Summary
. 2021;43(1):35-40
To evaluate the presence of residual disease in the uterine specimen after hysteroscopic polypectomy or polyp biopsy in patients with endometrioid endometrial cancer (EC).
We analyzed a series of 104 patients (92 cases from the Hospital AC Camargo and 12 from the Hospital do Servidor Público Estadual de São Paulo) with polyps that were diagnosed by hysteroscopy, showing endometrioid EC associated with the polyp or in the final pathological specimen. Patients underwent a surgical approach for endometrial cancer from January 2002 to January 2017. Their clinical and pathological data were retrospectively retrieved from the medical records.
In78cases (75%), thepolyphad EC, and in 40(38.5%), itwas restricted tothe polyp, without endometrial involvement. The pathologic stage was IA in 96 cases (92.3%) and 90 (86.5%) had histologic grade 1 or 2. In 18 cases (17.3%), there was no residual disease in the final uterine specimen, but only in 9 of them the hysteroscopy suggested that the tumor was restricted to the polyp. In 5 cases (4.8%) from the group without outside of the polyp during hysteroscopy, myometrial invasion was noted in the final uterine specimen. This finding suggests the possibility of disease extrapolation through the base of the polyp.
Patients with endometrioid EC associated with polyps may have the tumor completely removed during hysteroscopy, but the variables shown in the present study could not safely predict which patient would have no residual disease.
Summary
. 2021;43(1):35-40
To evaluate the presence of residual disease in the uterine specimen after hysteroscopic polypectomy or polyp biopsy in patients with endometrioid endometrial cancer (EC).
We analyzed a series of 104 patients (92 cases from the Hospital AC Camargo and 12 from the Hospital do Servidor Público Estadual de São Paulo) with polyps that were diagnosed by hysteroscopy, showing endometrioid EC associated with the polyp or in the final pathological specimen. Patients underwent a surgical approach for endometrial cancer from January 2002 to January 2017. Their clinical and pathological data were retrospectively retrieved from the medical records.
In78cases (75%), thepolyphad EC, and in 40(38.5%), itwas restricted tothe polyp, without endometrial involvement. The pathologic stage was IA in 96 cases (92.3%) and 90 (86.5%) had histologic grade 1 or 2. In 18 cases (17.3%), there was no residual disease in the final uterine specimen, but only in 9 of them the hysteroscopy suggested that the tumor was restricted to the polyp. In 5 cases (4.8%) from the group without outside of the polyp during hysteroscopy, myometrial invasion was noted in the final uterine specimen. This finding suggests the possibility of disease extrapolation through the base of the polyp.
Patients with endometrioid EC associated with polyps may have the tumor completely removed during hysteroscopy, but the variables shown in the present study could not safely predict which patient would have no residual disease.
Summary
. 2021;43(1):41-45
The aim of the present study was to analyze relapse rates and patterns in patients with endometrial cancer with the aim of evaluating the effectiveness of current follow-up procedures in terms of patient survival, as well as the convenience of modifying the surveillance strategy.
Retrospective descriptive study including all patients diagnosed with endometrial cancer relapse at the Department of Gynecology and Obstetrics of the Complejo Hospitalario Insular-Materno Infantil de Canarias, between 2005 and 2014.
Recurrence was observed in 81 patients (10.04% of the sample); 66.7% of them suffered relapse within 2 years and 80.2% within 3 years after the termination of the primary treatment; 41.9% showed distant metastases while the rest corresponded to local-regional (40.7%) or ganglionar (17.4%) relapse; 42% of these were symptomatic; 14 patients showed more than 1 site of relapse. Relapse was detected mainly through symptoms and physical examination findings (54.3%), followed by elevated serummarker levels (29.6%), computed tomography (CT) images (9.9%) and abnormal vaginal cytology findings (6.2%). No differences in global survival were found between patients with symptomatic or asymptomatic relapse.
