Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):174-181
DOI 10.1590/S0100-72032011000800002
PURPOSE: To describe the maternal and perinatal outcomes of pregnant women diagnosed with leukemia who were followed up for prenatal care and delivery at a university hospital. METHODS: A retrospective study of the period from 2001 to 2011, which included 16 pregnant women with a diagnosis of leukemia followed by antenatal care specialists in hematological diseases and pregnancy. For acute leukemia diagnosed after the first trimester, the recommendation was to perform chemotherapy despite the current pregnancy. For chronic leukemia, patients who were controlled in hematological terms were maintained without medication during pregnancy, or chemotherapy was introduced after the first trimester. We analyzed the maternal and perinatal outcome. RESULTS: Acute lymphoblastic leukemia (ALL) was diagnosed in five cases (31.3%), acute myeloid leukemia (AML) in two cases (12.5%) and chronic myeloid leukemia (CML) in nine cases (56.3%). Of the cases of acute leukemia, two (28.6%) were diagnosed in the first trimester, two (28.6%) in the second and three (42.9%) in the third. Two patients with ALL diagnosed in the first trimester opted for therapeutic abortion. Four patients with acute leukemia received chemotherapy during pregnancy, with a diagnosis established after the 20th week. In one case of ALL with a late diagnosis (30 weeks), chemotherapy was started after delivery. All pregnant women with acute leukemia developed anemia and thrombocytopenia, and four (57.1%) developed febrile neutropenia. Of nine pregnant women with CML, four were treated with imatinib mesylate when they became pregnant, with treatment being interrupted in the first trimester in three of them and in the second trimester in one. During pregnancy, three patients (33.3%) required no chemotherapy after discontinuation of imatinib, and six (66.7%) were treated with the following drugs: interferon (n=5) and/or hydroxyurea (n=3 ). In the group of pregnant women with CML, anemia occurred in four (44.4%) cases and thrombocytopenia in one (11.1%). The perinatal outcomes of pregnancies complicated by acute leukemia were as follows: mean gestational age at delivery was 32 weeks (standard deviation - SD=4.4) and the mean birth weight was 1476 g (SD=657 g), there were 2 (40.0%) perinatal deaths (a fetal one and a neonatal one). In pregnancies complicated by CML, the mean gestational age at delivery was 37.6 weeks (SD=1.1) and the mean birth weight was 2870 g (SD=516 g). There was no perinatal death and no fetal abnormality was detected. CONCLUSIONS: Maternal and fetal morbidity is high in pregnancies complicated by acute leukemia. Whereas, in pregnancies complicated by CML, the maternal and fetal prognosis appears to be more favorable, with greater ease in management of complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):174-181
DOI 10.1590/S0100-72032011000800002
PURPOSE: To describe the maternal and perinatal outcomes of pregnant women diagnosed with leukemia who were followed up for prenatal care and delivery at a university hospital. METHODS: A retrospective study of the period from 2001 to 2011, which included 16 pregnant women with a diagnosis of leukemia followed by antenatal care specialists in hematological diseases and pregnancy. For acute leukemia diagnosed after the first trimester, the recommendation was to perform chemotherapy despite the current pregnancy. For chronic leukemia, patients who were controlled in hematological terms were maintained without medication during pregnancy, or chemotherapy was introduced after the first trimester. We analyzed the maternal and perinatal outcome. RESULTS: Acute lymphoblastic leukemia (ALL) was diagnosed in five cases (31.3%), acute myeloid leukemia (AML) in two cases (12.5%) and chronic myeloid leukemia (CML) in nine cases (56.3%). Of the cases of acute leukemia, two (28.6%) were diagnosed in the first trimester, two (28.6%) in the second and three (42.9%) in the third. Two patients with ALL diagnosed in the first trimester opted for therapeutic abortion. Four patients with acute leukemia received chemotherapy during pregnancy, with a diagnosis established after the 20th