You searched for:"José Carlos Peraçoli"
We found (15) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(9):433-439
DOI 10.1590/S0100-72032009000900003
PURPOSE: the main goal of this study is to evaluate the emotional conditions among mothers of newborns with visible malformation (Group M) and mothers of eutrophic newborns (Group E) soon after birth. METHODS: twenty-two mothers from the Group M were matched by age and number of children to 22 mothers of the Group E. They were assessed through the Beck Depression Inventory (BDI) and the State-Trait Anxiety Inventory (STAI). The data were complemented by interviews and analyses of the medical files of both mother and child. RESULTS: the results have shown significant differences in the mean scores of the three subscales (trait anxiety, state anxiety, dysphoria/depression) between the two groups of mothers. In terms of clinical signs, there were a significantly larger percentage of mothers from Group M identified with depression and anxiety after the child's birth, and for both conditions when compared with mothers from Group E. Although the results may reflect characteristics of the maternal personality, the trait anxiety was significantly more evident in mothers of malformed children, especially due to the child's health condition, its referral to the ICU and his/her condition regarding their future life. CONCLUSION: the percentage of mothers with clinical depression and anxiety suggests the need for either individual or group support to attend the needs of the mothers and mitigate the adverse effects of stressors throughout the child's development. Support should also be provided during pregnancy, when the mothers currently receive the news about the malformation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(9):433-439
DOI 10.1590/S0100-72032009000900003
PURPOSE: the main goal of this study is to evaluate the emotional conditions among mothers of newborns with visible malformation (Group M) and mothers of eutrophic newborns (Group E) soon after birth. METHODS: twenty-two mothers from the Group M were matched by age and number of children to 22 mothers of the Group E. They were assessed through the Beck Depression Inventory (BDI) and the State-Trait Anxiety Inventory (STAI). The data were complemented by interviews and analyses of the medical files of both mother and child. RESULTS: the results have shown significant differences in the mean scores of the three subscales (trait anxiety, state anxiety, dysphoria/depression) between the two groups of mothers. In terms of clinical signs, there were a significantly larger percentage of mothers from Group M identified with depression and anxiety after the child's birth, and for both conditions when compared with mothers from Group E. Although the results may reflect characteristics of the maternal personality, the trait anxiety was significantly more evident in mothers of malformed children, especially due to the child's health condition, its referral to the ICU and his/her condition regarding their future life. CONCLUSION: the percentage of mothers with clinical depression and anxiety suggests the need for either individual or group support to attend the needs of the mothers and mitigate the adverse effects of stressors throughout the child's development. Support should also be provided during pregnancy, when the mothers currently receive the news about the malformation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):445-448
DOI 10.1590/S0100-72032003000600010
Development of preeclampsia/eclampsia prior to 20 weeks of pregnancy should raise the suspicion of hydatidiform mole. We report a case of complete hydatidiform mole (CHM) concurrent with eclampsia in a 20-year-old patient with vaginal bleeding, anemia, large uterine size, and ovary cysts associated with hypertension and proteinuria. Plasmatic b-hCG levels were high and there was abnormal thyroid function. The ultrasonographic findings were compatible with CHM. After uterine evacuation, the patient had headache and visual alterations, followed by tonic-clonic seizures, which ceased with the administration of 50% magnesium sulfate. At post-molar follow-up, a gestational trophoblastic tumor (GTT) was diagnosed and promptly treated with chemotherapy. Association between CHM and eclampsia requires immediate uterine evacuation and strict post-molar follow-up, due to increased risk of GTT development.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(6):445-448
