You searched for:"Gustavo Salata Romão"
We found (14) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo17
To determine the prevalence of anxiety, depression and burnout in residents of Gynecology and Obstetrics during COVID-19 pandemic in Brazil and its associated factors.
Cross-sectional study involving all regions of Brazil, through the application of a sociodemographic questionnaire, the Hospital Anxiety and Depression Scale (HAD) and the Maslach Burnout Inventory (MBI-HSS) instrument. Multivariate analysis was performed after adjusting the Poisson model.
Among the 719 participating medical residents, screening was positive for anxiety in 75.7% and for depression in 49.8% of cases. Burnout syndrome was evidenced in 41.3% of the physicians studied. Those with depression are more likely to have anxiety (OR 0.797; 95%CI 0.687 - 0.925) and burnout syndrome (OR 0.847 95%CI 0.74 - 0.97). Residents with anxiety (OR 0.805; 95%CI 0.699 - 0.928) and burnout (OR 0.841; 95%CI 0.734 - 0.963) are more likely to have depression.
High prevalence of anxiety, depression and burnout were found in residents of Gynecology and Obstetrics in Brazil, in addition to important correlations between anxiety-depression and depression-burnout.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2024;46:e-rbgo17
To determine the prevalence of anxiety, depression and burnout in residents of Gynecology and Obstetrics during COVID-19 pandemic in Brazil and its associated factors.
Cross-sectional study involving all regions of Brazil, through the application of a sociodemographic questionnaire, the Hospital Anxiety and Depression Scale (HAD) and the Maslach Burnout Inventory (MBI-HSS) instrument. Multivariate analysis was performed after adjusting the Poisson model.
Among the 719 participating medical residents, screening was positive for anxiety in 75.7% and for depression in 49.8% of cases. Burnout syndrome was evidenced in 41.3% of the physicians studied. Those with depression are more likely to have anxiety (OR 0.797; 95%CI 0.687 - 0.925) and burnout syndrome (OR 0.847 95%CI 0.74 - 0.97). Residents with anxiety (OR 0.805; 95%CI 0.699 - 0.928) and burnout (OR 0.841; 95%CI 0.734 - 0.963) are more likely to have depression.
High prevalence of anxiety, depression and burnout were found in residents of Gynecology and Obstetrics in Brazil, in addition to important correlations between anxiety-depression and depression-burnout.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):819-820
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(9):819-820
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):621-628
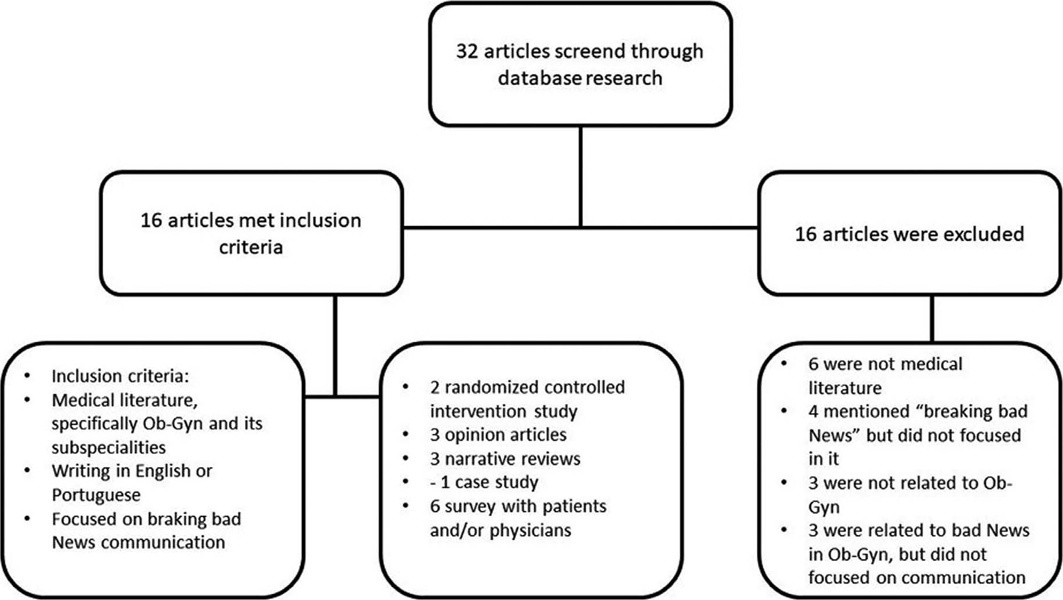
Breaking bad news is common in obstetrics and gynecology (ob-gyn). However, it is difficult, and few doctors receive training on how to deal with this situation. This narrative review aims to gather, analyze, and synthesize part of the knowledge on the area, focused on Ob-Gyn. Among the 16 selected articles, two are randomized controlled intervention studies, and most studies refer to obstetrics. The results found by us pointed out that simulation, feedback/debriefing, lectures, and protocols could improve doctors’ performance in communicating bad news. For patients, the context and how the information is transmitted seem to impact more than the content of the news. Ob-Gyn doctors could benefit from specific protocols and education, given the specialty’s particularities. There is a lack of evidence about the most effective way to conduct such training. Finding validated ways to quantify and classify studies’ results in the area, which would allow for the objective analysis of outcomes, is one of the biggest challenges concerning this topic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):621-628