week. In one case of ALL with a late diagnosis (30 weeks), chemotherapy was started after delivery. All pregnant women with acute leukemia developed anemia and thrombocytopenia, and four (57.1%) developed febrile neutropenia. Of nine pregnant women with CML, four were treated with imatinib mesylate when they became pregnant, with treatment being interrupted in the first trimester in three of them and in the second trimester in one. During pregnancy, three patients (33.3%) required no chemotherapy after discontinuation of imatinib, and six (66.7%) were treated with the following drugs: interferon (n=5) and/or hydroxyurea (n=3 ). In the group of pregnant women with CML, anemia occurred in four (44.4%) cases and thrombocytopenia in one (11.1%). The perinatal outcomes of pregnancies complicated by acute leukemia were as follows: mean gestational age at delivery was 32 weeks (standard deviation - SD=4.4) and the mean birth weight was 1476 g (SD=657 g), there were 2 (40.0%) perinatal deaths (a fetal one and a neonatal one). In pregnancies complicated by CML, the mean gestational age at delivery was 37.6 weeks (SD=1.1) and the mean birth weight was 2870 g (SD=516 g). There was no perinatal death and no fetal abnormality was detected. CONCLUSIONS: Maternal and fetal morbidity is high in pregnancies complicated by acute leukemia. Whereas, in pregnancies complicated by CML, the maternal and fetal prognosis appears to be more favorable, with greater ease in management of complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):182-187
DOI 10.1590/S0100-72032011000800003
PURPOSE:to evaluate psychosocial adaptation to pregnancy by translating and cross-culturally adapting a specific assessment instrument to be used with Brazilian women. METHODS: this was a cross-sectional observational study. the translation and cross-cultural adaptation and of the Prenatal Self-evaluation Questionnaire (PSeQ) was performed following all the required methodological steps. another questionnaire was applied to characterize the sociodemographic and clinical status of the pregnant women (n=36). Statistical analysis consisted of the determination of the mean and standard deviation (SD) and of absolute and relative frequency. the statistical test used for the analysis of internal consistency was Cronbach's alpha coefficient, using SPSS version 17.0. RESULTS: the volunteers were of low socioeconomic status, aged on average 25.1 years ( 5.5), and had an average gestational age of 25.9 weeks ( 8.1). 58.3% of these volunteers had not planned their current pregnancy. the pretest showed that 75% of the pregnant women found the questionnaire easy to understand. Regarding the PSeQ instrument, the identification with the maternal role was the subcategory which showed the highest average, 24.8 ( 5.6), while the relationship with the mother had the lowest average 15.4 ( 7.7). the internal consistency ranged from 0.52 to 0.89. CONCLUSION: the assessment of psychosocial adaptation to pregnancy in pregnant women is very important during the progress of pregnancy and permits intervention through obstetric-neonatal actions of promotion and prevention regarding the well-being of mother and child.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):182-187
DOI 10.1590/S0100-72032011000800003
PURPOSE:to evaluate psychosocial adaptation to pregnancy by translating and cross-culturally adapting a specific assessment instrument to be used with Brazilian women. METHODS: this was a cross-sectional observational study. the translation and cross-cultural adaptation and of the Prenatal Self-evaluation Questionnaire (PSeQ) was performed following all the required methodological steps. another questionnaire was applied to characterize the sociodemographic and clinical status of the pregnant women (n=36). Statistical analysis consisted of the determination of the mean and standard deviation (SD) and of absolute and relative frequency. the statistical test used for the analysis of internal consistency was Cronbach's alpha coefficient, using SPSS version 17.0. RESULTS: the volunteers were of low socioeconomic status, aged on average 25.1 years ( 5.5), and had an average gestational age of 25.9 weeks ( 8.1). 