DOI 10.1590/S0100-72032003000600010
Development of preeclampsia/eclampsia prior to 20 weeks of pregnancy should raise the suspicion of hydatidiform mole. We report a case of complete hydatidiform mole (CHM) concurrent with eclampsia in a 20-year-old patient with vaginal bleeding, anemia, large uterine size, and ovary cysts associated with hypertension and proteinuria. Plasmatic b-hCG levels were high and there was abnormal thyroid function. The ultrasonographic findings were compatible with CHM. After uterine evacuation, the patient had headache and visual alterations, followed by tonic-clonic seizures, which ceased with the administration of 50% magnesium sulfate. At post-molar follow-up, a gestational trophoblastic tumor (GTT) was diagnosed and promptly treated with chemotherapy. Association between CHM and eclampsia requires immediate uterine evacuation and strict post-molar follow-up, due to increased risk of GTT development.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):61-65
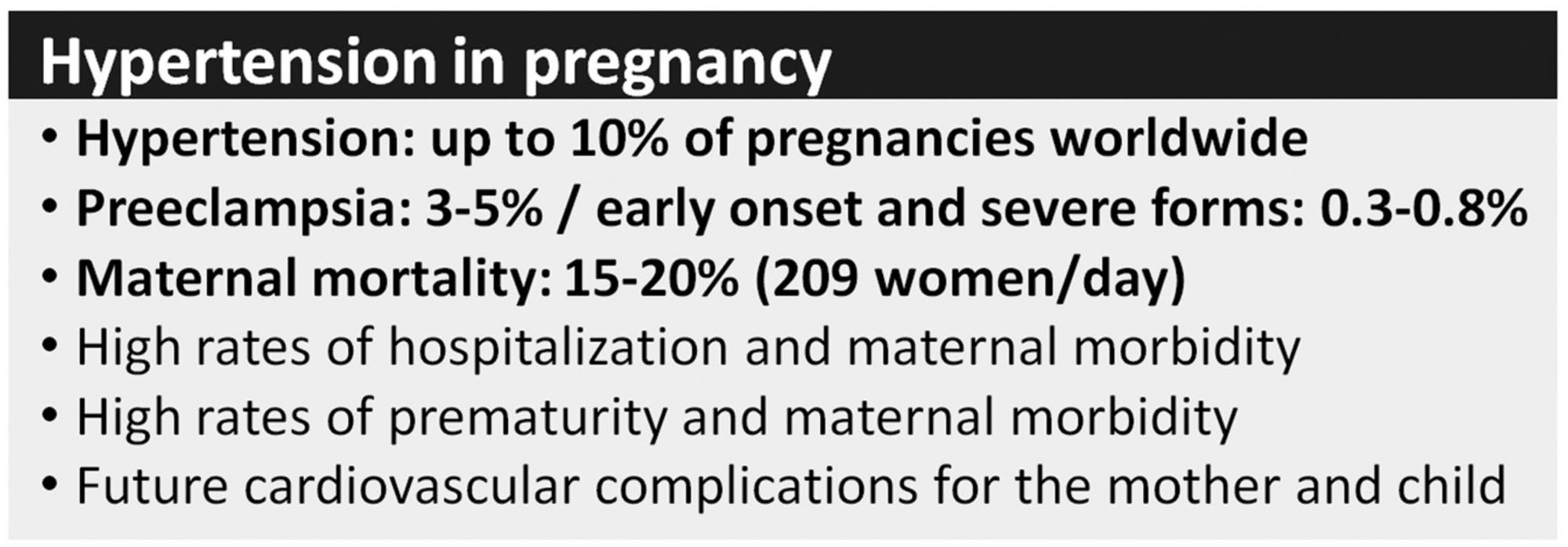
Pre-eclampsia (PE) is a severe disorder that affects up to 8% of all pregnancies and represents an important cause of maternal and perinatal morbidity and mortality. The screening of the disease is a subject of studies, but the complexity and uncertainties regarding its etiology make this objective a difficult task. In addition, the costs related to screening protocols, the heterogeneity of the most affected populations and the lack of highly effective prevention methods reduce the potential of current available algorithms for screening. Thus, the National Specialized Commission of Hypertension in Pregnancy of the Brazilian Association of Gynecology and Obstetrics Federation (Febrasgo, in the Portuguese acronym) (NSC Hypertension in Pregnancy of the Febrasgo) considers that there are no screening algorithms to be implemented in the country to date and advocates that Aspirin and calcium should be widely used.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):61-65
Pre-eclampsia (PE) is a severe disorder that affects up to 8% of all pregnancies and represents an important cause of maternal and perinatal morbidity and mortality. The screening of the disease is a subject of studies, but the complexity and uncertainties regarding its etiology make this objective a difficult task. In addition, the costs related to screening protocols, the heterogeneity of the most affected populations and the lack of highly effective prevention methods reduce the potential of current available algorithms for screening. Thus, the National Specialized Commission of Hypertension in Pregnancy of the Brazilian Association of Gynecology and Obstetrics Federation (Febrasgo, in the Portuguese acronym) (NSC Hypertension in Pregnancy of the Febrasgo) considers that there are no screening algorithms to be implemented in the country to date and advocates that Aspirin and calcium should be widely used.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(10):627-634
DOI 10.1590/S0100-72032005001000010
Arterial hypertension is one of the most frequent causes of maternal death. The most important types found in pregnancy are gestational hypertension, clinically defined by increased arterial pressure after the 20th week of pregnancy, and preeclampsia associated with proteinuria. In the initial phase, the disease is asymptomatic, but when not treated or when the pregnancy is not interrupted, it naturally progresses to serious forms such as eclampsia and HELLP syndrome. Eclampsia is defined by one or more generalized tonic-clonic seizures or coma in a pregnant woman with gestational hypertension or preeclampsia, and without neurological disease. It may occur during pregnancy, labor, and immediately after delivery. It is often preceded by signs and symptoms of imminent eclampsia (central nervous system, visual and gastric