You searched for:"Melania Maria Ramos de Amorim"
We found (25) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 06-27-2024;46:e-rbgo47
In Brazil, postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality. Data on the profile of women and risk factors associated with PPH are sparse. This study aimed to describe the profile and management of patients with PPH, and the association of risk factors for PPH with severe maternal outcomes (SMO).
A cross-sectional study was conducted in Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) obstetric intensive care unit (ICU) between January 2012 and March 2020, including patients who gave birth at the hospital and that were admitted with PPH to the ICU.
The study included 358 patients, of whom 245 (68.4%) delivered in the IMIP maternity, and 113 (31.6%) in other maternity. The mean age of the patients was 26.7 years, with up to eight years of education (46.1%) and a mean of six prenatal care. Uterine atony (72.9%) was the most common cause, 1.6% estimated blood loss, 2% calculated shock index (SI), 63.9% of patients received hemotransfusion, and 27% underwent hysterectomy. 136 cases of SMO were identified, 35.5% were classified as maternal near miss and 3.0% maternal deaths. Multiparity was associated with SMO as an antepartum risk factor (RR=1.83, 95% CI1.42-2.36). Regarding intrapartum risk factors, abruptio placentae abruption was associated with SMO (RR=2.2 95% CI1.75-2.81). Among those who had hypertension (49.6%) there was a lower risk of developing SMO.
The principal factors associated with poor maternal outcome were being multiparous and placental abruption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 06-27-2024;46:e-rbgo47
In Brazil, postpartum hemorrhage (PPH) is a major cause of maternal morbidity and mortality. Data on the profile of women and risk factors associated with PPH are sparse. This study aimed to describe the profile and management of patients with PPH, and the association of risk factors for PPH with severe maternal outcomes (SMO).
A cross-sectional study was conducted in Instituto de Medicina Integral Prof. Fernando Figueira (IMIP) obstetric intensive care unit (ICU) between January 2012 and March 2020, including patients who gave birth at the hospital and that were admitted with PPH to the ICU.
The study included 358 patients, of whom 245 (68.4%) delivered in the IMIP maternity, and 113 (31.6%) in other maternity. The mean age of the patients was 26.7 years, with up to eight years of education (46.1%) and a mean of six prenatal care. Uterine atony (72.9%) was the most common cause, 1.6% estimated blood loss, 2% calculated shock index (SI), 63.9% of patients received hemotransfusion, and 27% underwent hysterectomy. 136 cases of SMO were identified, 35.5% were classified as maternal near miss and 3.0% maternal deaths. Multiparity was associated with SMO as an antepartum risk factor (RR=1.83, 95% CI1.42-2.36). Regarding intrapartum risk factors, abruptio placentae abruption was associated with SMO (RR=2.2 95% CI1.75-2.81). Among those who had hypertension (49.6%) there was a lower risk of developing SMO.
The principal factors associated with poor maternal outcome were being multiparous and placental abruption.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 07-01-2016;38(7):325-332
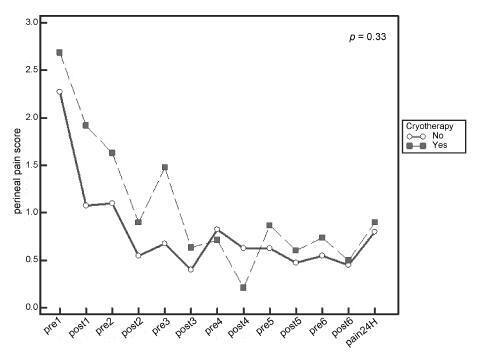
Systematic reviews that evaluate the perineal cryotherapy to reduce pain in the vaginal postpartum are inconclusive.
To evaluate clinical effectiveness of cryotherapy in the management of humanized postpartum perineal pain and vaginal edema.
