Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(4):201-206
To evaluate recurrence rates and risk factors among women with stage IA1 cervical cancer without lymph vascular space invasion managed conservatively.
retrospective review of women with stage IA1 squamous cervical cancer who underwent cold knife cone or loop electrosurgical excision procedure, between 1994 and 2015, at a gynecologic oncology center in Southern Brazil. Age at diagnosis, pre-conization findings, conization method, margin status, residual disease, recurrence and survival rates were collected and analyzed.
26 women diagnosed with stage IA1 squamous cervical cancer without lymphovascular space invasion underwent conservative management and had at least 12 months follow-up. The mean follow-up was 44.6 months. The mean age at diagnosis was 40.9 years. Median first intercourse occurred at age 16 years, 11.5% were nulliparous and 30.8% were current or past tobacco smokers. There was one Human immunodeficiency virus positive patient diagnosed with cervical intraepithelial neoplasia grade 2 at 30 months after surgery. However, there were no patients diagnosed with recurrent invasive cervical cancer and there were no deaths due to cervical cancer or other causes in the cohort.
Excellent outcomes were noted in women with stage IA1 cervical cancer without lymphovascular space invasion and with negative margins who were managed conservatively, even in a developing country.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):11-20
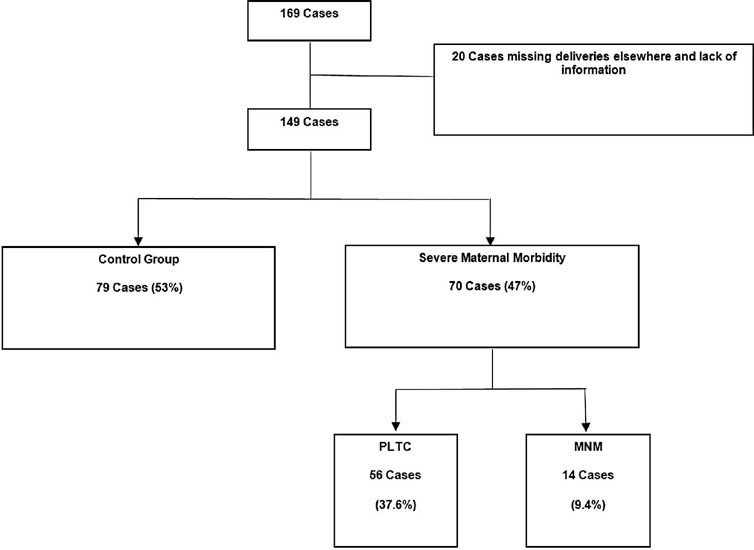
Systemic lupus erythematosus (SLE) may cause irreversible organ damage. Pregnancy with SLE may have severe life-threatening risks. The present study aimed to determine the prevalence of severe maternal morbidity (SMM) in patients with SLE and analyze the parameters that contributed to cases of greater severity.
This is a cross-sectional retrospective study from analysis of data retrieved from medical records of pregnant women with SLE treated at a University Hospital in Brazil. The pregnant women were divided in a control group without complications, a group with potentially life-threatening conditions (PLTC), and a group with maternal near miss (MNM).
The maternal near miss rate was 112.9 per 1,000 live births. The majority of PLTC (83.9%) and MNM (92.9%) cases had preterm deliveries with statistically significant increased risk compared with the control group (p = 0.0042; odds ratio [OR]: 12.05; 95% confidence interval [CI]: 1.5–96.6 for the MNM group and p = 0.0001; OR: 4.84; 95%CI: 2.2–10.8 for the PLTC group). Severe maternal morbidity increases the risk of longer hospitalization (p < 0.0001; OR: 18.8; 95%CI: 7.0–50.6 and p < 0.0001; OR: 158.17; 95%CI: 17.6–1424,2 for the PLTC and MNM groups, respectively), newborns with low birthweight (p = 0.0006; OR: 3.67; 95%CI: 1.7–7.9 and p = 0.0009; OR: 17.68; 95%CI: 2–153.6) for the PLTC and MNM groups, respectively] as well as renal diseases (PLTC [8.9%; 33/56; p = 0.0069] and MNM [78.6%; 11/14; p = 0.0026]). Maternal near miss cases presented increased risk for neonatal death (p = 0.0128; OR: 38.4; 95%CI: 3.3–440.3]), and stillbirth and miscarriage (p = 0.0011; OR: 7.68; 95%CI: 2.2–26.3]).