Taking into account that the recurrence rate of endometrial cancer is low, that relapse occurs mainly within the first 3 years post-treatment and that symptom evaluation and physical examination are the most effective follow-up methods, we postulate that a modification of the current model of hospital follow-up should be considered.
Summary
. 2021;43(1):41-45
The aim of the present study was to analyze relapse rates and patterns in patients with endometrial cancer with the aim of evaluating the effectiveness of current follow-up procedures in terms of patient survival, as well as the convenience of modifying the surveillance strategy.
Retrospective descriptive study including all patients diagnosed with endometrial cancer relapse at the Department of Gynecology and Obstetrics of the Complejo Hospitalario Insular-Materno Infantil de Canarias, between 2005 and 2014.
Recurrence was observed in 81 patients (10.04% of the sample); 66.7% of them suffered relapse within 2 years and 80.2% within 3 years after the termination of the primary treatment; 41.9% showed distant metastases while the rest corresponded to local-regional (40.7%) or ganglionar (17.4%) relapse; 42% of these were symptomatic; 14 patients showed more than 1 site of relapse. Relapse was detected mainly through symptoms and physical examination findings (54.3%), followed by elevated serummarker levels (29.6%), computed tomography (CT) images (9.9%) and abnormal vaginal cytology findings (6.2%). No differences in global survival were found between patients with symptomatic or asymptomatic relapse.
Taking into account that the recurrence rate of endometrial cancer is low, that relapse occurs mainly within the first 3 years post-treatment and that symptom evaluation and physical examination are the most effective follow-up methods, we postulate that a modification of the current model of hospital follow-up should be considered.
Summary
. 2021;43(1):46-53
Magnetic resonance imaging (MRI) has been considered another tool for use during the pre- and postoperative periods of the management of pelvic-organ prolapse (POP). However, there is little consensus regarding its practical use for POP and the association betweenMRI lines of reference and physical examination.We aimedto evaluate the mid- to long-term results of two surgical techniques for apical prolapse.
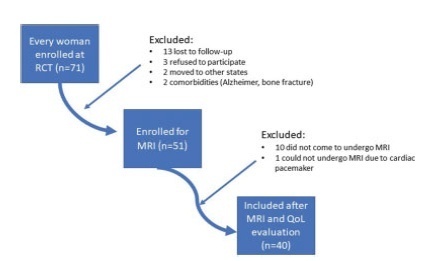
In total, 40 women with apical POP randomized from 2014 to 2016 underwent abdominal sacrocolpopexy (ASC group; n = 20) or bilateral vaginal sacrospinous fixation with an anterior mesh (VSF-AM group; n = 20). A physical examination using the POP Quantification System (POP-Q) for staging (objective cure) and the International Consultation on Incontinence Questionnaire-Vaginal Symptoms (ICIQ-VS: subjective cure), were applied and analyzed before and one year after surgery respectively. All MRI variables (pubococcigeous line [PCL], bladder base [BB], anorectal junction [ARJ], and the estimated levator ani subtended volume [eLASV]) were investigated one year after surgery. Significance was established at p < 0.05.
After a mean 27-month follow-up, according to the MRI criteria, 60% of the women were cured in the VSF-AM group versus 45% in ASC group (p= 0.52). The POP-Q and objective cure rates by MRI were correlated in the anterior vaginal wall (p= 0.007), but no correlationwas foundwith the subjective cure. The eLASVwas largeramongthe patients with surgical failure, and a cutoff of ≥ 33.5mm3 was associated with postoperative failure (area under the receiver operating characteristic curve [ROC]: 0.813; p= 0.002).
Both surgeries for prolapse were similar regarding theobjective variables (POP-Q measurements and MRI cure rates). Larger eLASV areas were associated with surgical failure.
Summary
. 2021;43(1):46-53
Magnetic resonance imaging (MRI) has been considered another tool for use during the pre- and postoperative periods of the management of pelvic-organ prolapse (POP). However, there is little consensus regarding its practical use for POP and the association betweenMRI lines of reference and physical examination.We aimedto evaluate the mid- to long-term results of two surgical techniques for apical prolapse.