58.3% of these volunteers had not planned their current pregnancy. the pretest showed that 75% of the pregnant women found the questionnaire easy to understand. Regarding the PSeQ instrument, the identification with the maternal role was the subcategory which showed the highest average, 24.8 ( 5.6), while the relationship with the mother had the lowest average 15.4 ( 7.7). the internal consistency ranged from 0.52 to 0.89. CONCLUSION: the assessment of psychosocial adaptation to pregnancy in pregnant women is very important during the progress of pregnancy and permits intervention through obstetric-neonatal actions of promotion and prevention regarding the well-being of mother and child.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):188-195
DOI 10.1590/S0100-72032011000800004
PURPOSE: To describe the epidemiological profile and nutritional status of pregnant women infected with human immunodeficiency virus (HIV) and its effect on the nutritional status of these women during pregnancy. METHODS: A retrospective cohort study was conducted on 121 pregnant women with HIV infection, single fetus pregnancies, who received prenatal care and delivered at a referral unit for HIV-infected pregnant women during the period from 1997 to 2007. Outcomes of the study were the initial and final nutritional status as measured by body mass index, weight gain, anemia (hemoglobin <11 g/dL) and low birth weight. Bivariate analysis investigated the association of these outcomes with socio-demographic, clinical-care and dietary characteristics. We estimated the relative risks (RR) with 95% confidence intervals (CI). RESULTS: At the beginning of pregnancy, 11.0% of the women were underweight, and in late pregnancy, the prevalence was 29.3%. Low educational level, urinary infection and worm infestation were associated with low gestational weight in late pregnancy. The percentage of insufficient weight gain was 47.5%, with well-nourished pregnant women (RR=3.3 95%CI 1.3-8.1) and women with no companion (RR=1.5 95%CI 1.1-2.2) having a higher risk for this outcome. The prevalences of overweight at the beginning and at the end of pregnancy were 26.8 and 29.4, respectively. There was a significant prevalence of anemia (61.0%). CONCLUSIONS: The high percentage of negative nutritional outcomes identified at this referral service with multidisciplinary care for pregnant women living with HIV reveals the need to establish more effective strategies to deal with the complex context of HIV.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):188-195
DOI 10.1590/S0100-72032011000800004
PURPOSE: To describe the epidemiological profile and nutritional status of pregnant women infected with human immunodeficiency virus (HIV) and its effect on the nutritional status of these women during pregnancy. METHODS: A retrospective cohort study was conducted on 121 pregnant women with HIV infection, single fetus pregnancies, who received prenatal care and delivered at a referral unit for HIV-infected pregnant women during the period from 1997 to 2007. Outcomes of the study were the initial and final nutritional status as measured by body mass index, weight gain, anemia (hemoglobin <11 g/dL) and low birth weight. Bivariate analysis investigated the association of these outcomes with socio-demographic, clinical-care and dietary characteristics. We estimated the relative risks (RR) with 95% confidence intervals (CI). RESULTS: At the beginning of pregnancy, 11.0% of the women were underweight, and in late pregnancy, the prevalence was 29.3%. Low educational level, urinary infection and worm infestation were associated with low gestational weight in late pregnancy. The percentage of insufficient weight gain was 47.5%, with well-nourished pregnant women (RR=3.3 95%CI 1.3-8.1) and women with no companion (RR=1.5 95%CI 1.1-2.2) having a higher risk for this outcome. The prevalences of overweight at the beginning and at the end of pregnancy were 26.8 and 29.4, respectively. There was a significant prevalence of anemia (61.0%). CONCLUSIONS: The high percentage of negative nutritional outcomes identified at this referral service with multidisciplinary care for pregnant women living with HIV reveals the need to establish more effective strategies to deal with the complex context of HIV.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):196-200