Systemic lupus erythematosus was significantly associated with severe maternal morbidity, longer hospitalizations, and increased risk of poor obstetric and neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):11-20
Systemic lupus erythematosus (SLE) may cause irreversible organ damage. Pregnancy with SLE may have severe life-threatening risks. The present study aimed to determine the prevalence of severe maternal morbidity (SMM) in patients with SLE and analyze the parameters that contributed to cases of greater severity.
This is a cross-sectional retrospective study from analysis of data retrieved from medical records of pregnant women with SLE treated at a University Hospital in Brazil. The pregnant women were divided in a control group without complications, a group with potentially life-threatening conditions (PLTC), and a group with maternal near miss (MNM).
The maternal near miss rate was 112.9 per 1,000 live births. The majority of PLTC (83.9%) and MNM (92.9%) cases had preterm deliveries with statistically significant increased risk compared with the control group (p = 0.0042; odds ratio [OR]: 12.05; 95% confidence interval [CI]: 1.5–96.6 for the MNM group and p = 0.0001; OR: 4.84; 95%CI: 2.2–10.8 for the PLTC group). Severe maternal morbidity increases the risk of longer hospitalization (p < 0.0001; OR: 18.8; 95%CI: 7.0–50.6 and p < 0.0001; OR: 158.17; 95%CI: 17.6–1424,2 for the PLTC and MNM groups, respectively), newborns with low birthweight (p = 0.0006; OR: 3.67; 95%CI: 1.7–7.9 and p = 0.0009; OR: 17.68; 95%CI: 2–153.6) for the PLTC and MNM groups, respectively] as well as renal diseases (PLTC [8.9%; 33/56; p = 0.0069] and MNM [78.6%; 11/14; p = 0.0026]). Maternal near miss cases presented increased risk for neonatal death (p = 0.0128; OR: 38.4; 95%CI: 3.3–440.3]), and stillbirth and miscarriage (p = 0.0011; OR: 7.68; 95%CI: 2.2–26.3]).
Systemic lupus erythematosus was significantly associated with severe maternal morbidity, longer hospitalizations, and increased risk of poor obstetric and neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):03-10
To evaluate the association between pain intensity in the active phase of the first stage of labor with the use or not of nonpharmacological methods for pain relief in a real-life scenario.
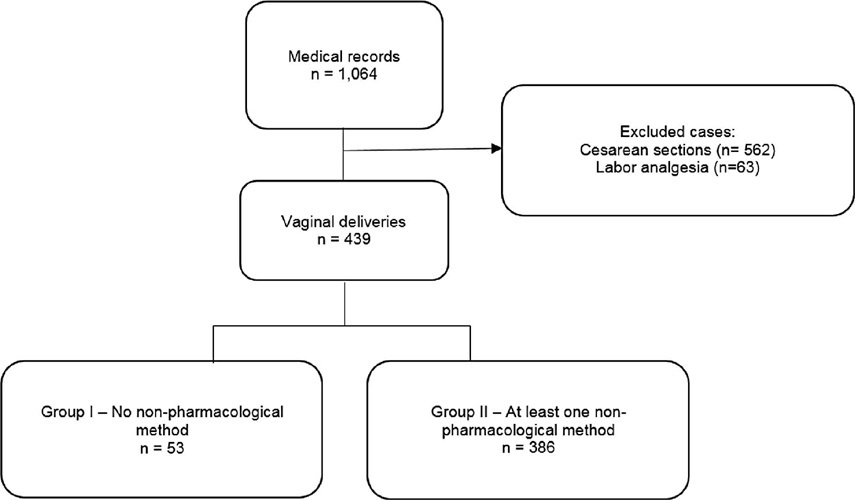
This was an observational cross-sectional study. The variables analyzed were obtained by a questionnaire with the mothers (up to 48 hours postpartum) to investigate the intensity of pain during labor using the visual analog scale (VAS). The nonpharmacological pain relief methods routinely used in obstetric practice were evaluated by consulting medical records. The patients were separated into two groups: Group I – patients who did not use nonpharmacological methods for pain relief and Group II –patients who used these methods.