A double-bind randomized controlled clinical trial (UTN number: U1111- 1131-8433) was conducted in a hospital in Northeastern, Brazil.Women were included following humanized childbirth. All had vaginal deliveries of a single, full-term pregnancy with cephalic presentation. Exclusion criteria included previous perineal lesion, episiotomy during the current delivery, instrumental delivery, uterine curettage and postpartum hemorrhage. In the experimental group, an ice pack was applied six times on the perineum for 20 minutes, reducing the temperature between 10 and 15° C, then 60 minutes without exposure to cold. In the non-cryotherapy, a water bag unable to reduce the temperature to this extent was used, compliance with the same application protocol of the first group. Perineal temperature wasmonitored at zero, 10 and 20 minutes for application in both groups. Evaluations were made immediately before and after the applications and 24 hours after delivery spontaneous, to determine the association between variables.
A total of 80 women were included in the study, 40 in each group. There was no significant difference in scores of perineal pain and edema between the groups with or without cryotherapy until 24 hours after childbirth. There was no difference between groups when accomplished repeated measures analysis over the 24 hours after delivery, considering the median perineal pain (p = 0.3) and edema (p = 0.9). Perineal cryotherapy did not influence the amount of analgesics used (p = 0.07) and no adverse effect was registered.
The use of cryotherapy following normal vaginal delivery within the concept of humanized minimally interventionist childbirth had no effect on perineal pain and edema, since it was already substantially lower, nor the need for pain medicaments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 07-01-2016;38(7):325-332
Systematic reviews that evaluate the perineal cryotherapy to reduce pain in the vaginal postpartum are inconclusive.
To evaluate clinical effectiveness of cryotherapy in the management of humanized postpartum perineal pain and vaginal edema.
A double-bind randomized controlled clinical trial (UTN number: U1111- 1131-8433) was conducted in a hospital in Northeastern, Brazil.Women were included following humanized childbirth. All had vaginal deliveries of a single, full-term pregnancy with cephalic presentation. Exclusion criteria included previous perineal lesion, episiotomy during the current delivery, instrumental delivery, uterine curettage and postpartum hemorrhage. In the experimental group, an ice pack was applied six times on the perineum for 20 minutes, reducing the temperature between 10 and 15° C, then 60 minutes without exposure to cold. In the non-cryotherapy, a water bag unable to reduce the temperature to this extent was used, compliance with the same application protocol of the first group. Perineal temperature wasmonitored at zero, 10 and 20 minutes for application in both groups. Evaluations were made immediately before and after the applications and 24 hours after delivery spontaneous, to determine the association between variables.
A total of 80 women were included in the study, 40 in each group. There was no significant difference in scores of perineal pain and edema between the groups with or without cryotherapy until 24 hours after childbirth. There was no difference between groups when accomplished repeated measures analysis over the 24 hours after delivery, considering the median perineal pain (p = 0.3) and edema (p = 0.9). Perineal cryotherapy did not influence the amount of analgesics used (p = 0.07) and no adverse effect was registered.
