Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):304-309
DOI 10.1590/S0100-72032012000700003
PURPOSE: To evaluate the impact of body mass index (BMI) at the beginning of pregnancy and weight gain on pregnancy outcome so that this measure can be implemented and valued by prenatal care health services. METHOD: Cross-sectional population-based study of all births in the only two hospitals in Rio Grande city (Brazil), in 2007. Among the 2,557 mothers interviewed, it was possible to calculate BMI in only 1,117. The Stata 11 software was used for data analysis. Logist regression was applied to the outomes involving diabetes mellitus, premature labor and cesarean section. Regarding birth weight, data were adjusted by multinomial logistic regression using as base category the group of 2,500 to 4,000 g. The level of significance was set at p-value <0.05 in a two-tailed test. RESULTS: There was no increased risk of hypertension or diabetes in patients in the different groups of BMI and weight gain. The risk of preterm delivery was evident in the group with a weight gain ≤8 kg (p<0.05). Regarding the route of delivery, it was observed that the higher the BMI in early pregnancy (p=0.001) and the greater the weight gain during pregnancy (p=0.004), the greater the risk of surgical delivery, which reached 11% in the group of obese mothers (p=0.004) and 12% in the group with a weight gain ≥17 kg (p=0.001). The weight of the newborns was influenced by BMI and weight gain, and the higher the BMI in early pregnancy and the gestational weight gain, the greater the risk of macrosomia. CONCLUSION: The monitoring of BMI and weight gain during pregnancy is a low cost and useful procedure for the establishment of nutritional interventions aimed at reducing maternal and fetal risks.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):304-309
DOI 10.1590/S0100-72032012000700003
PURPOSE: To evaluate the impact of body mass index (BMI) at the beginning of pregnancy and weight gain on pregnancy outcome so that this measure can be implemented and valued by prenatal care health services. METHOD: Cross-sectional population-based study of all births in the only two hospitals in Rio Grande city (Brazil), in 2007. Among the 2,557 mothers interviewed, it was possible to calculate BMI in only 1,117. The Stata 11 software was used for data analysis. Logist regression was applied to the outomes involving diabetes mellitus, premature labor and cesarean section. Regarding birth weight, data were adjusted by multinomial logistic regression using as base category the group of 2,500 to 4,000 g. The level of significance was set at p-value <0.05 in a two-tailed test. RESULTS: There was no increased risk of hypertension or diabetes in patients in the different groups of BMI and weight gain. The risk of preterm delivery was evident in the group with a weight gain ≤8 kg (p<0.05). Regarding the route of delivery, it was observed that the higher the BMI in early pregnancy (p=0.001) and the greater the weight gain during pregnancy (p=0.004), the greater the risk of surgical delivery, which reached 11% in the group of obese mothers (p=0.004) and 12% in the group with a weight gain ≥17 kg (p=0.001). The weight of the newborns was influenced by BMI and weight gain, and the higher the BMI in early pregnancy and the gestational weight gain, the greater the risk of macrosomia. CONCLUSION: The monitoring of BMI and weight gain during pregnancy is a low cost and useful procedure for the establishment of nutritional interventions aimed at reducing maternal and fetal risks.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):304-310
To review data on the use of corticosteroids for the treatment of fetuses with high-risk congenital pulmonary adenomatoid malformation (CPAM).
Integrative review based on the literature available onMEDLINE and LILACS, including articles published until November, 2020.
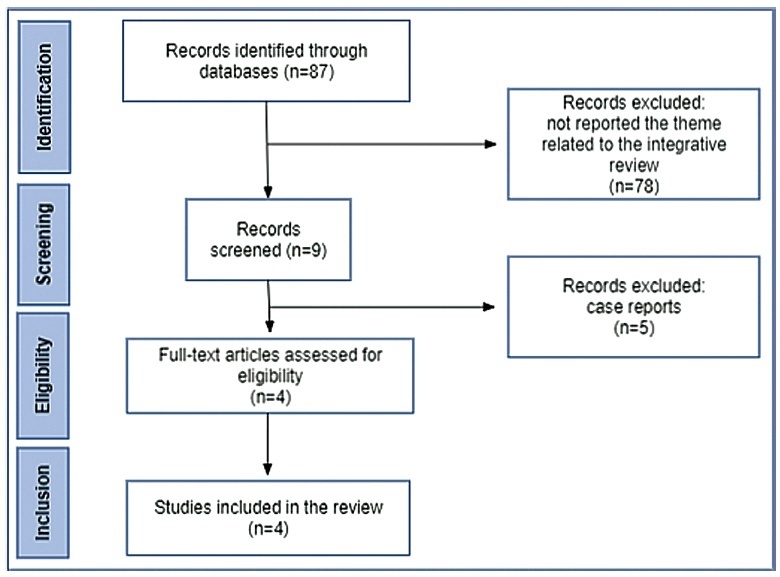
The initial search resulted in 87 articles, 4 of which were selected for analysis, with all of them being retrospective descriptive observational studies. In the group of fetuses that received only a single corticosteroid cycle, the hydrops resolution rate was 70%, and the survival rate was 83.8%. In fetuses treated with 2 or more cycles of corticosteroids, there was an improvement in the condition of hydrops or edema in a single body compartment in 47%, and survival of 81.8% of the fetuses.
