Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):304-309
DOI 10.1590/S0100-72032012000700003
PURPOSE: To evaluate the impact of body mass index (BMI) at the beginning of pregnancy and weight gain on pregnancy outcome so that this measure can be implemented and valued by prenatal care health services. METHOD: Cross-sectional population-based study of all births in the only two hospitals in Rio Grande city (Brazil), in 2007. Among the 2,557 mothers interviewed, it was possible to calculate BMI in only 1,117. The Stata 11 software was used for data analysis. Logist regression was applied to the outomes involving diabetes mellitus, premature labor and cesarean section. Regarding birth weight, data were adjusted by multinomial logistic regression using as base category the group of 2,500 to 4,000 g. The level of significance was set at p-value <0.05 in a two-tailed test. RESULTS: There was no increased risk of hypertension or diabetes in patients in the different groups of BMI and weight gain. The risk of preterm delivery was evident in the group with a weight gain ≤8 kg (p<0.05). Regarding the route of delivery, it was observed that the higher the BMI in early pregnancy (p=0.001) and the greater the weight gain during pregnancy (p=0.004), the greater the risk of surgical delivery, which reached 11% in the group of obese mothers (p=0.004) and 12% in the group with a weight gain ≥17 kg (p=0.001). The weight of the newborns was influenced by BMI and weight gain, and the higher the BMI in early pregnancy and the gestational weight gain, the greater the risk of macrosomia. CONCLUSION: The monitoring of BMI and weight gain during pregnancy is a low cost and useful procedure for the establishment of nutritional interventions aimed at reducing maternal and fetal risks.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(7):304-309
DOI 10.1590/S0100-72032012000700003
PURPOSE: To evaluate the impact of body mass index (BMI) at the beginning of pregnancy and weight gain on pregnancy outcome so that this measure can be implemented and valued by prenatal care health services. METHOD: Cross-sectional population-based study of all births in the only two hospitals in Rio Grande city (Brazil), in 2007. Among the 2,557 mothers interviewed, it was possible to calculate BMI in only 1,117. The Stata 11 software was used for data analysis. Logist regression was applied to the outomes involving diabetes mellitus, premature labor and cesarean section. Regarding birth weight, data were adjusted by multinomial logistic regression using as base category the group of 2,500 to 4,000 g. The level of significance was set at p-value <0.05 in a two-tailed test. RESULTS: There was no increased risk of hypertension or diabetes in patients in the different groups of BMI and weight gain. The risk of preterm delivery was evident in the group with a weight gain ≤8 kg (p<0.05). Regarding the route of delivery, it was observed that the higher the BMI in early pregnancy (p=0.001) and the greater the weight gain during pregnancy (p=0.004), the greater the risk of surgical delivery, which reached 11% in the group of obese mothers (p=0.004) and 12% in the group with a weight gain ≥17 kg (p=0.001). The weight of the newborns was influenced by BMI and weight gain, and the higher the BMI in early pregnancy and the gestational weight gain, the greater the risk of macrosomia. CONCLUSION: The monitoring of BMI and weight gain during pregnancy is a low cost and useful procedure for the establishment of nutritional interventions aimed at reducing maternal and fetal risks.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):107-112
DOI 10.1590/S0100-72032012000300003
PURPOSE: To analyze the influence of maternal nutritional status, weight gain and energy consumption on fetal growth in high-risk pregnancies. METHODS: A prospective study from August 2009 to August 2010 with the following inclusion criteria: puerperae up to the 5th postpartum day; high-risk singleton pregnancies (characterized by medical or obstetrical complications during pregnancy); live fetus at labor onset; delivery at the institution; maternal weight measured on the day of delivery, and presence of medical and/or obstetrical complications characterizing pregnancy as high-risk. Nutritional status was assessed by pregestational body mass index and body mass index in late pregnancy, and the patients were classified as: underweight, adequate, overweight and obese. A food frequency questionnaire was applied to evaluate energy consumption. We investigated maternal weight gain, delivery data and perinatal outcomes, as well as fetal growth based on the occurrence of small for gestational age and large for gestational age neonates. RESULTS: We included 374 women who were divided into three study groups according to newborn birth weight: adequate for gestational age (270 cases, 72.2%), small for gestational age (91 cases, 24.3%), and large for gestational age (13 cases, 3.5%). Univaried analysis showed that women with small for gestational age neonates had a significantly lower mean pregestational body mass index (23.5 kg/m², p<0.001), mean index during late pregnancy (27.7 kg/m², p<0.001), and a higher proportion of maternal underweight