The use of cryotherapy following normal vaginal delivery within the concept of humanized minimally interventionist childbirth had no effect on perineal pain and edema, since it was already substantially lower, nor the need for pain medicaments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 01-23-2012;33(11):361-366
DOI 10.1590/S0100-72032011001100007
PURPOSE: to compare the accuracy of transvaginal ultrasonographic measurement of the uterine cervix with Bishop’s score for the prediction of vaginal delivery after labor induction, with 25 mcg of misoprostol. METHODS: a prospective study for the validation of a diagnostic test was conducted on 126 pregnant women with indication for labor induction. The patients were evaluated by Bishop’s score and transvaginal ultrasonography for cervical measurement. They also undergone obstetric transabdominal ultrasound to evaluate static and fetal weight, as well as the amniotic fluid index, and basal cardiotocography for the evaluation of fetal vitality. Labor was induced with vaginal and sublingual misoprostol, one of the tablets containing 25 mcg of the drug and the other only placebo. The tablets were administered every six hours, with a maximum number of eight. Frequency tables were obtained, and measures of central tendency and dispersion were calculated. ROC curves were constructed for the evaluation of Bishop’s score and ultrasonographic measurement of the uterine cervix for the prediction of vaginal delivery. RESULTS: the area under the ROC curve was 0.5 (p=0.8) for the ultrasonographic measurement of the uterine cervix, and 0.6 (p=0.02) for Bishop’s score (cut point ³4). Bishop’s score had a sensitivity of 56.2% and specificity of 67.9% for prediction of vaginal delivery, with a positive likelihood ratio of 1.75 and a negative one of 0.65. CONCLUSIONS: ultrasonographic measurement of the uterine cervix was not a good predictor of evolution to vaginal delivery among patients with misoprostol-induced labor. Bishop’s score was a better predictor of vaginal delivery under these circumstances.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 01-23-2012;33(11):361-366
DOI 10.1590/S0100-72032011001100007
PURPOSE: to compare the accuracy of transvaginal ultrasonographic measurement of the uterine cervix with Bishop’s score for the prediction of vaginal delivery after labor induction, with 25 mcg of misoprostol. METHODS: a prospective study for the validation of a diagnostic test was conducted on 126 pregnant women with indication for labor induction. The patients were evaluated by Bishop’s score and transvaginal ultrasonography for cervical measurement. They also undergone obstetric transabdominal ultrasound to evaluate static and fetal weight, as well as the amniotic fluid index, and basal cardiotocography for the evaluation of fetal vitality. Labor was induced with vaginal and sublingual misoprostol, one of the tablets containing 25 mcg of the drug and the other only placebo. The tablets were administered every six hours, with a maximum number of eight. Frequency tables were obtained, and measures of central tendency and dispersion were calculated. ROC curves were constructed for the evaluation of Bishop’s score and ultrasonographic measurement of the uterine cervix for the prediction of vaginal delivery. RESULTS: the area under the ROC curve was 0.5 (p=0.8) for the ultrasonographic measurement of the uterine cervix, and 0.6 (p=0.02) for Bishop’s score (cut point ³4). Bishop’s score had a sensitivity of 56.2% and specificity of 67.9% for prediction of vaginal delivery, with a positive likelihood ratio of 1.75 and a negative one of 0.65. CONCLUSIONS: ultrasonographic measurement of the uterine cervix was not a good predictor of evolution to vaginal delivery among patients with misoprostol-induced labor. Bishop’s score was a better predictor of vaginal delivery under these circumstances.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 08-05-2011;33(4):157-163
DOI 10.1590/S0100-72032011000400002