Breaking bad news is common in obstetrics and gynecology (ob-gyn). However, it is difficult, and few doctors receive training on how to deal with this situation. This narrative review aims to gather, analyze, and synthesize part of the knowledge on the area, focused on Ob-Gyn. Among the 16 selected articles, two are randomized controlled intervention studies, and most studies refer to obstetrics. The results found by us pointed out that simulation, feedback/debriefing, lectures, and protocols could improve doctors’ performance in communicating bad news. For patients, the context and how the information is transmitted seem to impact more than the content of the news. Ob-Gyn doctors could benefit from specific protocols and education, given the specialty’s particularities. There is a lack of evidence about the most effective way to conduct such training. Finding validated ways to quantify and classify studies’ results in the area, which would allow for the objective analysis of outcomes, is one of the biggest challenges concerning this topic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(6):425-428
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(6):425-428
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):411-414
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):411-414
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(5):272-288
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(5):272-288
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):01-03
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):01-03
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(3):136-140
DOI 10.1590/S0100-72032013000300008
Anti-mullerian hormone (AMH) is a glycoprotein produced by granulosa cells of primary, pre-antral and small antral ovarian follicles and its clinical applicability has been recently demonstrated by several studies. Prediction of the response to ovarian stimulation for in vitro fertilization corresponds to the most frequent utilization of AMH in clinical practice, being routinely assessed in many services to identify subgroups of women susceptible to a poor response or to Ovarian Hyperstimulation Syndrome. There are great perspectives that AMH may be applicable to the individual determination of risk for iatrogenic gonadal injury in women with neoplasms who will be submitted to chemotherapy. It is also probable that AMH assessment will be included in protocols for the investigation of amenorrhea and oligomenorrhea, since AMH levels are increased in Polycystic Ovary Syndrome, reduced in premature ovarian failure and normal in other conditions such as hyperprolactinemia and hypogonadotropic hypogonadism. It is possible that AMH will be utilized in the future for the prediction of age at menopause and of reproductive prognosis, providing solid bases for pre-conceptive and contraceptive counseling.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2013;35(3):136-140
DOI 10.1590/S0100-72032013000300008
Anti-mullerian hormone (AMH) is a glycoprotein produced by granulosa cells of primary, pre-antral and small antral ovarian follicles and its clinical applicability has been recently demonstrated by several studies. Prediction of the response to ovarian stimulation for in vitro fertilization corresponds to the most frequent utilization of AMH in clinical practice, being routinely assessed in many services to identify subgroups of women susceptible to a poor response or to Ovarian Hyperstimulation Syndrome. There are great perspectives that AMH may be applicable to the individual determination of risk for iatrogenic gonadal injury in women with neoplasms who will be submitted to chemotherapy. It is also probable that AMH assessment will be included in protocols for the investigation of amenorrhea and oligomenorrhea, since AMH levels are increased in Polycystic Ovary Syndrome, reduced in premature ovarian failure and normal in other conditions such as hyperprolactinemia and hypogonadotropic hypogonadism. It is possible that AMH will be utilized in the future for the prediction of age at menopause and of reproductive prognosis, providing solid bases for pre-conceptive and contraceptive counseling.