In total, 40 women with apical POP randomized from 2014 to 2016 underwent abdominal sacrocolpopexy (ASC group; n = 20) or bilateral vaginal sacrospinous fixation with an anterior mesh (VSF-AM group; n = 20). A physical examination using the POP Quantification System (POP-Q) for staging (objective cure) and the International Consultation on Incontinence Questionnaire-Vaginal Symptoms (ICIQ-VS: subjective cure), were applied and analyzed before and one year after surgery respectively. All MRI variables (pubococcigeous line [PCL], bladder base [BB], anorectal junction [ARJ], and the estimated levator ani subtended volume [eLASV]) were investigated one year after surgery. Significance was established at p < 0.05.
After a mean 27-month follow-up, according to the MRI criteria, 60% of the women were cured in the VSF-AM group versus 45% in ASC group (p= 0.52). The POP-Q and objective cure rates by MRI were correlated in the anterior vaginal wall (p= 0.007), but no correlationwas foundwith the subjective cure. The eLASVwas largeramongthe patients with surgical failure, and a cutoff of ≥ 33.5mm3 was associated with postoperative failure (area under the receiver operating characteristic curve [ROC]: 0.813; p= 0.002).
Both surgeries for prolapse were similar regarding theobjective variables (POP-Q measurements and MRI cure rates). Larger eLASV areas were associated with surgical failure.
Summary
. 2021;43(1):9-13
We evaluated risk factors to determine if there were specific risk factors that could predict massive bleeding in nulliparous women with placenta previa.
The participants were classified into two groups. Women with a calculated blood loss ≥ 1,000mL were included in the massive bleeding group. Women without any signs or symptoms related with hypovolemia or with a calculated bleeding volume < 1,000 mL were categorized into the non-massive bleeding group.
There were 28 patients (40.6%) with massive bleeding and 41 cases (59.4%) with non-massive bleeding. The calculated blood loss and number of cases that required red cell transfusions were statistically different between the groups (< 0.005 and 0.002, respectively). There were no statistically significant differences in terms of maternal or fetal factors, placental location, or delivery characteristics between the two groups.
We could not determine the predictive features for massive hemorrhage based on clinical features, delivery features, or placental location.
Summary
. 2021;43(1):9-13
We evaluated risk factors to determine if there were specific risk factors that could predict massive bleeding in nulliparous women with placenta previa.
The participants were classified into two groups. Women with a calculated blood loss ≥ 1,000mL were included in the massive bleeding group. Women without any signs or symptoms related with hypovolemia or with a calculated bleeding volume < 1,000 mL were categorized into the non-massive bleeding group.
There were 28 patients (40.6%) with massive bleeding and 41 cases (59.4%) with non-massive bleeding. The calculated blood loss and number of cases that required red cell transfusions were statistically different between the groups (< 0.005 and 0.002, respectively). There were no statistically significant differences in terms of maternal or fetal factors, placental location, or delivery characteristics between the two groups.
We could not determine the predictive features for massive hemorrhage based on clinical features, delivery features, or placental location.
Summary
. 2021;43(2):113-118
To identify risk factors related to postpartum hemorrhage (PPH) and severe PPH with blood loss quantified objectively.
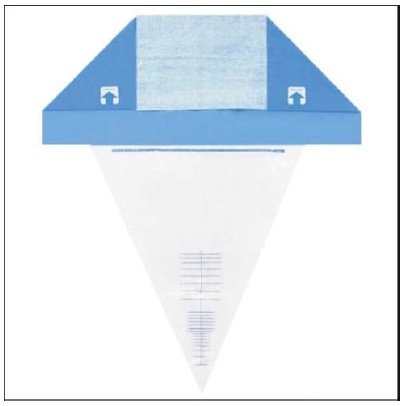
This is a complementary analysis of a prospective cohort study that included pregnant women delivering vaginally. The total blood loss was obtained through the sum of the volume collected from the drape with the weight of gauzes, compresses and pads used by women within 2 hours. Exploratory data analysis was performed to assess mean, standard deviation (SD), frequency, percentage and percentiles. The risk factors for postpartum bleeding were evaluated using linear and logistic regression.