PURPOSE: to determine the best Doppler flow velocimetry index to predict small infants for gestational age (SGAI), in pregnant women with hypertensive syndromes. METHODS: a cross-sectional study was conducted enrolling 129 women with high blood pressure, submitted to dopplervelocimetry up to 15 days before delivery. Women with multiple fetuses, fetal malformations, genital bleeding, placental abruption, premature rupture of fetal membranes, smoking, use of illicit drugs, and chronic diseases were excluded. A receiver operating characteristic (ROC) curve for each Doppler variable was constructed to diagnose SGAI and the sensitivity (Se), specificity (Sp), positive (PLR) and negative (NLR) likelihood ratio were calculated. RESULTS: the area under the ROC curve for the middle cerebral artery resistance index was 52% (p=0.79) with Se, Sp, PLR, and NLR of 25.0, 89.1, 2.3 and 0.84% for a resistance index lower than 0.70, respectively. While the area under the ROC curve for the resistance index of the umbilical artery was 74% (p=0.0001), with Se=50.0%, Sp=90.0%, PLR=5.0 and NLR=0.56, for a resistance index higher or equal to 0.70. The area under the ROC curve for the resistance index umbilical artery/middle cerebral artery ratio was 75% (p=0.0001). When it was higher than 0.86, the Se, Sp, PLR and NLR were 70.8, 80.0, 3.4 and 0.36%, respectively. For the resistance index of the middle cerebral artery/uterine artery ratio, the area under the ROC curve was 71% (p=0.0001). We found a Se=52.2%, Sp=85.9%, PLR=3.7 and NLR=0.56, when the ratio was lower than 1.05. When we compared the area under the ROC curve of the four dopplervelocimetry indexes, we observed that only the resistance index umbilical artery/middle cerebral artery, resistance index middle cerebral artery/uterine artery and resistance index umbilical artery ratios seem to be useful for the prediction of SGA. CONCLUSION: in patients with high blood pressure during pregnancy, all dopplervelocimetry parameters, except the middle cerebral artery resistance index, can be used to predict SGAI. The umbilical artery/middle cerebral artery ratio seems to be the most recommended one.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 08-05-2011;33(4):157-163
DOI 10.1590/S0100-72032011000400002
PURPOSE: to determine the best Doppler flow velocimetry index to predict small infants for gestational age (SGAI), in pregnant women with hypertensive syndromes. METHODS: a cross-sectional study was conducted enrolling 129 women with high blood pressure, submitted to dopplervelocimetry up to 15 days before delivery. Women with multiple fetuses, fetal malformations, genital bleeding, placental abruption, premature rupture of fetal membranes, smoking, use of illicit drugs, and chronic diseases were excluded. A receiver operating characteristic (ROC) curve for each Doppler variable was constructed to diagnose SGAI and the sensitivity (Se), specificity (Sp), positive (PLR) and negative (NLR) likelihood ratio were calculated. RESULTS: the area under the ROC curve for the middle cerebral artery resistance index was 52% (p=0.79) with Se, Sp, PLR, and NLR of 25.0, 89.1, 2.3 and 0.84% for a resistance index lower than 0.70, respectively. While the area under the ROC curve for the resistance index of the umbilical artery was 74% (p=0.0001), with Se=50.0%, Sp=90.0%, PLR=5.0 and NLR=0.56, for a resistance index higher or equal to 0.70. The area under the ROC curve for the resistance index umbilical artery/middle cerebral artery ratio was 75% (p=0.0001). When it was higher than 0.86, the Se, Sp, PLR and NLR were 70.8, 80.0, 3.4 and 0.36%, respectively. For the resistance index of the middle cerebral artery/uterine artery ratio, the area under the ROC curve was 71% (p=0.0001). We found a Se=52.2%, Sp=85.9%, PLR=3.7 and NLR=0.56, when the ratio was lower than 1.05. When we compared the area under the ROC curve of the four dopplervelocimetry indexes, we observed that only the resistance index umbilical artery/middle cerebral artery, resistance index middle cerebral artery/uterine artery and resistance index umbilical artery ratios seem to be useful for the prediction of SGA. CONCLUSION: in patients with high blood pressure during pregnancy, all dopplervelocimetry parameters, except the middle cerebral artery resistance index, can be used to predict SGAI. The umbilical artery/middle cerebral artery ratio seems to be the most recommended one.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 03-15-2010;32(2):82-87
DOI 10.1590/S0100-72032010000200006
