Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):119-121
DOI 10.1590/S0100-72032001000200010
Endometrial metaplastic ossification is a rare condition and can be partially explained by a neoformation in the endometrium, with calcium deposition. However, a common situation is the previous history of abortion with persistence of ossicles in the uterine cavity. The endometrial ossification was reported in a 31-year-old woman, without previous pregnancy or history of abortion. This patient presented dysmenorrhea and infertility. Pelvic ultrasonography showed a hyperechoic area in the uterine fundus. Histeroscopy was performed and an image suggestive of bone was seen. This tissue was removed by histeroscopy and the histopathological analysis confirmed endometrial ossification.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(2):119-121
DOI 10.1590/S0100-72032001000200010
Endometrial metaplastic ossification is a rare condition and can be partially explained by a neoformation in the endometrium, with calcium deposition. However, a common situation is the previous history of abortion with persistence of ossicles in the uterine cavity. The endometrial ossification was reported in a 31-year-old woman, without previous pregnancy or history of abortion. This patient presented dysmenorrhea and infertility. Pelvic ultrasonography showed a hyperechoic area in the uterine fundus. Histeroscopy was performed and an image suggestive of bone was seen. This tissue was removed by histeroscopy and the histopathological analysis confirmed endometrial ossification.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(9):605-607
DOI 10.1590/S0100-72032001000900009
Actinomycosis of the breast is a rare inflammatory disease that has been infrequently reported. It can be primary actinomycosis of the breast, when caused by lesions of the mammary skin and secondary, when there is thoracic or pleural infection; it has extremely variable clinical presentations and may simulate mastitis and malignancies such as inflammatory carcinoma. The diagnosis is confirmed by culture and by finding typical actinomycotic colonies. The usual treatment is surgical drainage and intravenous and oral long-term administration of antibiotics. The authors present a case of actinomycosis of the breast in a 12-week pregnant woman who presented a tumor in the left breast.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(9):605-607
DOI 10.1590/S0100-72032001000900009
Actinomycosis of the breast is a rare inflammatory disease that has been infrequently reported. It can be primary actinomycosis of the breast, when caused by lesions of the mammary skin and secondary, when there is thoracic or pleural infection; it has extremely variable clinical presentations and may simulate mastitis and malignancies such as inflammatory carcinoma. The diagnosis is confirmed by culture and by finding typical actinomycotic colonies. The usual treatment is surgical drainage and intravenous and oral long-term administration of antibiotics. The authors present a case of actinomycosis of the breast in a 12-week pregnant woman who presented a tumor in the left breast.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(8):535-539
DOI 10.1590/S0100-72032001000800009
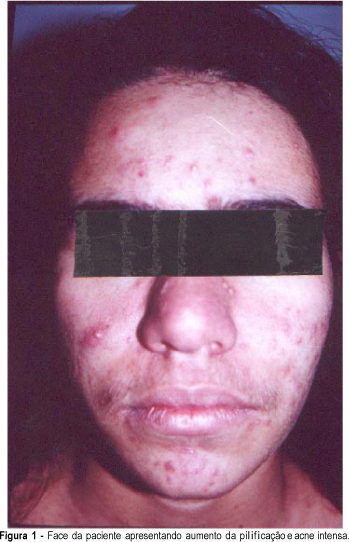
Luteomas of pregnancy are ovarian pseudotumors diagnosed by ultrasound, during cesarean section or at postdelivery tubal ligation. Twenty-five per cent of the cases appear around the second half of pregnancy. Usually there are signs of maternal virilization and 50% are detected because female newborns show clitorimegaly and/or labial fusion. The concentrations of androgenic steroids in the maternal blood during pregnancy and in the cord blood at child-birth show significantly increased rates. The ultrasound shows solid or cystic-solid structures and few weeks after the delivery they decrease and the ovary size returns to normal. The authors report a case of a patient who exhibited virilization signs in two consecutive pregnancies as well as in the two female fetuses. At adnexal sonographic examination a solid tumoral image was found in both pregnancies. Serum androgen levels were increased.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(8):535-539
DOI 10.1590/S0100-72032001000800009
Luteomas of pregnancy are ovarian pseudotumors diagnosed by ultrasound, during cesarean section or at postdelivery tubal ligation. Twenty-five per cent of the cases appear around the second half of pregnancy. Usually there are signs of maternal virilization and 50% are detected because female newborns show clitorimegaly and/or labial fusion. The concentrations of androgenic steroids in the maternal blood during pregnancy and in the cord blood at child-birth show significantly increased rates. The ultrasound shows solid or cystic-solid structures and few weeks after the delivery they decrease and the ovary size returns to normal. The authors report a case of a patient who exhibited virilization signs in two consecutive pregnancies as well as in the two female fetuses. At adnexal sonographic examination a solid tumoral image was found in both pregnancies. Serum androgen levels were increased.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(7):465-468