A total of 439 women who underwent vaginal delivery were included; 386 (87.9%) used at least 1 nonpharmacological method and 53 (12.1%) did not. The women who did not use nonpharmacological methods had significantly lower gestational age (37.2 versus 39.6 weeks, p < 0.001) and shorter duration of labor (24 versus 114 min, p < 0.001) than those who used the methods. There was no statistically significant difference in the pain scale score using the VAS between the group that used nonpharmacological methods and the group that did not (median 10 [minimum 2– maximum 10] versus 10 [minimum 6–maximum 10] p = 0.334).
In a real-life setting, there was no difference in labor pain intensity between the patients who used nonpharmacological methods and those who did not use them during the active phase of labor.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):03-10
To evaluate the association between pain intensity in the active phase of the first stage of labor with the use or not of nonpharmacological methods for pain relief in a real-life scenario.
This was an observational cross-sectional study. The variables analyzed were obtained by a questionnaire with the mothers (up to 48 hours postpartum) to investigate the intensity of pain during labor using the visual analog scale (VAS). The nonpharmacological pain relief methods routinely used in obstetric practice were evaluated by consulting medical records. The patients were separated into two groups: Group I – patients who did not use nonpharmacological methods for pain relief and Group II –patients who used these methods.
A total of 439 women who underwent vaginal delivery were included; 386 (87.9%) used at least 1 nonpharmacological method and 53 (12.1%) did not. The women who did not use nonpharmacological methods had significantly lower gestational age (37.2 versus 39.6 weeks, p < 0.001) and shorter duration of labor (24 versus 114 min, p < 0.001) than those who used the methods. There was no statistically significant difference in the pain scale score using the VAS between the group that used nonpharmacological methods and the group that did not (median 10 [minimum 2– maximum 10] versus 10 [minimum 6–maximum 10] p = 0.334).
In a real-life setting, there was no difference in labor pain intensity between the patients who used nonpharmacological methods and those who did not use them during the active phase of labor.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):21-30
To evaluate the rates of precancerous lesions, colposcopy referral, and positive predictive value (PPV) by age groups of a population-based screening with DNA-HPV testing.
The present demonstration study compared 16,384 HPV tests performed in the first 30 months of the program with 19,992 women tested in the cytology screening. The colposcopy referral rate and PPV for CIN2+ and CIN3+ by age group and screening program were compared. The statistical analysis used the chi-squared test and odds ratio (OR) with 95% confidence interval (95%CI).
The HPV tests were 3.26% positive for HPV16-HPV18 and 9.92% positive for 12 other HPVs with a 3.7 times higher colposcopy referral rate than the cytology program, which had 1.68% abnormalities. Human Papillomavirus testing detected 103 CIN2, 89 CIN3, and one AIS, compared with 24 CIN2 and 54 CIN3 detected by cytology (p < 0.0001). The age group between 25 and 29 years old screened by HPV testing had 2.4 to 3.0 times more positivity, 13.0% colposcopy referral, twice more than women aged 30 to 39 years old (7.7%; p < 0.0001), and detected 20 CIN3 and 3 early-stage cancer versus 9 CIN3 and no cancer by cytology screening (CIN3 OR= 2.10; 95%CI: 0.91 -5.25; p = 0.043). The PPV of colposcopy for CIN2+ ranged from 29.5 to 41.0% in the HPV testing program.
There was a significant increase in detections of cervix precancerous lesions in a short period of screening with HPV testing. In women < 30 years old, the HPV testing exhibited more positivity, high colposcopy referral rate, similar colposcopy PPV to older women, and more detection of HSIL and early-stage cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):21-30
To evaluate the rates of precancerous lesions, colposcopy referral, and positive predictive value (PPV) by age groups of a population-based screening with DNA-HPV testing.
The present demonstration study compared 16,384 HPV tests performed in the first 30 months of the program with 19,992 women tested in the cytology screening. The colposcopy referral rate and PPV for CIN2+ and CIN3+ by age group and screening program were compared. The statistical analysis used the chi-squared test and odds ratio (OR) with 95% confidence interval (95%CI).
The HPV tests were 3.26% positive for HPV16-HPV18 and 9.92% positive for 12 other HPVs with a 3.7 times higher colposcopy referral rate than the cytology program, which had 1.68% abnormalities. Human Papillomavirus testing detected 103 CIN2, 89 CIN3, and one AIS, compared with 24 CIN2 and 54 CIN3 detected by cytology (p < 0.0001). The age group between 25 and 29 years old screened by HPV testing had 2.4 to 3.0 times more positivity, 13.0% colposcopy referral, twice more than women aged 30 to 39 years old (7.7%; p < 0.0001), and detected 20 CIN3 and 3 early-stage cancer versus 9 CIN3 and no cancer by cytology screening (CIN3 OR= 2.10; 95%CI: 0.91 -5.25; p = 0.043). The PPV of colposcopy for CIN2+ ranged from 29.5 to 41.0% in the HPV testing program.