at the end of pregnancy (25.3%, p<0.001). Women with large for gestational age neonates had a significantly higher mean pregestational body mass index (29.1 kg/m², p<0.001), mean index during late pregnancy (34.3 kg/m², p<0.001), and a higher proportion of overweight (30.8%, p=0.02) and obesity (38.5%, p=0.02) according to pregestational body mass index, and obesity at the end of pregnancy (53.8%, p<0.001). Multivariate analysis revealed the index value during late pregnancy (OR=0.9; CI95% 0.8-0.9, p<0.001) and the presence of hypertension (OR=2.6; 95%CI 1.5-4.5, p<0.001) as independent factors for small for gestational age. Independent predictors of large for gestational age infant were the presence of diabetes mellitus (OR=20.2; 95%CI 5.3-76.8, p<0.001) and obesity according to body mass index during late pregnancy (OR=3.6; 95%CI 1.1-11.7, p=0.04). CONCLUSION: The maternal nutritional status at the end of pregnancy in high-risk pregnancies is independently associated with fetal growth, the body mass index during late pregnancy is a protective factor against small for gestational age neonates, and maternal obesity is a risk factor for large for gestational age neonates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(3):107-112
DOI 10.1590/S0100-72032012000300003
PURPOSE: To analyze the influence of maternal nutritional status, weight gain and energy consumption on fetal growth in high-risk pregnancies. METHODS: A prospective study from August 2009 to August 2010 with the following inclusion criteria: puerperae up to the 5th postpartum day; high-risk singleton pregnancies (characterized by medical or obstetrical complications during pregnancy); live fetus at labor onset; delivery at the institution; maternal weight measured on the day of delivery, and presence of medical and/or obstetrical complications characterizing pregnancy as high-risk. Nutritional status was assessed by pregestational body mass index and body mass index in late pregnancy, and the patients were classified as: underweight, adequate, overweight and obese. A food frequency questionnaire was applied to evaluate energy consumption. We investigated maternal weight gain, delivery data and perinatal outcomes, as well as fetal growth based on the occurrence of small for gestational age and large for gestational age neonates. RESULTS: We included 374 women who were divided into three study groups according to newborn birth weight: adequate for gestational age (270 cases, 72.2%), small for gestational age (91 cases, 24.3%), and large for gestational age (13 cases, 3.5%). Univaried analysis showed that women with small for gestational age neonates had a significantly lower mean pregestational body mass index (23.5 kg/m², p<0.001), mean index during late pregnancy (27.7 kg/m², p<0.001), and a higher proportion of maternal underweight at the end of pregnancy (25.3%, p<0.001). Women with large for gestational age neonates had a significantly higher mean pregestational body mass index (29.1 kg/m², p<0.001), mean index during late pregnancy (34.3 kg/m², p<0.001), and a higher proportion of overweight (30.8%, p=0.02) and obesity (38.5%, p=0.02) according to pregestational body mass index, and obesity at the end of pregnancy (53.8%, p<0.001). Multivariate analysis revealed the index value during late pregnancy (OR=0.9; CI95% 0.8-0.9, p<0.001) and the presence of hypertension (OR=2.6; 95%CI 1.5-4.5, p<0.001) as independent factors for small for gestational age. Independent predictors of large for gestational age infant were the presence of diabetes mellitus (OR=20.2; 95%CI 5.3-76.8, p<0.001) and obesity according to body mass index during late pregnancy (OR=3.6; 95%CI 1.1-11.7, p=0.04). CONCLUSION: The maternal nutritional status at the end of pregnancy in high-risk pregnancies is independently associated with fetal growth, the body mass index during late pregnancy is a protective factor against small for gestational age neonates, and maternal obesity is a risk factor for large for gestational age neonates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(2):56-62
DOI 10.1590/S0100-72032012000200003
PURPOSE: To describe the characteristics of pregnancies complicated by maternal syphilis and fetal death. METHODS: Retrospective descriptive study performed by reviewing the medical records of 48 pregnant women with maternal syphilis and fetal death outcome admitted to Hospital Geral de Nova Iguaçu, Baixada Fluminense, State of Rio de Janeiro, during the period from 2005 to 2008. Birth weight >500 g and fetal death documented by Death Certificate were the inclusion criteria. The following aspects were analyzed: sociodemographic factors, reproductive history, aspects of the current pregnancy, prenatal care, Venereal Disease Research Laboratory (VDRL) testing, and other gestational conditions, in addition to syphilis. The fetal deaths were classified as maternal, placental or fetal. Percentage, mean, standard deviation (SD), maximum and minimum values were reported. RESULTS: The mean maternal age was 22.7 years (SD=0.9 years), and at least 50% of the patients had low educational level. At hospital admission, 68.8% of the subjects were in the third trimester, with a mean gestational age