DOI 10.1590/S0100-72032011000800005
PURPOSE: To estimate the prevalence of asymptomatic bacteriuria among pregnant women attended at our university prenatal care clinic and to identify probable clinical predictors. METHODS: Across-sectional study was carried out from August 2008 to October 2009 at the Bahiana School of Medicine involving 260 pregnant women without symptoms of urinary tract infection. The following exclusion criteria were considered: presence of clinical signs such as fever, dysuria, vesical tenesmus, lumbar pain, history of active genital bleeding or loss of amniotic fluid, use of antimicrobial agents in the 30 days prior to sample collection, and refusal to participate in the project. The presence of single pathogen bacterial colonization ≥10(5) CFU/mL in the urine sample obtained from the middle jet was considered to be a dependent variable. The predictive factors evaluated were as follows: age, race, marital status, schooling, gestational age, hypertension, anemia, vaginal infection, sickle cell trait and previous history of urinary tract infection, urinary symptoms related to the lower urinary tract (frequency, urgency and nocturia) and data obtained from the urine summary (leukocyturia, increased bacterial flora, hematuria, proteinuria, and presence of nitrite). Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS) software version 13.0 and the level of significance was set at p<0.05. Prevalences were expressed as percentage, and the confidence interval considered was 95% (95%CI). RESULTS: The prevalence of asymptomatic bacteriuria was 12.3% (95%CI=8.3-16.3). E. coli was the most frequent etiologic agent (59.4%). Logistic regression indicated that urgency to void (OR=5.99; 95%CI=2.20-16.31; p<0.001); leukocyturia (OR=2.85; 95%CI=1.04-7.83; p=0.042) and increased bacterial flora (OR=10.62; 95%CI=3.95-28.56; p<0.001) were independent predictors of asymptomatic bacteriuria. CONCLUSION: The prevalence of asymptomatic bacteriuria in the studied population was high. The prediction score created for the final logistic regression model has an accuracy of 91.9% for bacteriuria.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):196-200
DOI 10.1590/S0100-72032011000800005
PURPOSE: To estimate the prevalence of asymptomatic bacteriuria among pregnant women attended at our university prenatal care clinic and to identify probable clinical predictors. METHODS: Across-sectional study was carried out from August 2008 to October 2009 at the Bahiana School of Medicine involving 260 pregnant women without symptoms of urinary tract infection. The following exclusion criteria were considered: presence of clinical signs such as fever, dysuria, vesical tenesmus, lumbar pain, history of active genital bleeding or loss of amniotic fluid, use of antimicrobial agents in the 30 days prior to sample collection, and refusal to participate in the project. The presence of single pathogen bacterial colonization ≥10(5) CFU/mL in the urine sample obtained from the middle jet was considered to be a dependent variable. The predictive factors evaluated were as follows: age, race, marital status, schooling, gestational age, hypertension, anemia, vaginal infection, sickle cell trait and previous history of urinary tract infection, urinary symptoms related to the lower urinary tract (frequency, urgency and nocturia) and data obtained from the urine summary (leukocyturia, increased bacterial flora, hematuria, proteinuria, and presence of nitrite). Statistical analysis was performed with the Statistical Package for the Social Sciences (SPSS) software version 13.0 and the level of significance was set at p<0.05. Prevalences were expressed as percentage, and the confidence interval considered was 95% (95%CI). RESULTS: The prevalence of asymptomatic bacteriuria was 12.3% (95%CI=8.3-16.3). E. coli was the most frequent etiologic agent (59.4%). Logistic regression indicated that urgency to void (OR=5.99; 95%CI=2.20-16.31; p<0.001); leukocyturia (OR=2.85; 95%CI=1.04-7.83; p=0.042) and increased bacterial flora (OR=10.62; 95%CI=3.95-28.56; p<0.001) were independent predictors of asymptomatic bacteriuria. CONCLUSION: The prevalence of asymptomatic bacteriuria in the studied population was high. The prediction score created for the final logistic regression model has an accuracy of 91.9% for bacteriuria.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):201-206