disorders). Its association with hemolysis, low platelet count, and hepatic dysfunction had already been reported in the literature of the 1950's. In 1982, Weinstein grouped these alterations as a syndrome under the acronym of HELLP, meaning hemolysis (H), elevated liver enzyme levels (EL), and low platelet (LP) count. The literature differs in relation to the parameter values that define the syndrome. Sibai et al. (1986) proposed a system of laboratory and biochemical diagnosis standards which has been adopted by the Brazilian Health Ministry. Clinical manifestations are sometimes imprecise; common complaints are epigastric pain, general malaise, loss of appetite, nausea, and vomiting. Early diagnosis is exclusively by laboratory tests and should be systematically investigated in women with serious preeclampsia/eclampsia or pain in the superior right abdominal quadrant. Differentiating HELLP syndrome from others with similar clinical or laboratory manifestations is not easy. Differential diagnosis is particularly difficult regarding diseases such as thrombotic thrombocytopenic purpura, hemolytic-uremic syndrome, or acute fatty liver of pregnancy, due to poor clinical history, and similar physiopathological aspects. An understanding of preeclampsia physiopathology, early diagnosis, and precise action at the right moment in situations complicated by eclampsia or HELLP syndrome, allows a better maternal and perinatal prognosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(10):627-634
DOI 10.1590/S0100-72032005001000010
Arterial hypertension is one of the most frequent causes of maternal death. The most important types found in pregnancy are gestational hypertension, clinically defined by increased arterial pressure after the 20th week of pregnancy, and preeclampsia associated with proteinuria. In the initial phase, the disease is asymptomatic, but when not treated or when the pregnancy is not interrupted, it naturally progresses to serious forms such as eclampsia and HELLP syndrome. Eclampsia is defined by one or more generalized tonic-clonic seizures or coma in a pregnant woman with gestational hypertension or preeclampsia, and without neurological disease. It may occur during pregnancy, labor, and immediately after delivery. It is often preceded by signs and symptoms of imminent eclampsia (central nervous system, visual and gastric disorders). Its association with hemolysis, low platelet count, and hepatic dysfunction had already been reported in the literature of the 1950's. In 1982, Weinstein grouped these alterations as a syndrome under the acronym of HELLP, meaning hemolysis (H), elevated liver enzyme levels (EL), and low platelet (LP) count. The literature differs in relation to the parameter values that define the syndrome. Sibai et al. (1986) proposed a system of laboratory and biochemical diagnosis standards which has been adopted by the Brazilian Health Ministry. Clinical manifestations are sometimes imprecise; common complaints are epigastric pain, general malaise, loss of appetite, nausea, and vomiting. Early diagnosis is exclusively by laboratory tests and should be systematically investigated in women with serious preeclampsia/eclampsia or pain in the superior right abdominal quadrant. Differentiating HELLP syndrome from others with similar clinical or laboratory manifestations is not easy. Differential diagnosis is particularly difficult regarding diseases such as thrombotic thrombocytopenic purpura, hemolytic-uremic syndrome, or acute fatty liver of pregnancy, due to poor clinical history, and similar physiopathological aspects. An understanding of preeclampsia physiopathology, early diagnosis, and precise action at the right moment in situations complicated by eclampsia or HELLP syndrome, allows a better maternal and perinatal prognosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(9):669-675
Preeclampsia (PE) is a pregnancy-specific syndrome characterized by abnormal levels of cytokines and angiogenic factors, playing a role in the disease development. The present study evaluated whether immunological markers are associated with the gestational age and with the disease severity in preeclamptic women.