There was a significant increase in detections of cervix precancerous lesions in a short period of screening with HPV testing. In women < 30 years old, the HPV testing exhibited more positivity, high colposcopy referral rate, similar colposcopy PPV to older women, and more detection of HSIL and early-stage cervical cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):31-37
To evaluate the expulsion and continuation rates of the copper intrauterine device (IUD) inserted in the immediate postpartum period in a Brazilian public university hospital.
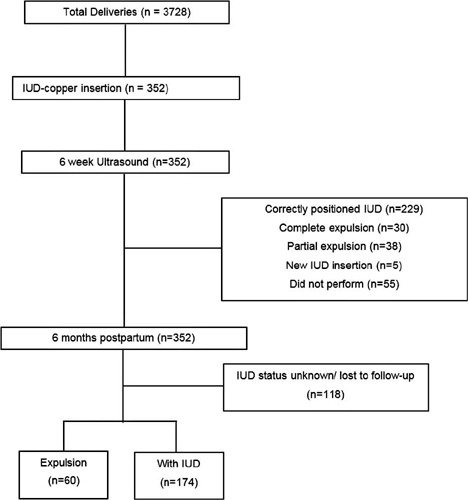
In the present cohort study, we included women who received immediate postpartum IUD at vaginal delivery or cesarean s March 2018 to December 2019. Clinical data and the findings of transvaginal ultrasound (US) scans performed 6-weeks postpartum were collected. The expulsion and continuation rates were assessed 6-months postpartum using data from the electronic medical records or by telephone contact. The primary outcome was the proportion of IUDs expelled at 6 months. For the statistical analysis, we used the Student t-test, the Poisson distribution, and the Chi-squared test.
There were 3,728 births in the period, and 352 IUD insertions were performed, totaling a rate of 9.4%. At 6 weeks postpartum, the IUD was properly positioned in 65.1% of the cases, in 10.8% there was partial expulsion, and in 8.5% it had been completely expelled. At 6 months postpartum, information was obtained from 234 women, 74.4% of whom used IUD, with an overall expulsion rate of 25.6%. The expulsion rate was higher after vaginal delivery when compared with cesarean section (68.4% versus 31.6% respectively; p = 0.031). There were no differences in terms of age, parity, gestational age, final body mass index, and newborn weight.
Despite the low insertion rate of copper IUDs in the postpartum period and a higher expulsion rate, the rate of long-term continuation of intrauterine contraception was high, indicating that it is a useful intervention to prevent unwanted pregnancies and to reduce short-interval birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):31-37
To evaluate the expulsion and continuation rates of the copper intrauterine device (IUD) inserted in the immediate postpartum period in a Brazilian public university hospital.
In the present cohort study, we included women who received immediate postpartum IUD at vaginal delivery or cesarean s March 2018 to December 2019. Clinical data and the findings of transvaginal ultrasound (US) scans performed 6-weeks postpartum were collected. The expulsion and continuation rates were assessed 6-months postpartum using data from the electronic medical records or by telephone contact. The primary outcome was the proportion of IUDs expelled at 6 months. For the statistical analysis, we used the Student t-test, the Poisson distribution, and the Chi-squared test.
There were 3,728 births in the period, and 352 IUD insertions were performed, totaling a rate of 9.4%. At 6 weeks postpartum, the IUD was properly positioned in 65.1% of the cases, in 10.8% there was partial expulsion, and in 8.5% it had been completely expelled. At 6 months postpartum, information was obtained from 234 women, 74.4% of whom used IUD, with an overall expulsion rate of 25.6%. The expulsion rate was higher after vaginal delivery when compared with cesarean section (68.4% versus 31.6% respectively; p = 0.031). There were no differences in terms of age, parity, gestational age, final body mass index, and newborn weight.
