in 47% after 20minutes. Bradycardia was not detected in the other phases. The mean STV and HV were 7.9, 17.0, and 8.0 milliseconds (p<0.001) and 7.6, 10.8 and 7.6 bpm (p=0.002) in the resting, walking and recovery phases, respectively. Themean number of fetalmovements in 1 hour was 29.9, 22.2 and 45.5, respectively, in the 3 periods (p<0.001). In overweight/obese women, the mean FHR was lower (p=0.02). Following the logistic regression analysis, two variables remained significantly associated with bradycardia: maternal fitness in the 28th week of pregnancy (protective effect) and maternal weight (increased risk).
In healthy fetuses, physical exercise proved to be safe, since, although FHR and AFM decreased during treadmill walking, an increase in SVT and LTV was observed.
Summary
Rev Bras Ginecol Obstet. 2019;41(9):531-538
To determine the effect of treadmill walking on maternal heart rate (MHR) and cardiotocographic parameters (basal fetal heart rate [FHR], active fetal movements [AFM], number of accelerations and decelerations, and short-term variation [STV] and long-term variation [LTV] of fetal heart rate) in pregnant women at 36 weeks.
A nonrandomized, open clinical trial involving 88 healthy pregnant women submitted to moderate intensity walking and computed cardiotocography in 3 20- minute periods (resting, treadmill walking, and postexercise recovery).
The mean FHR decreased during walking (resting: 137 bpm; treadmill: 98 bpm; recovery: 140 bpm; p<0.001), with bradycardia occurring in 56% of the fetuses in the first 10minutes of exercise, and in 47% after 20minutes. Bradycardia was not detected in the other phases. The mean STV and HV were 7.9, 17.0, and 8.0 milliseconds (p<0.001) and 7.6, 10.8 and 7.6 bpm (p=0.002) in the resting, walking and recovery phases, respectively. Themean number of fetalmovements in 1 hour was 29.9, 22.2 and 45.5, respectively, in the 3 periods (p<0.001). In overweight/obese women, the mean FHR was lower (p=0.02). Following the logistic regression analysis, two variables remained significantly associated with bradycardia: maternal fitness in the 28th week of pregnancy (protective effect) and maternal weight (increased risk).
In healthy fetuses, physical exercise proved to be safe, since, although FHR and AFM decreased during treadmill walking, an increase in SVT and LTV was observed.
Summary
Rev Bras Ginecol Obstet. 2009;31(11):552-558
DOI 10.1590/S0100-72032009001100005
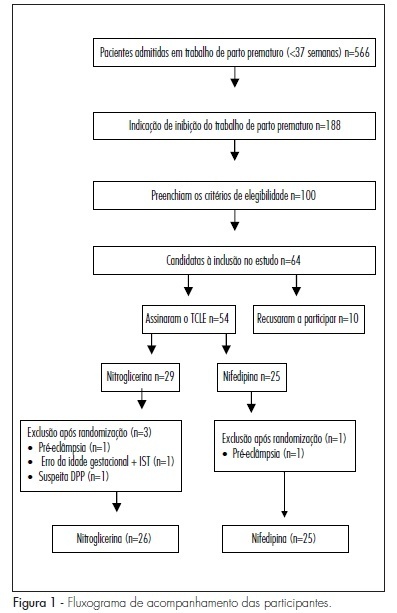
PURPOSE: to compare the effectiveness of transdermal nitroglycerin with oral nifedipine in the inhibition of preterm delivery. METHODS: a clinical essay has been performed with 50 women in preterm delivery, randomly divided into two groups, 24 receiving oral nifedipine (20 mg), and 26, transdermal nitroglycerin (10 mg patch). Patients with a single gestation, between the 24th and the 34th weeks and diagnosis of preterm delivery were selected. Women with fetal malformation and clinical or obstetric diseases were excluded. The variables analyzed were: effective tocolysis, time needed for tocolysis, recurrence frequency, progression to preterm delivery, and side effects. RESULTS: tocolysis efficacy in the first 12 hours was similar between the groups (nitroglycerin: 84.6% versus nifedipine: 87.5%; p=0.50). The time average time needed for tocolysis was also similar (6.6 versus 5.8 hours; p=0.30). There was no difference between the groups, concerning the recurrence of preterm delivery (26.9 versus 16.7%; p=0.30), and neither in the rate of preterm delivery within 48 hours (15.4 versus 12.5%; p=0.50). Nevertheless, the cephalea rate was significantly higher in the Nitroglycerin Group (30.8 versus 8.3%; p=0.04). CONCLUSIONS: transdermal nitroglycerin has presented similar effectiveness to oral nifedipine to inhibit preterm delivery in the first 48 hours, however with higher cephalea frequency.