PURPOSE: to study the clinical and microbiological profile of women with bacterial vaginosis participating in a randomized, double-blind clinical trial, which compared the vaginal use of preparations from red pepper tree and metronidazole for the treatment of genital discharge. METHODS: the study was conducted on a series of 277 women with bacterial vaginosis concomitantly diagnosed by the criteria of Amsel and Nugent, selected from a total of 462 recruited patients using the information obtained before intervention. Data were analyzed with the Epi-Info 3.32 software. In order to compare the outcomes frequencies between the intervention groups, the χ2 test was used and the risk ratio and 95% confidence interval were calculated. The intention to treat analysis was performed. In addition to the determination of diagnostic parameters, the culture of vaginal content and a Papanicolaou cytology test were also performed. RESULTS: the most frequent clinical complaints were genital discharge, observed in 206 participants (74.4%) and the fish odor of the vaginal secretion, which occurred in 68.6% of the cases (190 patients). Among the diagnostic clinical criteria, the presence of clue-cells was positive in 275 women (99.3%), the Whiff test, in 266 (96.0%), followed by pH >4.5, which occurred in 92.8% of the cases, and by the presence of fluid grayish discharge reported by 206 participants (74.4%). Regarding the Nugent criterion, the median score was 8.0. Culture of the vaginal content permitted the identification of Gardnerella vaginalis in 96.8% of cases and of Mobiluncus in 53.1%. Only one third of the exams showed the presence of Lactobacillus (89 women - 32.1%). Fungal growth occurred in the cultures of 14 participants (5.1%). In most cases, culture revealed the presence of Corynebacterium (94.2%), Gram-positive cocci (98.2%), as well as Gram-positive (99.3%) and Gram-negative (91.0%) bacilli. Oncotic colposcopy revealed a very scarce presence of lactobacilli, which were present in only 8 cytological exams (2.9%) out of the total of 273 exams performed. CONCLUSIONS: the results of the present study did not differ from the literature regarding the symptoms reported by the women, the clinical criteria most frequently observed in the diagnosis, or the bacterial species detected in cultures of vaginal content. These findings indicate the need for further studies that might better elucidate the interrelations between the microbiological findings and the clinical expression of bacterial vaginosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 03-15-2010;32(2):82-87
DOI 10.1590/S0100-72032010000200006
PURPOSE: to study the clinical and microbiological profile of women with bacterial vaginosis participating in a randomized, double-blind clinical trial, which compared the vaginal use of preparations from red pepper tree and metronidazole for the treatment of genital discharge. METHODS: the study was conducted on a series of 277 women with bacterial vaginosis concomitantly diagnosed by the criteria of Amsel and Nugent, selected from a total of 462 recruited patients using the information obtained before intervention. Data were analyzed with the Epi-Info 3.32 software. In order to compare the outcomes frequencies between the intervention groups, the χ2 test was used and the risk ratio and 95% confidence interval were calculated. The intention to treat analysis was performed. In addition to the determination of diagnostic parameters, the culture of vaginal content and a Papanicolaou cytology test were also performed. RESULTS: the most frequent clinical complaints were genital discharge, observed in 206 participants (74.4%) and the fish odor of the vaginal secretion, which occurred in 68.6% of the cases (190 patients). Among the diagnostic clinical criteria, the presence of clue-cells was positive in 275 women (99.3%), the Whiff test, in 266 (96.0%), followed by pH >4.5, which occurred in 92.8% of the cases, and by the presence of fluid grayish discharge reported by 206 participants (74.4%). Regarding the Nugent criterion, the median score was 8.0. Culture of the vaginal content permitted the identification of Gardnerella vaginalis in 96.8% of cases and of Mobiluncus in 53.1%. Only one third of the exams showed the presence of Lactobacillus (89 women - 32.1%). Fungal growth occurred in the cultures of 14 participants (5.1%). In most cases, culture revealed the presence of Corynebacterium (94.2%), Gram-positive cocci (98.2%), as well as Gram-positive (99.3%) and Gram-negative (91.0%) bacilli. Oncotic colposcopy revealed a very scarce presence of lactobacilli, which were present in only 8 cytological exams (2.9%) out of the total of 273 exams performed. CONCLUSIONS: the results of the present study did not differ from the literature regarding the symptoms reported by the women, the clinical criteria most frequently observed in the diagnosis, or the bacterial species detected in cultures of vaginal content. These findings indicate the need for further studies that might better elucidate the interrelations between the microbiological findings and the clinical expression of bacterial vaginosis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 08-13-2009;31(6):285-292