We included 270 women. Themean blood loss at 120 minutes was 427.49 mL (±335.57 mL). Thirty-one percent (84 women) bled > 500mL and 8.2% (22 women) bled > 1,000 mL within 2 hours. Episiotomy, longer second stage of labor and forceps delivery were related to blood loss > 500mL within 2 hours, in the univariate analysis. In the multivariate analysis, only forceps remained associated with bleeding > 500 mL within 2 hours (odds ratio [OR] = 9.5 [2.85-31.53]). Previous anemia and episiotomy were also related to blood loss > 1,000mL.
Prolonged second stage of labor, forceps and episiotomy are related to increased incidence of PPH, and should be used as an alert for the delivery assistants for early recognition and prompt treatment for PPH.
Summary
. 2021;43(2):113-118
To identify risk factors related to postpartum hemorrhage (PPH) and severe PPH with blood loss quantified objectively.
This is a complementary analysis of a prospective cohort study that included pregnant women delivering vaginally. The total blood loss was obtained through the sum of the volume collected from the drape with the weight of gauzes, compresses and pads used by women within 2 hours. Exploratory data analysis was performed to assess mean, standard deviation (SD), frequency, percentage and percentiles. The risk factors for postpartum bleeding were evaluated using linear and logistic regression.
We included 270 women. Themean blood loss at 120 minutes was 427.49 mL (±335.57 mL). Thirty-one percent (84 women) bled > 500mL and 8.2% (22 women) bled > 1,000 mL within 2 hours. Episiotomy, longer second stage of labor and forceps delivery were related to blood loss > 500mL within 2 hours, in the univariate analysis. In the multivariate analysis, only forceps remained associated with bleeding > 500 mL within 2 hours (odds ratio [OR] = 9.5 [2.85-31.53]). Previous anemia and episiotomy were also related to blood loss > 1,000mL.
Prolonged second stage of labor, forceps and episiotomy are related to increased incidence of PPH, and should be used as an alert for the delivery assistants for early recognition and prompt treatment for PPH.
Summary
. 2021;43(2):119-125
To investigate whether follicular fluid (FF) from infertile women with mild endometriosis (ME) alters in vitro bovine embryo development, and whether the antioxidants N-acetyl-cysteine (NAC) and/or L-carnitine (LC) could prevent such damages.
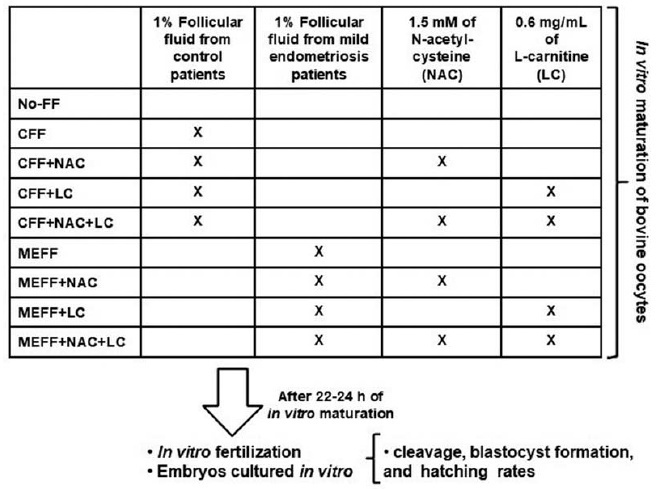
Follicular fluid was obtained from infertile women (11 with ME and 11 control). Bovine oocytes were matured in vitro divided in: No-FF, with 1% of FF from control women (CFF) or ME women (MEFF); with 1.5mM NAC (CFF + NAC, MEFF + NAC), with 0.6mg/mL LC (CFF + LC, MEFF + LC), or both antioxidants (CFF + NAC + LC, MEFF + NAC + LC). After in vitro fertilization, in vitro embryo culture was performed for 9 days.