The use of corticosteroids for the prenatal treatment of high-risk CPAM appears to be associated with an improvement in perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(3):304-310
To review data on the use of corticosteroids for the treatment of fetuses with high-risk congenital pulmonary adenomatoid malformation (CPAM).
Integrative review based on the literature available onMEDLINE and LILACS, including articles published until November, 2020.
The initial search resulted in 87 articles, 4 of which were selected for analysis, with all of them being retrospective descriptive observational studies. In the group of fetuses that received only a single corticosteroid cycle, the hydrops resolution rate was 70%, and the survival rate was 83.8%. In fetuses treated with 2 or more cycles of corticosteroids, there was an improvement in the condition of hydrops or edema in a single body compartment in 47%, and survival of 81.8% of the fetuses.
The use of corticosteroids for the prenatal treatment of high-risk CPAM appears to be associated with an improvement in perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(6):305-309
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(6):305-309
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(6):305-308
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(6):305-308
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(10):305-309
DOI 10.1590/S0100-72032011001000006
PURPOSE: to investigate the micronucleation (MN) of exfoliated cells from the uterine cervix of HIV+ women according to immunocompetence status. We investigated the clinical conditions of immunocompetence by analyzing the levels of CD4+ lymphocytes and viral count for HIV (VC). METHODS: biological material was collected from 23 HIV+ patients whose cervical oncologic cytology results were negative. They were patients from the STD/AIDS-FCMS-PUCSP who underwent a cytobrush collection in the squamous columnar junction. Similar material was obtained from 19 healthy control women. The material, about 2000 cells per patient, was processed for cytology using light microscopy and an immersion objective. To analyze the immunological status of HIV+ patients we used CD4+ count and VC. Statistical analysis was performed using the Χ2 and Kolmorogov-Smirnov tests. RESULTS: twenty-three pacients composed the group of HIV+ women and 19 composed the control group. We found micronuclei (MN) in all HIV+ patients and in 84.2% of the control group. In 17 73.9% of the HIV+ patients and in 5.2% of the control group we found more than 7 MN cells. MN tended to occur more among women with poorer immunological status in the HIV+ group. CONCLUSIONS: HIV+ patients in the AIDS phase have a higher prevalence of micronucleated cells, as opposed to a control group. Also, the frequency of MN was associated with worse conditions of immunosuppression.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(10):305-309
DOI 10.1590/S0100-72032011001000006
PURPOSE: to investigate the micronucleation (MN) of exfoliated cells from the uterine cervix of HIV+ women according to immunocompetence status. We investigated the clinical conditions of immunocompetence by analyzing the levels of CD4+ lymphocytes and viral count for HIV (VC). METHODS: biological material was collected from 23 HIV+ patients whose cervical oncologic cytology results were negative. They were patients from the STD/AIDS-FCMS-PUCSP who underwent a cytobrush collection in the squamous columnar junction. Similar material was obtained from 19 healthy control women. The material, about 2000 cells per patient, was processed for cytology using light microscopy and an immersion objective. To analyze the immunological status of HIV+ patients we used CD4+ count and VC. Statistical analysis was performed using the Χ2 and Kolmorogov-Smirnov tests. RESULTS: twenty-three pacients composed the group of HIV+ women and 19 composed the control group. We found micronuclei (MN) in all HIV+ patients and in 84.2% of the control group. In 17 73.9% of the HIV+ patients and in 5.2% of the control group we found more than 7 MN cells. MN tended to occur more among women with poorer immunological status in the HIV+ group. CONCLUSIONS: HIV+ patients in the AIDS phase have a higher prevalence of micronucleated cells, as opposed to a control group. Also, the frequency of MN was associated with worse conditions of immunosuppression.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(6):305-310
DOI 10.1590/S0100-72032009000600007
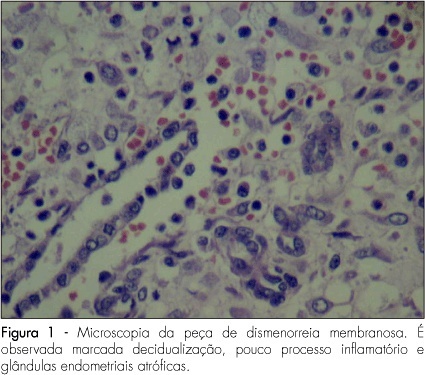