DOI 10.1590/S0100-72032009000600004
PURPOSE: to investigate the main factors associated with fetal death in the city of Recife, Pernambuco, Brazil. METHODS: an observational, case-control study, including cases attended from June 1st 2004 to 31st March 2005. A number of 116 stillbirth cases and 472 live birth controls, with deliveries assisted at the service, were included. The cases were identified in the record book from the delivery room. The puerperium women were identified by the name and register number at a puerperium infirmary. The controls were selected, using the puerperium infirmary neighborhood criterion, identifying the beds with numbers immediately lower (two patients) and higher (two patients) than the patient's, as far as they had delivered live babies. In case they did not agree to participate in the research, the next beds with numbers consecutively lower or higher were approached. The χ2 association and Fisher's exact tests were used when necessary to test the association between the independent (predictive) and dependent (stillborn) variables, considering 5% as the significance level. To determine the association strength, the estimate of relative risk for case-control cases, Odds Ratio (OR) was used, with 95% as the confidence interval (CI). Logistic regression analysis according to the hierarchy model was done to control confounding factors. RESULTS: the fetal mortality rate corresponded to 24.4 by 1,000 births. After the multivariate analysis, the variables which kept significantly associated with fetal death were: malformation (OR=7.5; CI=3.2-17.4), number of pre-natal appointments lower than six (OR=4.4; CI=2.5-7.5), hemorrhagic syndromes (OR=2.9; CI=1.4-5.7), attendance in another hospital unit along the 24 hours which preceded the patient's admission in the institution (OR=2.9; CI=1.8-4.6), mothers' age over or equal to 35 years old (OR=2.2; CI=1.0-4.9) and schooling lower than eight years (OR=1.6; CI=1.02-2.6). CONCLUSIONS: it was found a high fetal mortality coefficient, the main factors associated with death were: malformation, number of pre-natal appointments lower than six, hemorrhagic syndromes, history of attendance previous to the hospital admission, mothers' age over or equal to 35 and schooling lower than eight years.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 08-13-2009;31(6):285-292
DOI 10.1590/S0100-72032009000600004
PURPOSE: to investigate the main factors associated with fetal death in the city of Recife, Pernambuco, Brazil. METHODS: an observational, case-control study, including cases attended from June 1st 2004 to 31st March 2005. A number of 116 stillbirth cases and 472 live birth controls, with deliveries assisted at the service, were included. The cases were identified in the record book from the delivery room. The puerperium women were identified by the name and register number at a puerperium infirmary. The controls were selected, using the puerperium infirmary neighborhood criterion, identifying the beds with numbers immediately lower (two patients) and higher (two patients) than the patient's, as far as they had delivered live babies. In case they did not agree to participate in the research, the next beds with numbers consecutively lower or higher were approached. The χ2 association and Fisher's exact tests were used when necessary to test the association between the independent (predictive) and dependent (stillborn) variables, considering 5% as the significance level. To determine the association strength, the estimate of relative risk for case-control cases, Odds Ratio (OR) was used, with 95% as the confidence interval (CI). Logistic regression analysis according to the hierarchy model was done to control confounding factors. RESULTS: the fetal mortality rate corresponded to 24.4 by 1,000 births. After the multivariate analysis, the variables which kept significantly associated with fetal death were: malformation (OR=7.5; CI=3.2-17.4), number of pre-natal appointments lower than six (OR=4.4; CI=2.5-7.5), hemorrhagic syndromes (OR=2.9; CI=1.4-5.7), attendance in another hospital unit along the 24 hours which preceded the patient's admission in the institution (OR=2.9; CI=1.8-4.6), mothers' age over or equal to 35 years old (OR=2.2; CI=1.0-4.9) and schooling lower than eight years (OR=1.6; CI=1.02-2.6). CONCLUSIONS: it was found a high fetal mortality coefficient, the main factors associated with death were: malformation, number of pre-natal appointments lower than six, hemorrhagic syndromes, history of attendance previous to the hospital admission, mothers' age over or equal to 35 and schooling lower than eight years.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 07-29-2009;31(5):241-248