DOI 10.1590/S0100-72032001000700009
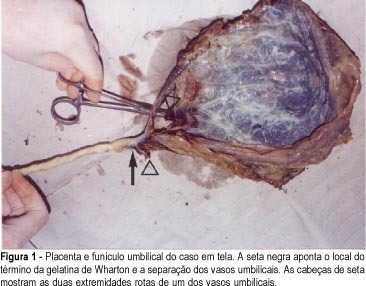
The differential diagnosis of hemorrhages during the third trimester of pregnancy due exclusively to obstetrical causes includes: abruptio placentae, low insertion of placenta (placenta previa with subtypes), rupture of the uterus, rupture of the marginal placental sinus and rupture of the vasa previa. The three first diagnoses occur more frequently, their epidemiological factors are better known and therefore, have an easier diagnosis. It is common for obstetricians with long practical experience, as well as for ultrasonographers specialized in fetal medicine and who thoroughly know their theory, not to have ever been exposed to practical obstetrical cases of vasa previa or their rupture. The reason to write this article was the fact that, during the past 32 years, we have been working constantly and uninterruptedly in obstetrical practice and we have seen only one case of rupture of vasa previa during labor, which killed the fetus. Initially, we investigated the issue in obstetrical textbooks having no luck whatsoever, except for a couple of lines on the subject. Carrying out our search in depth, we were able to learn that, even though a rarity, today's literature on the subject suggests that it is possible to have a diagnosis for this morbid entity during gestation, and to solve the problem by making the cesarian section mandatory in these cases, leading to a significant reduction in the actual fetal mortality figures which, according to experts, vary between 33 and 100%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(7):465-468
DOI 10.1590/S0100-72032001000700009
The differential diagnosis of hemorrhages during the third trimester of pregnancy due exclusively to obstetrical causes includes: abruptio placentae, low insertion of placenta (placenta previa with subtypes), rupture of the uterus, rupture of the marginal placental sinus and rupture of the vasa previa. The three first diagnoses occur more frequently, their epidemiological factors are better known and therefore, have an easier diagnosis. It is common for obstetricians with long practical experience, as well as for ultrasonographers specialized in fetal medicine and who thoroughly know their theory, not to have ever been exposed to practical obstetrical cases of vasa previa or their rupture. The reason to write this article was the fact that, during the past 32 years, we have been working constantly and uninterruptedly in obstetrical practice and we have seen only one case of rupture of vasa previa during labor, which killed the fetus. Initially, we investigated the issue in obstetrical textbooks having no luck whatsoever, except for a couple of lines on the subject. Carrying out our search in depth, we were able to learn that, even though a rarity, today's literature on the subject suggests that it is possible to have a diagnosis for this morbid entity during gestation, and to solve the problem by making the cesarian section mandatory in these cases, leading to a significant reduction in the actual fetal mortality figures which, according to experts, vary between 33 and 100%.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(9):625-628
DOI 10.1590/S0100-72032002000900009
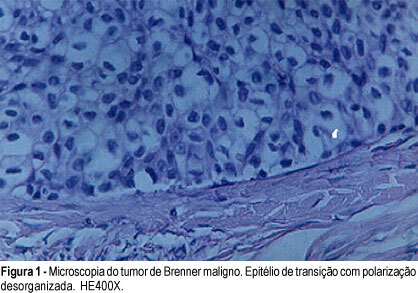
Brenner's tumor is small, unilateral and benign. Its diagnosis can only be confirmed by the anatomomicopathological examination, that on microscopy presents nests or columns of transition epithelial cells in a fibromatous matrix. The epithelial cells present a characteristic longitudinal "coffee bean" furrow and can undergo carcinomatous transformation. We present a case of a menopausal patient with vaginal bleeding, and a palpable abdominal mass. She was submitted to surgical treatment (total hysterectomy, bilateral oophorectomy and omentectomy) with the histopathological diagnosis of Brenner's bilateral tumor, being malignant on one side and benign on the other. After surgical treatment she is now alive for three years and free of disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(9):625-628
DOI 10.1590/S0100-72032002000900009
Brenner's tumor is small, unilateral and benign. Its diagnosis can only be confirmed by the anatomomicopathological examination, that on microscopy presents nests or columns of transition epithelial cells in a fibromatous matrix. The epithelial cells present a characteristic longitudinal "coffee bean" furrow and can undergo carcinomatous transformation. We present a case of a menopausal patient with vaginal bleeding, and a palpable abdominal mass. She was submitted to surgical treatment (total hysterectomy, bilateral oophorectomy and omentectomy) with the histopathological diagnosis of Brenner's bilateral tumor, being malignant on one side and benign on the other. After surgical treatment she is now alive for three years and free of disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(8):555-559