A total of 883 presumptive zygotes were cultured in vitro. No differences were observed in cleavage rate (p = 0.5376) and blastocyst formation rate (p = 0.4249). However, the MEFF group (12.5%) had lower hatching rate than the No-FF (42.1%, p = 0.029) and CFF (42.9%, p = 0.036) groups. Addition of antioxidants in the group with CFF did not alter hatching rate (p ≥ 0.56), and in groups with MEFF, just NAC increased the hatching rate [(MEFF: 12.5% versus MEFF + NAC: 44.4% (p = 0.02); vs MEFF + LC: 18.8% (p = 0.79); versus MEFF + NAC + LC: 30.8% (p = 0.22)].
Therefore, FF from infertile women with ME added to medium of in vitro maturation of bovine oocytes impairs hatching rate, and NAC prevented these damages, suggesting involvement of oxidative stress in worst of oocyte and embryo quality of women with ME.
Summary
. 2021;43(2):119-125
To investigate whether follicular fluid (FF) from infertile women with mild endometriosis (ME) alters in vitro bovine embryo development, and whether the antioxidants N-acetyl-cysteine (NAC) and/or L-carnitine (LC) could prevent such damages.
Follicular fluid was obtained from infertile women (11 with ME and 11 control). Bovine oocytes were matured in vitro divided in: No-FF, with 1% of FF from control women (CFF) or ME women (MEFF); with 1.5mM NAC (CFF + NAC, MEFF + NAC), with 0.6mg/mL LC (CFF + LC, MEFF + LC), or both antioxidants (CFF + NAC + LC, MEFF + NAC + LC). After in vitro fertilization, in vitro embryo culture was performed for 9 days.
A total of 883 presumptive zygotes were cultured in vitro. No differences were observed in cleavage rate (p = 0.5376) and blastocyst formation rate (p = 0.4249). However, the MEFF group (12.5%) had lower hatching rate than the No-FF (42.1%, p = 0.029) and CFF (42.9%, p = 0.036) groups. Addition of antioxidants in the group with CFF did not alter hatching rate (p ≥ 0.56), and in groups with MEFF, just NAC increased the hatching rate [(MEFF: 12.5% versus MEFF + NAC: 44.4% (p = 0.02); vs MEFF + LC: 18.8% (p = 0.79); versus MEFF + NAC + LC: 30.8% (p = 0.22)].
Therefore, FF from infertile women with ME added to medium of in vitro maturation of bovine oocytes impairs hatching rate, and NAC prevented these damages, suggesting involvement of oxidative stress in worst of oocyte and embryo quality of women with ME.
Summary
. 2021;43(3):158-164
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
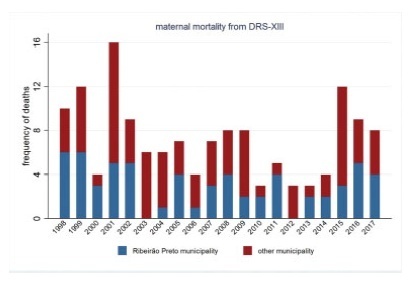
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
. 2021;43(3):158-164
To describe the evolution of maternal mortality right after the establishment of maternal death committees in the region of the city of Ribeirão Preto, state of São Paulo, Brazil.
The present study describes the spatial and temporal distribution of maternal mortality frequencies and rates, using data from the state of São Paulo, the municipality of Ribeirão Preto, and its Regional Health Department (DRS-XIII) from 1998 to 2017. The present ecological study considered the maternal mortality and live birth frequencies made available by the Computer Science Department of the Brazilian Unified Health System (Departamento de Informática do Sistema Único de Saúde, DATASUS, in the Portuguese acronym)/Ministry of Health, which were grouped by year and political-administrative division (the state of São Paulo, the DRS-XIII, and the city of Ribeirão Preto). The maternal mortality rate (MMR) was calculated and presented through descriptive measures, graphs, and cartograms.