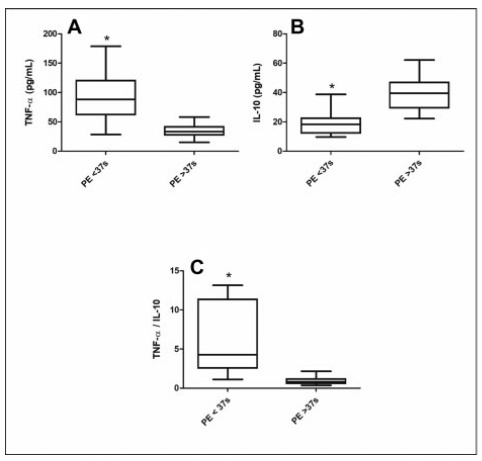
Ninety-five women who developed PE were stratified for gestational age as preterm PE (< 37 weeks) and term PE (≥ 37 weeks of gestation) and compared for disease severity as well as plasma concentration of angiogenic factors and cytokines. The concentrations of placental growth factor (PlGF), vascular endothelial growth factor (VEGF), Fms-like soluble tyrosine kinase (sFlt-1) and soluble endoglin (sEng), as well as the cytokines, tumor necrosis factor-α (TNF-α) and interleukin 10 (IL-10), were determined by enzyme-linked immunosorbent assay (ELISA).
The comparison between preeclamptic groups showed a higher percentage of severe cases in preterm PE (82.1%) than in term PE (35.9%). Similarly, the concentrations of TNF-α, sFlt-1, and sEng, as well as TNF-α/IL-10 and sFlt-1/PlGF ratios were significantly higher in the preterm PE group. In contrast, concentrations of PlGF, VEGF, and IL-10 were significantly lower in women with preterm PE. Negative correlations between TNF-α and IL-10 (r = 0.5232) and between PlGF and sFlt1 (r = 0.4158) were detected in the preterm PE.
In pregnant women with preterm PE, there is an imbalance between immunological markers, with the predominance of anti-angiogenic factors and TNF-α, associated with adverse maternal clinical outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(9):669-675
Preeclampsia (PE) is a pregnancy-specific syndrome characterized by abnormal levels of cytokines and angiogenic factors, playing a role in the disease development. The present study evaluated whether immunological markers are associated with the gestational age and with the disease severity in preeclamptic women.
Ninety-five women who developed PE were stratified for gestational age as preterm PE (< 37 weeks) and term PE (≥ 37 weeks of gestation) and compared for disease severity as well as plasma concentration of angiogenic factors and cytokines. The concentrations of placental growth factor (PlGF), vascular endothelial growth factor (VEGF), Fms-like soluble tyrosine kinase (sFlt-1) and soluble endoglin (sEng), as well as the cytokines, tumor necrosis factor-α (TNF-α) and interleukin 10 (IL-10), were determined by enzyme-linked immunosorbent assay (ELISA).
The comparison between preeclamptic groups showed a higher percentage of severe cases in preterm PE (82.1%) than in term PE (35.9%). Similarly, the concentrations of TNF-α, sFlt-1, and sEng, as well as TNF-α/IL-10 and sFlt-1/PlGF ratios were significantly higher in the preterm PE group. In contrast, concentrations of PlGF, VEGF, and IL-10 were significantly lower in women with preterm PE. Negative correlations between TNF-α and IL-10 (r = 0.5232) and between PlGF and sFlt1 (r = 0.4158) were detected in the preterm PE.
In pregnant women with preterm PE, there is an imbalance between immunological markers, with the predominance of anti-angiogenic factors and TNF-α, associated with adverse maternal clinical outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):878-883
It is a challenge to consider preeclampsia (PE) diagnosis and management in low and middle-income settings, where it represents a major public health concern. The placenta is the underlying cause of disease, and the plasma concentrations of proangiogenic and antiangiogenic factors released by the placenta can reflect the risks of disease progression. Antiangiogenic proteins, such as soluble fms-like tyrosine kinase 1 (sFlt-1), and proangiogenic, like placental growth factors (PlGF), are directly and inversely correlated with the disease onset, respectively.
Narrative review on the use of biomarkers (sFlt-1 to PlGF ratio) with a suggested guidance protocol.
Key considerations on the use of biomarkers: the sFlt-1/PlGF ratio is mainly relevant to rule out PE between 20 and 36 6/7 weeks in cases of suspected PE; however, it should not replace the routine exams for the diagnosis of PE. The sFlt-1/PlGF ratio should not be performed after confirmed PE diagnosis (only in research settings). In women with suspected PE, sFlt-1/PlGF ratio < 38 can rule out the diagnosis of PE for 1 week (VPN = 99.3) and up to 4 weeks (VPN= 94.3); sFlt-1/PlGF ratio > 38 does not confirm the diagnosis of PE; however, it can assist clinical management. In cases of severe hypertension and/or symptoms (imminent eclampsia), hospitalization is imperative, regardless of the result of the sFlt-1/PlGF ratio.