DOI 10.1590/S0100-72032011000800006
PURPOSE: To evaluate the impact of uterine artery embolization (UAE) on uterine volume (UV), greater myoma diameter (GMD) and ovarian function three months after the procedure, by transvaginal pelvic ultrasonography (TVPUS) and by the determination of follicle-stimulating hormone (FSH). METHODS: Thirty patients with leiomyomas were submitted to UAE. TVPUS and FSH determination were performed before and three months after UAE. UV was determined in cm³, GMD in cm and FSH in IU/mL. Data are reported as as mean standard deviation (SD) and were analyzed statistically by the nonparametric Mann-Whitney test. RESULTS: Twenty-nine patients were analyzed. Before UAE, mean UV was 402.4 165.9 cm³ and GMD was 5.9 2.1 cm. After UAE, mean UV was 258.9 118.6 cm³ and GMD was 4.6 1.8 cm. Mean FSH concentration was 4.9 3.5 IU/mL before UAE and 5.5 4.7 IU/mL after UAE, with p=0.5. There was a 35% reduction of UV and a 22% reduction of GMD, with no changes in FSH values after three months. CONCLUSION: The procedure significantly reduced UV and GMD but did not cause a significant increase in FSH levels, thus causing no changes in ovarian function.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):201-206
DOI 10.1590/S0100-72032011000800006
PURPOSE: To evaluate the impact of uterine artery embolization (UAE) on uterine volume (UV), greater myoma diameter (GMD) and ovarian function three months after the procedure, by transvaginal pelvic ultrasonography (TVPUS) and by the determination of follicle-stimulating hormone (FSH). METHODS: Thirty patients with leiomyomas were submitted to UAE. TVPUS and FSH determination were performed before and three months after UAE. UV was determined in cm³, GMD in cm and FSH in IU/mL. Data are reported as as mean standard deviation (SD) and were analyzed statistically by the nonparametric Mann-Whitney test. RESULTS: Twenty-nine patients were analyzed. Before UAE, mean UV was 402.4 165.9 cm³ and GMD was 5.9 2.1 cm. After UAE, mean UV was 258.9 118.6 cm³ and GMD was 4.6 1.8 cm. Mean FSH concentration was 4.9 3.5 IU/mL before UAE and 5.5 4.7 IU/mL after UAE, with p=0.5. There was a 35% reduction of UV and a 22% reduction of GMD, with no changes in FSH values after three months. CONCLUSION: The procedure significantly reduced UV and GMD but did not cause a significant increase in FSH levels, thus causing no changes in ovarian function.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):207-213
DOI 10.1590/S0100-72032011000800007
PURPOSE: To investigate changes in the dietary consumption as well as the influence of the general characteristics, of the sociodemographic, clinical and nutritional factors, and of the antineoplastic therapy on the changes in the energy intake of women from southern Brazil, before and after adjuvant therapy for breast cancer. METHODS: A non-randomized clinical study was conducted on 53 patients at a hospital of the public health network. Dietary information was collected with a food frequency questionnaire. A mixed-effects linear regression model was used to evaluate the factors that influenced longitudinal alterations of energy intake. RESULTS: A significant increase was observed in daily energy intake of fats, calcium, iron, copper, polyunsaturated fatty acids, omega 6 and omega 3, and a significant decrease in vitamin B2 intake. The final regression model for the change in energy intake showed an average increase of 19.2 kcal/month. Fruit and legume consumption showed the highest association with energy intake, with each 100 g consumed resulting in an average increase of 68.4 and 370.5 kcal, respectively. Women in the 51 to 60 year age range consumed 403.5 kcal less than those in the 31 to 50 year age range. CONCLUSION: There was an increase in energy intake during treatment and the increase in the ingestion of fruits and legumes was associated with significant increases in energy intake.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):207-213
DOI 10.1590/S0100-72032011000800007