Despite the low insertion rate of copper IUDs in the postpartum period and a higher expulsion rate, the rate of long-term continuation of intrauterine contraception was high, indicating that it is a useful intervention to prevent unwanted pregnancies and to reduce short-interval birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):38-42
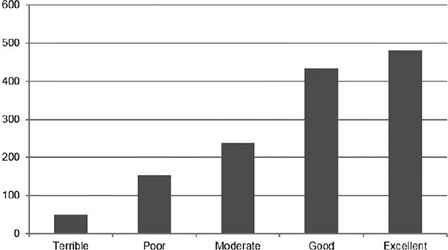
Pain is the primary limitation to performing hysteroscopy. We aimed to evaluate the predictive factors of low tolerance to office hysteroscopic procedures. Methods Retrospective cohort study of the patients who underwent office hysteroscopy from January 2018 to December 2020 at a tertiary care center. Pain tolerance to office-based hysteroscopy was subjectively assessed by the operator as terrible, poor, moderate, good, or excellent. Categorical variables were compared with the use of the Chi-squared test; an independent-samples t-test was conducted to compare continuous variables. Logistic regression was performed to determine the main factors associated with low procedure tolerance.
A total of 1,418 office hysteroscopies were performed. The mean age of the patients was 53 ± 13.8 years; 50.8% of women were menopausal, 17.8% were nulliparous, and 68.7% had a previous vaginal delivery. A total of 42.6% of women were submitted to an operative hysteroscopy. Tolerance was categorized as terrible or poor in 14.9% of hysteroscopies and moderate, good, or excellent in 85.1%. A terrible or poor tolerance was more frequently reported in menopausal women (18.1% vs. 11.7% in premenopausal women, p = 0.001) and women with no previous vaginal delivery (18.8% vs. 12.9% in women with at least one vaginal birth, p = 0.007). Low tolerance led more often to scheduling a second hysteroscopic procedure under anesthesia (56.4% vs. 17.5% in reasonable-to-excellent tolerance, p < 0.0005).
Office hysteroscopy was a well-tolerated procedure in our experience, but menopause and lack of previous vaginal delivery were associated with low tolerance. These patients are more likely to benefit from pain relief measures during office hysteroscopy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(1):38-42
Pain is the primary limitation to performing hysteroscopy. We aimed to evaluate the predictive factors of low tolerance to office hysteroscopic procedures. Methods Retrospective cohort study of the patients who underwent office hysteroscopy from January 2018 to December 2020 at a tertiary care center. Pain tolerance to office-based hysteroscopy was subjectively assessed by the operator as terrible, poor, moderate, good, or excellent. Categorical variables were compared with the use of the Chi-squared test; an independent-samples t-test was conducted to compare continuous variables. Logistic regression was performed to determine the main factors associated with low procedure tolerance.
A total of 1,418 office hysteroscopies were performed. The mean age of the patients was 53 ± 13.8 years; 50.8% of women were menopausal, 17.8% were nulliparous, and 68.7% had a previous vaginal delivery. A total of 42.6% of women were submitted to an operative hysteroscopy. Tolerance was categorized as terrible or poor in 14.9% of hysteroscopies and moderate, good, or excellent in 85.1%. A terrible or poor tolerance was more frequently reported in menopausal women (18.1% vs. 11.7% in premenopausal women, p = 0.001) and women with no previous vaginal delivery (18.8% vs. 12.9% in women with at least one vaginal birth, p = 0.007). Low tolerance led more often to scheduling a second hysteroscopic procedure under anesthesia (56.4% vs. 17.5% in reasonable-to-excellent tolerance, p < 0.0005).