The use of biomarkers can help support clinical decisions on the management of suspected PE cases, especially to rule out PE diagnosis, thus avoiding unnecessary interventions, especially hospitalizations and elective prematurity
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):878-883
It is a challenge to consider preeclampsia (PE) diagnosis and management in low and middle-income settings, where it represents a major public health concern. The placenta is the underlying cause of disease, and the plasma concentrations of proangiogenic and antiangiogenic factors released by the placenta can reflect the risks of disease progression. Antiangiogenic proteins, such as soluble fms-like tyrosine kinase 1 (sFlt-1), and proangiogenic, like placental growth factors (PlGF), are directly and inversely correlated with the disease onset, respectively.
Narrative review on the use of biomarkers (sFlt-1 to PlGF ratio) with a suggested guidance protocol.
Key considerations on the use of biomarkers: the sFlt-1/PlGF ratio is mainly relevant to rule out PE between 20 and 36 6/7 weeks in cases of suspected PE; however, it should not replace the routine exams for the diagnosis of PE. The sFlt-1/PlGF ratio should not be performed after confirmed PE diagnosis (only in research settings). In women with suspected PE, sFlt-1/PlGF ratio < 38 can rule out the diagnosis of PE for 1 week (VPN = 99.3) and up to 4 weeks (VPN= 94.3); sFlt-1/PlGF ratio > 38 does not confirm the diagnosis of PE; however, it can assist clinical management. In cases of severe hypertension and/or symptoms (imminent eclampsia), hospitalization is imperative, regardless of the result of the sFlt-1/PlGF ratio.
The use of biomarkers can help support clinical decisions on the management of suspected PE cases, especially to rule out PE diagnosis, thus avoiding unnecessary interventions, especially hospitalizations and elective prematurity
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(2):91-98
DOI 10.1590/S0100-72031999000200006
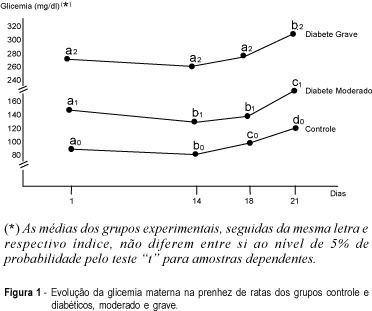
Purpose: placental alterations were evaluated in macrosomatia and fetal growth retardation in pregnancy complicated by diabetes. Three groups of rats, used as experimental models, were studied: control, moderate and severe diabetes. Material and Method: cesarian sections were carried out on the 18th or 21st day of pregnancy. Maternal and fetal glycemia, newborn weight, placental weight, relationship between placental and fetal weight, DNA, RNA and protein contents and the glycogen deposited on placental membranes were analyzed. Results: there was a higher number of macrosomic newborns in the moderate diabetes group, whose placentas were rich in DNA with progressive decrease of glycogen in their membranes towards the end of pregnancy. There was a predominance of small for date newborns in the severe diabetes group. Their placentas showed a small DNA proportion, an increase in RNA synthesis and a tendency to higher protein production, with no change in the glycogen deposit. Conclusions: we conclude that fetal growth deviation in moderate and severe maternal diabetes between the 18th and 21st days of pregnancy is related to several placental alterations. In the moderate form there were only cellular hyperplasia and disappearance of placental glycogen at the end of pregnancy. In the severe diabetes group there was thickening of maternal-fetal membranes during this period. There was cellular hyperplasia and hypertrophy associated with the maintenance of glycogen reserves in the placental membranes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(2):91-98
DOI 10.1590/S0100-72031999000200006
Purpose: placental alterations were evaluated in macrosomatia and fetal growth retardation in pregnancy complicated by diabetes. Three groups of rats, used as experimental models, were studied: control, moderate and severe diabetes. Material and Method: cesarian sections were carried out on the 18th or 21st day of pregnancy. Maternal and fetal glycemia, newborn weight, placental weight, relationship between placental and fetal weight, DNA, RNA and protein contents and the glycogen deposited on placental membranes were analyzed. Results: there was a higher number of macrosomic newborns in the moderate diabetes group, whose placentas were rich in DNA with progressive decrease of glycogen in their membranes towards the end of pregnancy. There was a predominance of small for date newborns in the severe diabetes group. Their placentas showed a small DNA proportion, an increase in RNA synthesis and a tendency to higher protein production, with no change in the glycogen deposit. Conclusions: we conclude that fetal growth deviation in moderate and severe maternal diabetes between the 18th and 21st days of pregnancy is related to several placental alterations. In the moderate form there were only cellular hyperplasia and disappearance of placental glycogen at the end of pregnancy. In the severe diabetes group there was thickening of maternal-fetal membranes during this period. There was cellular hyperplasia and hypertrophy associated with the maintenance of glycogen reserves in the placental membranes.