The overall MMR observed for the city of Ribeirão Preto was of 39.1; for the DRS-XIII, it was of of 40.4; and for the state of São Paulo, it was of 43.8 for every 100 thousand live birhts. During this period, the MMR for the city of Ribeirão Preto ranged from 0% to 80% of the total maternal mortalities, and from 40.7% to 47.2% of live births in the DRS-XIII. The city of Ribeirao Preto had an MMR of 76.5 in 1998and 1999, which decreased progressively to 12.1 until the years of 2012 and 2013, and increased to 54.3 for every 100 thousand live births over the past 4 years. The state of São Paulo State had an MMR of 54.0 in 1998-1999, which varied throughout the study period, with values pregnancy of 48.0 in 2008-2009, and 54.1 for every 100 thousand live births in 2016-2017. Several times before 2015, the city of Ribeirão Preto and the DRS-XIII reached the Millennium Goals. Recently, however, the MMR increased, which can be explained by the improvement in the surveillance of maternal mortality.
The present study describes a sharp decline in maternal death in the region of Ribeirão Preto by the end of 2012-2013, and a subsequent and distressing increase in recent years that needs to be fully faced.
Summary
. 2021;43(2):107-112
To evaluate the obstetric and sociodemographic characteristics of gestational diabetic women who maintained hyperglycemia in the postpartum period (6-12 weeks postpartum).
This is a longitudinal cohort study with women who have had gestational diabetes and/or macrosomic children between March 1st, 2016 and March 1st, 2017. Between 6 and 12 weeks after birth, women who had gestational diabetes collected fasting glycemia, glucose tolerance test, and glycated hemoglobin results. The data were collected from medical records and during an interview in the first postpartum consultation. A statistical analysis was performed using frequency, percentage, Chi- Squared test, Fisher exact test, Mann-Whitney test, and multivariate Poisson regression. The significance level adopted for the statistical tests was 5%.
One hundred and twenty-two women were included. Most of the women were younger than 35 years old (70.5%), white, multiparous, and with no history of gestational diabetes. Thirteen percent of the participants developed persistent hyperglycemia. A univariate analysis showed that maternal age above 35 years, being overweight, having grade 1 obesity and weight gain under 5 kg was related to the persistence of hyperglycemia in the postpartum period.
Maternal age above 35 years, obesity and overweight, and the diagnosis of gestational diabetes in the first trimester of pregnancy are associated with hyperglycemia during the postpartum period.
Summary
. 2021;43(2):107-112
To evaluate the obstetric and sociodemographic characteristics of gestational diabetic women who maintained hyperglycemia in the postpartum period (6-12 weeks postpartum).
This is a longitudinal cohort study with women who have had gestational diabetes and/or macrosomic children between March 1st, 2016 and March 1st, 2017. Between 6 and 12 weeks after birth, women who had gestational diabetes collected fasting glycemia, glucose tolerance test, and glycated hemoglobin results. The data were collected from medical records and during an interview in the first postpartum consultation. A statistical analysis was performed using frequency, percentage, Chi- Squared test, Fisher exact test, Mann-Whitney test, and multivariate Poisson regression. The significance level adopted for the statistical tests was 5%.
One hundred and twenty-two women were included. Most of the women were younger than 35 years old (70.5%), white, multiparous, and with no history of gestational diabetes. Thirteen percent of the participants developed persistent hyperglycemia. A univariate analysis showed that maternal age above 35 years, being overweight, having grade 1 obesity and weight gain under 5 kg was related to the persistence of hyperglycemia in the postpartum period.
Maternal age above 35 years, obesity and overweight, and the diagnosis of gestational diabetes in the first trimester of pregnancy are associated with hyperglycemia during the postpartum period.