PURPOSE: To investigate changes in the dietary consumption as well as the influence of the general characteristics, of the sociodemographic, clinical and nutritional factors, and of the antineoplastic therapy on the changes in the energy intake of women from southern Brazil, before and after adjuvant therapy for breast cancer. METHODS: A non-randomized clinical study was conducted on 53 patients at a hospital of the public health network. Dietary information was collected with a food frequency questionnaire. A mixed-effects linear regression model was used to evaluate the factors that influenced longitudinal alterations of energy intake. RESULTS: A significant increase was observed in daily energy intake of fats, calcium, iron, copper, polyunsaturated fatty acids, omega 6 and omega 3, and a significant decrease in vitamin B2 intake. The final regression model for the change in energy intake showed an average increase of 19.2 kcal/month. Fruit and legume consumption showed the highest association with energy intake, with each 100 g consumed resulting in an average increase of 68.4 and 370.5 kcal, respectively. Women in the 51 to 60 year age range consumed 403.5 kcal less than those in the 31 to 50 year age range. CONCLUSION: There was an increase in energy intake during treatment and the increase in the ingestion of fruits and legumes was associated with significant increases in energy intake.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):123-131
DOI 10.1590/S0100-72032011000700002
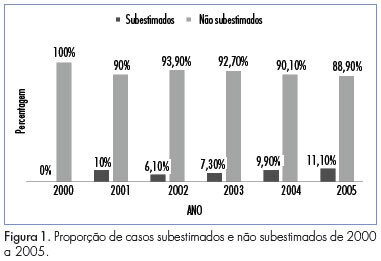
PURPOSE: To determine the rate of underestimation of an image-guided core biopsy of nonpalpable breast lesions, with validation by histologic examination after surgical excision. METHODS: We retrospectively reviewed 352 biopsies from patients who were submitted to surgery from February 2000 to December 2005, and whose histopathologic findings were recorded in the database system. Results were compared to surgical findings and underestimation rate was determined by dividing the number of lesions that proved to be carcinomas at surgical excision by the total number of lesions evaluated with excisional biopsy. Clinical, imaging, core biopsy and pathologic features were analyzed to identify factors that affect the rate of underestimation. The degree of agreement between the results was obtained by the percentage of agreement and Cohen's kappa coefficient. The association of variables with the underestimation of the diagnosis was determined by the chi-square, Fisher exact, ANOVA and Mann-Whitney U tests. The risk of underestimation was measured by the relative risk (RR) together with the respective 95% confidence intervals (95%CI). RESULTS: Inconclusive core biopsy findings occurred in 15.6% of cases. The histopathological result was benign in 26.4%, a high-risk lesion in 12.8% and malignant in 45.2%. There was agreement between core biopsy and surgery in 82.1% of cases (kappa=0.75). The false-negative rate was 5.4% and the lesion was completely removed in 3.4% of cases. The underestimation rate was 9.1% and was associated with BI-RADS® category 5 (p=0,01), microcalcifications (p CONCLUSIONS: The core breast biopsy under image guidance is a reliable procedure but the recommendation of surgical excision of high-risk lesions detected in the core biopsy remains since it was not possible to assess clinical, imaging, core biopsy and pathologic features that could predict underestimation and avoid excision. Representative samples are much more important than number of fragments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):123-131
DOI 10.1590/S0100-72032011000700002