DOI 10.1590/S0100-72032009000500007
OBJECTIVE: to determine the frequency of macrosomia in babies born alive at a reference obstetric service, and its association with maternal risk factors. METHODS: a transversal descriptive study, including 551 women at puerperium, hospitalized at Instituto de Saúde Elpídio de Almeida, in Campina Grande (PB), Brazil, from August to October, 2007. Women, whose deliveries had been assisted at the institution, with babies born alive from one single gestation and approached in the first postpartum day, were included in the study. The nutritional and sociodemographic maternal characteristics were analyzed, and the ratio of macrosomia (birth weight >4.000 g) and its association with maternal variables were determined. Macrosomia was classified as symmetric or asymmetric according to Rohrer's index. Statistical analysis has been done through Epi-Info 3.5 software; the prevalence ratio (PR) and the confidence interval at 95% (CI 95%) were calculated. The research protocol was approved by the local Ethics Committee and all the participants signed the informed consent. RESULTS: the mean maternal age was 24.7 years old, and the mean gestational age was 38.6 weeks. Excessive gestational weight gain was observed in 21.3% of the pregnant women, and 2.1% of the participants had a diagnosis of diabetes mellitus (gestational or clinic). A ratio of 5.4% of macrosomic newborns was found, 60 were asymmetric. There was no significant association between macrosomia, mother's age and parity. There was an association between macrosomia and overweight/obesity in the pre-gestational period (PR=2.9; CI 95%=1.0-7.8) and at the last medical appointment (PR=4.9; CI 95%=1.9-12.5), excessive weight gain (PR = 6.9; CI 95%:2.8-16.9), clinical or gestational diabetes (PR = 8.9; CI 95%:4.1-19.4) and hypertension (PR=2.9; CI 95%=1.1-7.9). The factors that persisted significantly associated with macrosomia in the multivariate analysis were the excessive weight gain during the gestation (RR=6.9; CI 95%=2.9-16.9) and the presence of diabetes mellitus (RR=8.9, CI 95%=4.1-19.4). CONCLUSIONS: considering that excessive gestational weight gain and diabetes mellitus were the factors more strongly associated with macrosomia, it is important that precocious detection measurements and adequate follow-up of such conditions be taken, aiming at preventing unfavorable perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 07-29-2009;31(5):241-248
DOI 10.1590/S0100-72032009000500007
OBJECTIVE: to determine the frequency of macrosomia in babies born alive at a reference obstetric service, and its association with maternal risk factors. METHODS: a transversal descriptive study, including 551 women at puerperium, hospitalized at Instituto de Saúde Elpídio de Almeida, in Campina Grande (PB), Brazil, from August to October, 2007. Women, whose deliveries had been assisted at the institution, with babies born alive from one single gestation and approached in the first postpartum day, were included in the study. The nutritional and sociodemographic maternal characteristics were analyzed, and the ratio of macrosomia (birth weight >4.000 g) and its association with maternal variables were determined. Macrosomia was classified as symmetric or asymmetric according to Rohrer's index. Statistical analysis has been done through Epi-Info 3.5 software; the prevalence ratio (PR) and the confidence interval at 95% (CI 95%) were calculated. The research protocol was approved by the local Ethics Committee and all the participants signed the informed consent. RESULTS: the mean maternal age was 24.7 years old, and the mean gestational age was 38.6 weeks. Excessive gestational weight gain was observed in 21.3% of the pregnant women, and 2.1% of the participants had a diagnosis of diabetes mellitus (gestational or clinic). A ratio of 5.4% of macrosomic newborns was found, 60 were asymmetric. There was no significant association between macrosomia, mother's age and parity. There was an association between macrosomia and overweight/obesity in the pre-gestational period (PR=2.9; CI 95%=1.0-7.8) and at the last medical appointment (PR=4.9; CI 95%=1.9-12.5), excessive weight gain (PR = 6.9; CI 95%:2.8-16.9), clinical or gestational diabetes (PR = 8.9; CI 95%:4.1-19.4) and hypertension (PR=2.9; CI 95%=1.1-7.9). The factors that persisted significantly associated with macrosomia in the multivariate analysis were the excessive weight gain during the gestation (RR=6.9; CI 95%=2.9-16.9) and the presence of diabetes mellitus (RR=8.9, CI 95%=4.1-19.4). CONCLUSIONS: considering that excessive gestational weight gain and diabetes mellitus were the factors more strongly associated with macrosomia, it is important that precocious detection measurements and adequate follow-up of such conditions be taken, aiming at preventing unfavorable perinatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 10-23-2008;30(9):459-465