PURPOSE: to present a series of cases of membranous dysmenorrhea. METHODS: all the patients selected were under diagnostic suspicion, after being clinically attended in a private medical office due to the report of painful dysmenorrhea associated with spontaneous elimination of elastic material with uterine shape. Only relevant facts about the pain condition have been described, together with the present and previous medical history and life habits. The material eliminated was forwarded to the pathology laboratory, where the macro and microscopic analyses were done. Cases with no confirmation of membranous material elimination were not selected. After the diagnostic confirmation, literature up to 2008 was carried out using the MeSH method, with the words "membranous dysmenorrheal". RESULTS: three cases of dysmenorrhea were transcribed. Besides the characteristic picture of pain and vaginal elimination of elastic material, all the cases were associated with the use of hormonal contraceptive methods. CONCLUSIONS: despite the fact that there are only sporadic reports of cases of membranous dysmenorrhea in the scientific literature, this etiology must be considered in cases of pain associated with vaginal bleeding plus elimination of elastic or solid material. The final diagnosis depends on anatomopathological exam, which should not be dismissed. We highlight the need for more discussion about this pathology, to keep the professionals updated with the aim of exerting adequate diagnosis and therapeutics.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(6):305-310
DOI 10.1590/S0100-72032009000600007
PURPOSE: to present a series of cases of membranous dysmenorrhea. METHODS: all the patients selected were under diagnostic suspicion, after being clinically attended in a private medical office due to the report of painful dysmenorrhea associated with spontaneous elimination of elastic material with uterine shape. Only relevant facts about the pain condition have been described, together with the present and previous medical history and life habits. The material eliminated was forwarded to the pathology laboratory, where the macro and microscopic analyses were done. Cases with no confirmation of membranous material elimination were not selected. After the diagnostic confirmation, literature up to 2008 was carried out using the MeSH method, with the words "membranous dysmenorrheal". RESULTS: three cases of dysmenorrhea were transcribed. Besides the characteristic picture of pain and vaginal elimination of elastic material, all the cases were associated with the use of hormonal contraceptive methods. CONCLUSIONS: despite the fact that there are only sporadic reports of cases of membranous dysmenorrhea in the scientific literature, this etiology must be considered in cases of pain associated with vaginal bleeding plus elimination of elastic or solid material. The final diagnosis depends on anatomopathological exam, which should not be dismissed. We highlight the need for more discussion about this pathology, to keep the professionals updated with the aim of exerting adequate diagnosis and therapeutics.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(4):305-309
DOI 10.1590/S0100-72032004000400007
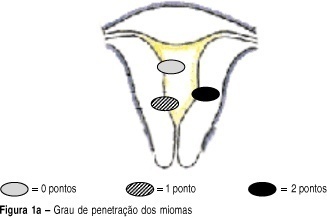
OBJECTIVE: to develop a new preoperative classification of submucous myomas to evaluate the viability and the degree of difficulty of hysteroscopic myomectomy. METHODS: forty-four patients were submitted to hysteroscopic resection of submucous myomas. The possibility of total resection of the myoma, the surgery duration, the fluid deficit, and the incidence of complications were evaluated. The myomas were classified by the Classification of the European Society of Endoscopic Surgery (CESES) and by the classification proposed (CP) by our group, that besides the degree of penetration of the myoma in the myometrium, adds the parameters: extent of the base of the myoma as related to the uterine wall, the size of the myoma in centimeters and its topography at the uterine cavity. For statistical analysis the Fisher test, the Student t test and the analysis of variance were used. Statistic significance was considered when the p-value was smaller than 0.05 in the bicaudal test. RESULTS: in 47 myomas the hysteroscopic surgery was considered complete. There was no significant difference among the three levels (0, 1 and 2) by CESES. By CP, the difference among the number of complete surgeries was significant (p=0.001) between the two levels (groups I and II). The difference between the surgery duration was significant when the two classifications were compared. In relation to the fluid deficit, just CP presented significant differences among the levels (p=0,02). CONCLUSIONS: the proposed classification includes more clues about the difficulties of the hysteroscopic myomectomy than the standard classification. It should be noted that the number of hysteroscopic myomectomies used for that analysis was modest, being interesting to evaluate the performance of the proposed classification in larger series of cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(4):305-309
DOI 10.1590/S0100-72032004000400007