Office hysteroscopy was a well-tolerated procedure in our experience, but menopause and lack of previous vaginal delivery were associated with low tolerance. These patients are more likely to benefit from pain relief measures during office hysteroscopy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(12):1083-1089
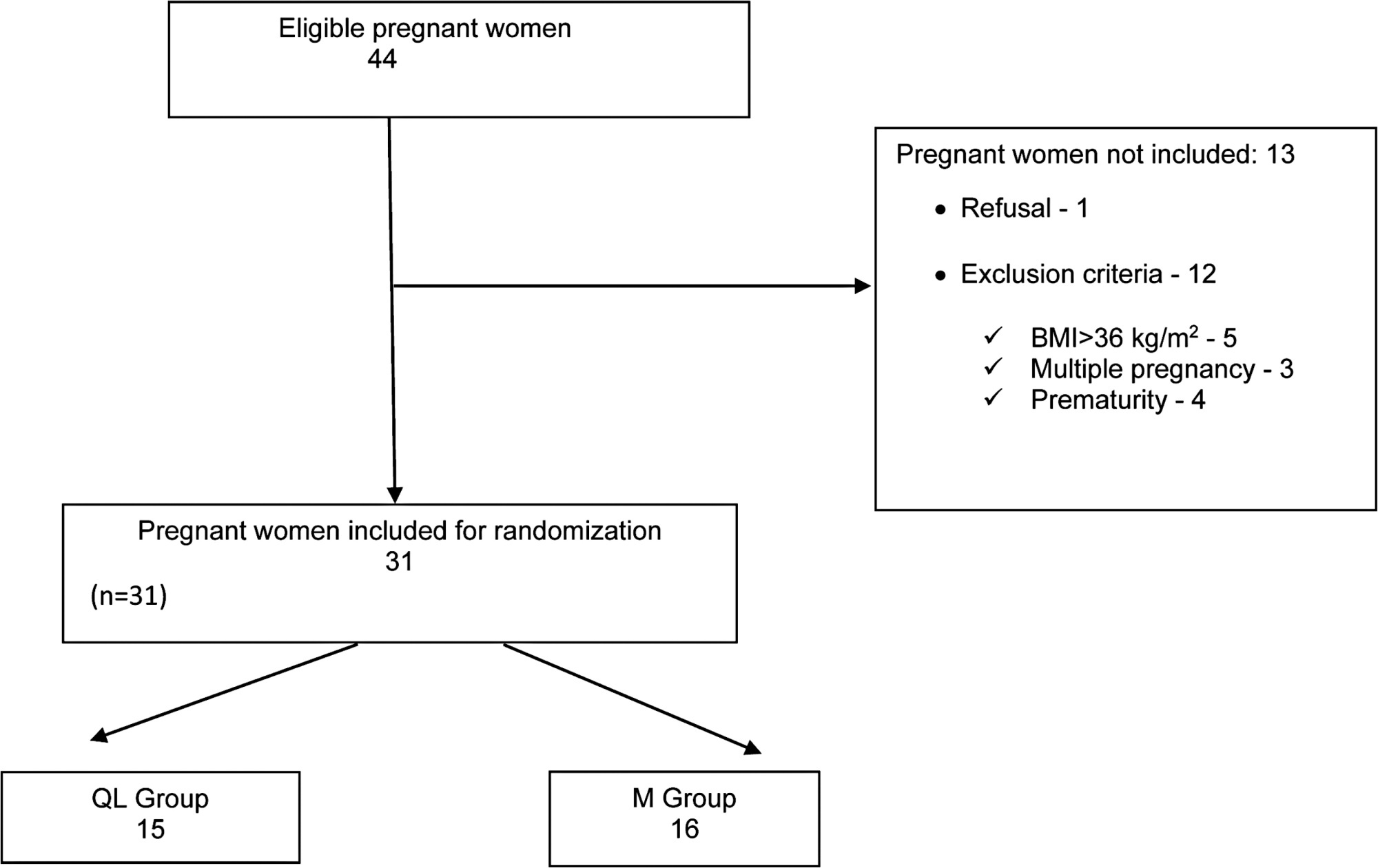
To compare the efficacy of quadratus lumborum (QL) block and intrathecal morphine (M) for postcesarean delivery analgesia.
Thirty-one pregnant women with ≥ 37 weeks of gestation submitted to elective cesarean section were included in the study. They were randomly allocated to either the QL group (12.5 mg 0.5% bupivacaine for spinal anesthesia and 0.3 ml/kg 0.2% bupivacaine for QL block) or the M group (12.5 mg bupivacaine 0.5% and 100 mcg of morphine in spinal anesthesia). The visual analog scale of pain, consumption of morphine and tramadol for pain relief in 48 hours, and side effects were recorded.
Median pain score and/or pain variation were higher in the morphine group than in the QL group (p = 0.02). There was no significant difference in the consumption of morphine or tramadol between groups over time. Side effects such as pruritus, nausea, and vomiting were observed only in the morphine group.
Quadratus lumborum block and intrathecal morphine are effective for analgesia after cesarean section. Patients undergoing QL block had lower postoperative pain scores without the undesirable side effects of opioids such as nausea, vomiting, and pruritus.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(12):1083-1089
To compare the efficacy of quadratus lumborum (QL) block and intrathecal morphine (M) for postcesarean delivery analgesia.