PURPOSE: To determine the rate of underestimation of an image-guided core biopsy of nonpalpable breast lesions, with validation by histologic examination after surgical excision. METHODS: We retrospectively reviewed 352 biopsies from patients who were submitted to surgery from February 2000 to December 2005, and whose histopathologic findings were recorded in the database system. Results were compared to surgical findings and underestimation rate was determined by dividing the number of lesions that proved to be carcinomas at surgical excision by the total number of lesions evaluated with excisional biopsy. Clinical, imaging, core biopsy and pathologic features were analyzed to identify factors that affect the rate of underestimation. The degree of agreement between the results was obtained by the percentage of agreement and Cohen's kappa coefficient. The association of variables with the underestimation of the diagnosis was determined by the chi-square, Fisher exact, ANOVA and Mann-Whitney U tests. The risk of underestimation was measured by the relative risk (RR) together with the respective 95% confidence intervals (95%CI). RESULTS: Inconclusive core biopsy findings occurred in 15.6% of cases. The histopathological result was benign in 26.4%, a high-risk lesion in 12.8% and malignant in 45.2%. There was agreement between core biopsy and surgery in 82.1% of cases (kappa=0.75). The false-negative rate was 5.4% and the lesion was completely removed in 3.4% of cases. The underestimation rate was 9.1% and was associated with BI-RADS® category 5 (p=0,01), microcalcifications (p CONCLUSIONS: The core breast biopsy under image guidance is a reliable procedure but the recommendation of surgical excision of high-risk lesions detected in the core biopsy remains since it was not possible to assess clinical, imaging, core biopsy and pathologic features that could predict underestimation and avoid excision. Representative samples are much more important than number of fragments.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):132-136
DOI 10.1590/S0100-72032011000700003
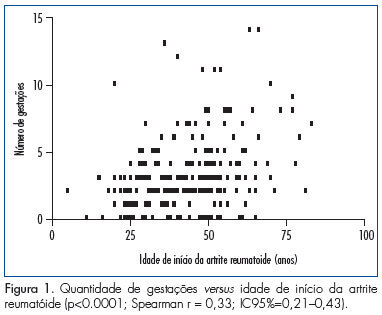
PURPOSE: To study if rheumatoid arthritis (RA) is influenced by age at menarche, number of pregnancies and reproductive life span. METHODS: This was a cross-sectional and retrospective study of medical records of 247 RA patients. We collected data on menarche, menopause, number of pregnancies, autoantibodies, serositis, rheumatoid nodules, and functional index of Steinbrocker. Association studies were done using the Student t and Mann-Whitney tests and correlation was determined by the Pearsonand Spearman tests. The level of significance adopted was 5%. RESULTS: The mean age at diagnosis of RA was 43.2±14.1 years, the median age at menarche was 13 years and the median number of pregnancies was 3. Rheumatoid factor was present in 63.9% of the patients, 20% had antinuclear factor, 8.8% rheumatoid nodules, 2.8% had pleural effusion, and 2.4% had pericarditis. The Steinbrocker functional index showed that 45.6% had a score of 1, 40.8% a score of 2, 3 score of 9.1, and 4.3% a score of 4. We found an inverse correlation between the number of pregnancies and age at onset of RA (p CONCLUSION: A precocious menarche and brief reproductive life indicate a poor prognosis regarding pleurisy. A larger number of pregnancies and late menopause show a protective effect, delaying the onset of the disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(7):132-136
DOI 10.1590/S0100-72032011000700003
PURPOSE: To study if rheumatoid arthritis (RA) is influenced by age at menarche, number of pregnancies and reproductive life span. METHODS: This was a cross-sectional and retrospective study of medical records of 247 RA patients. We collected data on menarche, menopause, number of pregnancies, autoantibodies, serositis, rheumatoid nodules, and functional index of Steinbrocker. Association studies were done using the Student t and Mann-Whitney tests and correlation was determined by the Pearsonand Spearman tests. The level of significance adopted was 5%. RESULTS: The mean age at diagnosis of RA was 43.2±14.1 years, the median age at menarche was 13 years and the median number of pregnancies was 3. Rheumatoid factor was present in 63.9% of the patients, 20% had antinuclear factor, 8.8% rheumatoid nodules, 2.8% had pleural effusion, and 2.4% had pericarditis. The Steinbrocker functional index showed that 45.6% had a score of 1, 40.8% a score of 2, 3 score of 9.1, and 4.3% a score of 4. We found an inverse correlation between the number of pregnancies and age at onset of RA (p CONCLUSION: A precocious menarche and brief reproductive life indicate a poor prognosis regarding pleurisy. A larger number of pregnancies and late menopause show a protective effect, delaying the onset of the disease.