DOI 10.1590/S0100-72032002000800009
The hemolytic - uremic syndrome (HUS) presents with a triad of acute renal failure, microangiopathic hemolytic anemia and thrombocytopenia associated with high morbidity and mortality. On the differential diagnosis, other entities must be considered like preeclampsia, HELLP syndrome, acute fatty liver of pregnancy and thrombotic thrombocytopenic purpura. We report a case of HUS occurring in the immediate postpartum period in a patient initially diagnosed as having preeclampsia. The differential diagnosis was based on abrupt renal failure, blood pressure increase and clinical and laboratorial evidence of hemolysis. Attention is directed to investigation, clinical management and prognosis based on review of the literature.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(8):555-559
DOI 10.1590/S0100-72032002000800009
The hemolytic - uremic syndrome (HUS) presents with a triad of acute renal failure, microangiopathic hemolytic anemia and thrombocytopenia associated with high morbidity and mortality. On the differential diagnosis, other entities must be considered like preeclampsia, HELLP syndrome, acute fatty liver of pregnancy and thrombotic thrombocytopenic purpura. We report a case of HUS occurring in the immediate postpartum period in a patient initially diagnosed as having preeclampsia. The differential diagnosis was based on abrupt renal failure, blood pressure increase and clinical and laboratorial evidence of hemolysis. Attention is directed to investigation, clinical management and prognosis based on review of the literature.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(7):485-489
DOI 10.1590/S0100-72032002000700009
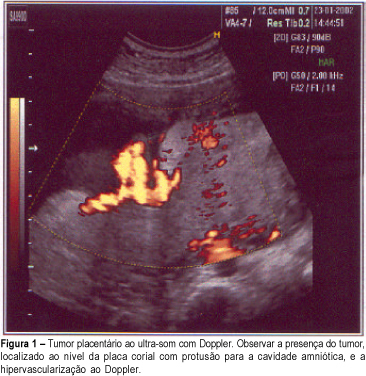
The most frequently nontrophoblastic tumor of the placenta found is chorioangioma, with an incidence of about 1%. When they are small, they do not significantly affect the fetus, but the large ones can cause intrauterine growth restriction, polyhydramnios, premature delivery, congestive heart failure and fetal death. The authors report a case of chorioangioma in a 28-year-old woman, second gestation, whose diagnosis was established at the 32nd week by ultrasound and confirmed by the anatomopathological examination. Ultrasonography evaluations showed chronic fetal distress and the delivery was performed at 36 weeks. The newborn results were satisfactory with Apgar 9-10 and fetal weight 2.460 g.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(7):485-489
DOI 10.1590/S0100-72032002000700009
The most frequently nontrophoblastic tumor of the placenta found is chorioangioma, with an incidence of about 1%. When they are small, they do not significantly affect the fetus, but the large ones can cause intrauterine growth restriction, polyhydramnios, premature delivery, congestive heart failure and fetal death. The authors report a case of chorioangioma in a 28-year-old woman, second gestation, whose diagnosis was established at the 32nd week by ultrasound and confirmed by the anatomopathological examination. Ultrasonography evaluations showed chronic fetal distress and the delivery was performed at 36 weeks. The newborn results were satisfactory with Apgar 9-10 and fetal weight 2.460 g.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):413-417
DOI 10.1590/S0100-72032002000600009
Massive hypertrophy of the breast in pregnancy is a rare condition, with few cases reported. In spite of the unknown etiology, it seems to be an exaggerated response of the breast receptors to the pregnancy hormones. Although it can happen in any pregnancy, it presents great capacity to recur in all subsequent pregnancies. The rapid and colossal breast enlargement determines pain and the involvement of the shoulder skeleton and muscles. The excessive enlargement may promote necrosis and ulceration of the skin, leading to breast infection. The authors report one case at the second pregnancy, explaining management during the pregnancy, lactation inhibition with bromocriptine immediately after the delivery and the banding of the elevated breast. They also emphasize the importance of reduction mammoplasty a few months after delivery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):413-417
DOI 10.1590/S0100-72032002000600009
Massive hypertrophy of the breast in pregnancy is a rare condition, with few cases reported. In spite of the unknown etiology, it seems to be an exaggerated response of the breast receptors to the pregnancy hormones. Although it can happen in any pregnancy, it presents great capacity to recur in all subsequent pregnancies. The rapid and colossal breast enlargement determines pain and the involvement of the shoulder skeleton and muscles. The excessive enlargement may promote necrosis and ulceration of the skin, leading to breast infection. The authors report one case at the second pregnancy, explaining management during the pregnancy, lactation inhibition with bromocriptine immediately after the delivery and the banding of the elevated breast. They also emphasize the importance of reduction mammoplasty a few months after delivery.