Thirty-one pregnant women with ≥ 37 weeks of gestation submitted to elective cesarean section were included in the study. They were randomly allocated to either the QL group (12.5 mg 0.5% bupivacaine for spinal anesthesia and 0.3 ml/kg 0.2% bupivacaine for QL block) or the M group (12.5 mg bupivacaine 0.5% and 100 mcg of morphine in spinal anesthesia). The visual analog scale of pain, consumption of morphine and tramadol for pain relief in 48 hours, and side effects were recorded.
Median pain score and/or pain variation were higher in the morphine group than in the QL group (p = 0.02). There was no significant difference in the consumption of morphine or tramadol between groups over time. Side effects such as pruritus, nausea, and vomiting were observed only in the morphine group.
Quadratus lumborum block and intrathecal morphine are effective for analgesia after cesarean section. Patients undergoing QL block had lower postoperative pain scores without the undesirable side effects of opioids such as nausea, vomiting, and pruritus.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(12):1090-1093
To describe the clinical results of patients admitted and managed as cases of placenta accreta spectrum (PAS) at a Central American public hospital and the influence of the prenatal diagnosis on the condition.
A retrospective analysis of PAS patients treated at Hospital Bertha Calderón Roque, in Managua, Nicaragua, between June 2017 and September 2021. The diagnostic criteria used were those of the International Federation of Gynecology and Obstetrics (Fédération Internationale de Gynécologie et d'Obstétrique, FIGO, in French). The population was divided into patients with a prenatal ultrasonographic diagnosis of PAS (group 1) and those whose the diagnosis of PAS was established at the time of the caesarean section (group 2).
During the search, we found 103 cases with a histological and/or clinical diagnosis of PAS; groups 1 and 2 were composed of 51 and 52 patients respectively. Regarding the clinical results of both groups, the patients in group 1 presented a lower frequency of transfusions (56.9% versus 96.1% in group 2), use of a lower number of red blood cell units (RBCUs) among those undergoing transfusions (median: 1; interquartile range: [IQR]: 0–4 versus median: 3; [IQR]: 2–4] in group 2), and lower frequency of 4 or more RBCU transfusions (29.4% versus 46.1% in group 2). Group 1 also exhibited a non-significant trend toward a lower volume of blood loss (1,000 mL [IQR]: 750–2,000 mL versus 1,500 mL [IQR]: 1,200–1,800 mL in group 2), and lower requirement of pelvic packing (1.9% versus 7.7% in group 2).
Establishing a prenatal diagnosis of PAS is related to a lower frequency of transfusions. We observed a high frequency of prenatal diagnostic failures of PAS. It is a priority to improve prenatal detection of this disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(12):1090-1093
To describe the clinical results of patients admitted and managed as cases of placenta accreta spectrum (PAS) at a Central American public hospital and the influence of the prenatal diagnosis on the condition.
A retrospective analysis of PAS patients treated at Hospital Bertha Calderón Roque, in Managua, Nicaragua, between June 2017 and September 2021. The diagnostic criteria used were those of the International Federation of Gynecology and Obstetrics (Fédération Internationale de Gynécologie et d'Obstétrique, FIGO, in French). The population was divided into patients with a prenatal ultrasonographic diagnosis of PAS (group 1) and those whose the diagnosis of PAS was established at the time of the caesarean section (group 2).
During the search, we found 103 cases with a histological and/or clinical diagnosis of PAS; groups 1 and 2 were composed of 51 and 52 patients respectively. Regarding the clinical results of both groups, the patients in group 1 presented a lower frequency of transfusions (56.9% versus 96.1% in group 2), use of a lower number of red blood cell units (RBCUs) among those undergoing transfusions (median: 1; interquartile range: [IQR]: 0–4 versus median: 3; [IQR]: 2–4] in group 2), and lower frequency of 4 or more RBCU transfusions (29.4% versus 46.1% in group 2). Group 1 also exhibited a non-significant trend toward a lower volume of blood loss (1,000 mL [IQR]: 750–2,000 mL versus 1,500 mL [IQR]: 1,200–1,800 mL in group 2), and lower requirement of pelvic packing (1.9% versus 7.7% in group 2).
Establishing a prenatal diagnosis of PAS is related to a lower frequency of transfusions. We observed a high frequency of prenatal diagnostic failures of PAS. It is a priority to improve prenatal detection of this disease.