DOI 10.1590/S0100-72032008000900006
PURPOSE: to evaluate the effect of maternal, socioeconomic and obstetric variables, as well the presence of artery incisions in the 20th and 24th weeks on the fetal weight estimated at the end of pregnancy (36th week) in pregnant women attended by Programa Saúde da Família, in an inland town of the northeast of Brazil. METHODS: a longitudinal study including 137 pregnant women, who have been followed up every four weeks in order to assess clinical, socioeconomic and obstetric conditions, including their weight. The uterine arteries were evaluated by Doppler in the 20th and 24th weeks, the fetal weight and the amniotic fluid index (AFI), determined in the 36th week. The initial maternal nutritional state has been determined by the body mass index (BMI), the pregnant women being classified as low weight, eutrophic, over weight and obese. Weight gain during gestation has been evaluated, according to the initial nutritional state, being classified at the end of the second and third trimester as insufficient, adequate and excessive weight gain. Analysis of variance was performed to evaluate the association of the fetal weight in the 36th week with the predictor variables, adjusted by multiple linear regression. RESULTS: an association between the fetal weight estimated in the 36th week and the mother's age (p=0.02), mother's job (p=0.02), initial nutritional state (p=0.04), weight gain in the second trimester (p=0.01), presence of incisions in the uterine arteries (p=0.02), and AFI (p=0.007) has been observed. The main factors associated to the fetal weight estimated in the 36th week, after the multiple regression analysis were: BMI at the pregnancy onset, weight gain in the second trimester, AFI and tabagism. CONCLUSIONS: in the present study, the fetal weight is positively associated with the initial maternal nutritional state, the weight gain in the second trimester and the volume of amniotic fluid, and negatively, to tabagism.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 10-23-2008;30(9):459-465
DOI 10.1590/S0100-72032008000900006
PURPOSE: to evaluate the effect of maternal, socioeconomic and obstetric variables, as well the presence of artery incisions in the 20th and 24th weeks on the fetal weight estimated at the end of pregnancy (36th week) in pregnant women attended by Programa Saúde da Família, in an inland town of the northeast of Brazil. METHODS: a longitudinal study including 137 pregnant women, who have been followed up every four weeks in order to assess clinical, socioeconomic and obstetric conditions, including their weight. The uterine arteries were evaluated by Doppler in the 20th and 24th weeks, the fetal weight and the amniotic fluid index (AFI), determined in the 36th week. The initial maternal nutritional state has been determined by the body mass index (BMI), the pregnant women being classified as low weight, eutrophic, over weight and obese. Weight gain during gestation has been evaluated, according to the initial nutritional state, being classified at the end of the second and third trimester as insufficient, adequate and excessive weight gain. Analysis of variance was performed to evaluate the association of the fetal weight in the 36th week with the predictor variables, adjusted by multiple linear regression. RESULTS: an association between the fetal weight estimated in the 36th week and the mother's age (p=0.02), mother's job (p=0.02), initial nutritional state (p=0.04), weight gain in the second trimester (p=0.01), presence of incisions in the uterine arteries (p=0.02), and AFI (p=0.007) has been observed. The main factors associated to the fetal weight estimated in the 36th week, after the multiple regression analysis were: BMI at the pregnancy onset, weight gain in the second trimester, AFI and tabagism. CONCLUSIONS: in the present study, the fetal weight is positively associated with the initial maternal nutritional state, the weight gain in the second trimester and the volume of amniotic fluid, and negatively, to tabagism.