OBJECTIVE: to develop a new preoperative classification of submucous myomas to evaluate the viability and the degree of difficulty of hysteroscopic myomectomy. METHODS: forty-four patients were submitted to hysteroscopic resection of submucous myomas. The possibility of total resection of the myoma, the surgery duration, the fluid deficit, and the incidence of complications were evaluated. The myomas were classified by the Classification of the European Society of Endoscopic Surgery (CESES) and by the classification proposed (CP) by our group, that besides the degree of penetration of the myoma in the myometrium, adds the parameters: extent of the base of the myoma as related to the uterine wall, the size of the myoma in centimeters and its topography at the uterine cavity. For statistical analysis the Fisher test, the Student t test and the analysis of variance were used. Statistic significance was considered when the p-value was smaller than 0.05 in the bicaudal test. RESULTS: in 47 myomas the hysteroscopic surgery was considered complete. There was no significant difference among the three levels (0, 1 and 2) by CESES. By CP, the difference among the number of complete surgeries was significant (p=0.001) between the two levels (groups I and II). The difference between the surgery duration was significant when the two classifications were compared. In relation to the fluid deficit, just CP presented significant differences among the levels (p=0,02). CONCLUSIONS: the proposed classification includes more clues about the difficulties of the hysteroscopic myomectomy than the standard classification. It should be noted that the number of hysteroscopic myomectomies used for that analysis was modest, being interesting to evaluate the performance of the proposed classification in larger series of cases.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(6):306-311
DOI 10.1590/S0100-72032008000600007
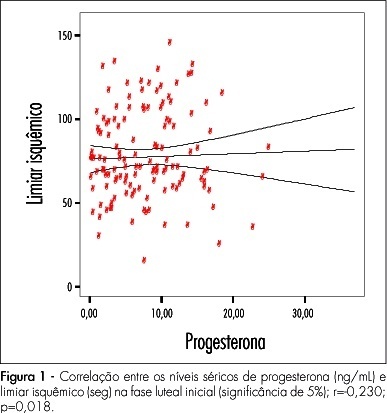
PURPOSE: to investigate the relationship between pain perception (experimental pain threshold and tolerance, in response to ischemia and pressure) in young and healthy young women and female sexual hormone seric levels (estradiol and progesterone). METHODS: 18 volunteers have participated of this study, during three consecutive menstrual cycles. A pressure algometer and a manual dynamometer have been used to measure painful responses to pressure and ischemia algesic stimuli. Blood has been collected for assessment of both hormonal and painful variables, during three menstrual cycles, whose characterization was based on daily oral temperature record, a diary of the menstrual cycles with the onset and end of each cycle, and on estradiol and progesterone plasmatic levels. The average for the algesic variables measured has been compared by analysis of variance (ANOVA) and the Tukey-Kramer's post-test, among the menstrual cycle phases (follicular, periovulatory, early luteal, late luteal and menstrual). The Pearson's test has been used for correlation analysis between algesic and hormonal variables. Statistical significance has been defined as p<0.05. RESULTS: no significant change in pain parameters among the menstrual cycle phases has been observed. Nevertheless, there have been significant negative correlations between progesterone and ischemic threshold (r=-0.23; p<0.01), and pressure tolerance (r=-0.23; p<0.01) at the early luteal phase. CONCLUSIONS: these results indicate that the increase in progesterone levels correlates with a decrease of ischemic threshold and pressure tolerance, suggesting that progesterone plays a role in the pain modulation during the early luteal phase.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(6):306-311
DOI 10.1590/S0100-72032008000600007
PURPOSE: to investigate the relationship between pain perception (experimental pain threshold and tolerance, in response to ischemia and pressure) in young and healthy young women and female sexual hormone seric levels (estradiol and progesterone). METHODS: 18 volunteers have participated of this study, during three consecutive menstrual cycles. A pressure algometer and a manual dynamometer have been used to measure painful responses to pressure and ischemia algesic stimuli. Blood has been collected for assessment of both hormonal and painful variables, during three menstrual cycles, whose characterization was based on daily oral temperature record, a diary of the menstrual cycles with the onset and end of each cycle, and on estradiol and progesterone plasmatic levels. The average for the algesic variables measured has been compared by analysis of variance (ANOVA) and the Tukey-Kramer's post-test, among the menstrual cycle phases (follicular, periovulatory, early luteal, late luteal and menstrual). The Pearson's test has been used for correlation analysis between algesic and hormonal variables. Statistical significance has been defined as p<0.05. RESULTS: no significant change in pain parameters among the menstrual cycle phases has been observed. Nevertheless, there have been significant negative correlations between progesterone and ischemic threshold (r=-0.23; p<0.01), and pressure tolerance (r=-0.23; p<0.01) at the early luteal phase. CONCLUSIONS: these results indicate that the increase in progesterone levels correlates with a decrease of ischemic threshold and pressure tolerance, suggesting that progesterone plays a role in the pain modulation during the early luteal phase.