Summary
Rev Bras Ginecol Obstet. 2009;31(11):552-558
DOI 10.1590/S0100-72032009001100005
PURPOSE: to compare the effectiveness of transdermal nitroglycerin with oral nifedipine in the inhibition of preterm delivery. METHODS: a clinical essay has been performed with 50 women in preterm delivery, randomly divided into two groups, 24 receiving oral nifedipine (20 mg), and 26, transdermal nitroglycerin (10 mg patch). Patients with a single gestation, between the 24th and the 34th weeks and diagnosis of preterm delivery were selected. Women with fetal malformation and clinical or obstetric diseases were excluded. The variables analyzed were: effective tocolysis, time needed for tocolysis, recurrence frequency, progression to preterm delivery, and side effects. RESULTS: tocolysis efficacy in the first 12 hours was similar between the groups (nitroglycerin: 84.6% versus nifedipine: 87.5%; p=0.50). The time average time needed for tocolysis was also similar (6.6 versus 5.8 hours; p=0.30). There was no difference between the groups, concerning the recurrence of preterm delivery (26.9 versus 16.7%; p=0.30), and neither in the rate of preterm delivery within 48 hours (15.4 versus 12.5%; p=0.50). Nevertheless, the cephalea rate was significantly higher in the Nitroglycerin Group (30.8 versus 8.3%; p=0.04). CONCLUSIONS: transdermal nitroglycerin has presented similar effectiveness to oral nifedipine to inhibit preterm delivery in the first 48 hours, however with higher cephalea frequency.
Summary
Rev Bras Ginecol Obstet. 2009;31(2):82-88
DOI 10.1590/S0100-72032009000200006
PURPOSE: to evaluate the effect of magnesium sulphate on the pulsatility index (PI) of the uterine, umbilical and fetal middle cerebral arteries, according to the persistency or not of the bilateral protodiastolic notch of the uterine arteries in severe pre-eclampsia. METHODS: a cohort study including 40 pregnant women with severe pre-eclampsia, 23 of them presenting bilateral protodiastolic notch, and 17, unilateral/absent notch. The patients were submitted to Doppler velocimetry before and 20 minutes after the intravenous administration of 6 g of magnesium sulphate. The examination was carried out with the patient in semi-Fowler position, the sonograms being obtained during fetal inactivity, in apnea and absent uterine contraction periods. All the exams were performed by two researchers, the average being considered as the final result. Wilcoxon's test was used to compare the PI, before and after magnesium sulphate in both groups. The difference between the two measurements (before and after magnesium sulphate) was compared between the groups (bilateral incision and unilateral/absent incision) using the Mann-Whitney test. RESULTS: there was a significant increase in the maternal heart rate (MHR) and decrease in the maternal blood pressure, and in the PI medians of the two uterine arteries and in the fetal middle cerebral artery, after magnesium sulphate in both groups. There was a significant decrease in the PI of the left uterine artery and in the umbilical artery, only in the protodiastolic unilateral/absent notch group. Nevertheless, it was not found any significant difference regarding the PI of the right uterine artery, or the cerebral/umbilical relationship, before and after magnesium sulphate in each group. No difference between the groups was found, before and after magnesium sulphate, for any of the studied outcomes. CONCLUSIONS: after the intravenous administration of 6 g of magnesium sulphate to patients with severe pre-eclampsia, a decrease in blood pressure and in the PI of the uterine, umbilical and fetal middle cerebral arteries occurs, besides the increase in the MHR, not influenced by the presence of bilateral protodiastolic notch in the uterine arteries.
Summary
Rev Bras Ginecol Obstet. 2009;31(2):82-88
DOI 10.1590/S0100-72032009000200006
PURPOSE: to evaluate the effect of magnesium sulphate on the pulsatility index (PI) of the uterine, umbilical and fetal middle cerebral arteries, according to the persistency or not of the bilateral protodiastolic notch of the uterine arteries in severe pre-eclampsia. METHODS: a cohort study including 40 pregnant women with severe pre-eclampsia, 23 of them presenting bilateral protodiastolic notch, and 17, unilateral/absent notch. The patients were submitted to Doppler velocimetry before and 20 minutes after the intravenous administration of 6 g of magnesium sulphate. The examination was carried out with the patient in semi-Fowler position, the sonograms being obtained during fetal inactivity, in apnea and absent uterine contraction periods. All the exams were performed by two researchers, the average being considered as the final result. Wilcoxon's test was used to compare the PI, before and after magnesium sulphate in both groups. The difference between the two measurements (before and after magnesium sulphate) was compared between the groups (bilateral incision and unilateral/absent incision) using the Mann-Whitney test. RESULTS: there was a significant increase in the maternal heart rate (MHR) and decrease in the maternal blood pressure, and in the PI medians of the two uterine arteries and in the fetal middle cerebral artery, after magnesium sulphate in both groups. There was a significant decrease in the PI of the left uterine artery and in the umbilical artery, only in the protodiastolic unilateral/absent notch group. Nevertheless, it was not found any significant difference regarding the PI of the right uterine artery, or the cerebral/umbilical relationship, before and after magnesium sulphate in each group. No difference between the groups was found, before and after magnesium sulphate, for any of the studied outcomes. CONCLUSIONS: after the intravenous administration of 6 g of magnesium sulphate to patients with severe pre-eclampsia, a decrease in blood pressure and in the PI of the uterine, umbilical and fetal middle cerebral arteries occurs, besides the increase in the MHR, not influenced by the presence of bilateral protodiastolic notch in the uterine arteries.