of 29.2 weeks (SD=0.5), and more than 50% were in labor. The vast majority of fetal deaths (93%) occurred before maternal hospitalization. Among the patients who received prenatal care (54.2%), 30.8% had no VDRL test, 30.8 and 15.4% had a reactive and non-reactive result, respectively, and none had more than one prenatal VDRL test. At the time of childbirth, most of the mothers (95.8%) carried out VDRL testing. Overall, the VDRL titers varied from 1:1 to 1:512, with predominant values >1:4 (91.7%). In 23% of cases other clinical conditions related to fetal death, in addition to syphilis, were found. CONCLUSIONS: The infection was the main clinically identified cause of fetal death in this patient series. Fetal death occurred during the preterm period and in the presence of high titers of maternal infection, suggesting recent syphilis infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(2):56-62
DOI 10.1590/S0100-72032012000200003
PURPOSE: To describe the characteristics of pregnancies complicated by maternal syphilis and fetal death. METHODS: Retrospective descriptive study performed by reviewing the medical records of 48 pregnant women with maternal syphilis and fetal death outcome admitted to Hospital Geral de Nova Iguaçu, Baixada Fluminense, State of Rio de Janeiro, during the period from 2005 to 2008. Birth weight >500 g and fetal death documented by Death Certificate were the inclusion criteria. The following aspects were analyzed: sociodemographic factors, reproductive history, aspects of the current pregnancy, prenatal care, Venereal Disease Research Laboratory (VDRL) testing, and other gestational conditions, in addition to syphilis. The fetal deaths were classified as maternal, placental or fetal. Percentage, mean, standard deviation (SD), maximum and minimum values were reported. RESULTS: The mean maternal age was 22.7 years (SD=0.9 years), and at least 50% of the patients had low educational level. At hospital admission, 68.8% of the subjects were in the third trimester, with a mean gestational age of 29.2 weeks (SD=0.5), and more than 50% were in labor. The vast majority of fetal deaths (93%) occurred before maternal hospitalization. Among the patients who received prenatal care (54.2%), 30.8% had no VDRL test, 30.8 and 15.4% had a reactive and non-reactive result, respectively, and none had more than one prenatal VDRL test. At the time of childbirth, most of the mothers (95.8%) carried out VDRL testing. Overall, the VDRL titers varied from 1:1 to 1:512, with predominant values >1:4 (91.7%). In 23% of cases other clinical conditions related to fetal death, in addition to syphilis, were found. CONCLUSIONS: The infection was the main clinically identified cause of fetal death in this patient series. Fetal death occurred during the preterm period and in the presence of high titers of maternal infection, suggesting recent syphilis infection.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(6):271-275
DOI 10.1590/S0100-72032011000600002
PURPOSE: to investigate the association between gene polymorphism of the progesterone receptor (PROGINS) and the risk of premature birth. METHODS: In this case-control study, 57 women with previous premature delivery (Case Group) and 57 patients with delivery at term in the current pregnancy and no history of preterm delivery (Control Group) were selected. A 10 mL amount of peripheral blood was collected by venipuncture and genomic DNA was extracted followed by the polymerase chain reaction (PCR) under specific conditions for this polymorphism and 2% agarose gel electrophoresis. The bands were visualized with an ultraviolet light transilluminator. Genotype and allele PROGINS frequencies were compared between the two groups by the χ2 test, with the level of significance set at value p<0.05. The Odds Ratio (OR) was also used, with 95% confidence intervals. RESULTS: PROGINS genotypic frequencies were 75.4% T1/T1, 22.8% T1/T2 and 1.8% T2/T2 in the Group with Preterm Delivery and 80.7% T1/T1, 19.3% T1/T2 and 0% T2/T2 in the term Delivery Group. There were no differences between groups when genotype and allele frequencies were analyzed: p=0.4 (OR=0.7) and p=0.4 (OR=0.7). CONCLUSIONS: the present study suggests that the presence of PROGINS polymorphism in our population does not constitute a risk factor for premature birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(6):271-275
DOI 10.1590/S0100-72032011000600002
PURPOSE: to investigate the association between gene polymorphism of the progesterone receptor (PROGINS) and the risk of premature birth. METHODS: In this case-control study, 57 women with previous premature delivery (Case Group) and 57 patients with delivery at term in the current pregnancy and no history of preterm delivery (Control Group) were selected. A 10 mL amount of peripheral blood was collected by venipuncture and genomic DNA was extracted followed by the polymerase chain reaction (PCR) under specific conditions for this polymorphism and 2% agarose gel electrophoresis. The bands were visualized with an ultraviolet light transilluminator. Genotype and allele PROGINS frequencies were compared between the two groups by the χ2 test, with the level of significance set at value p<0.05. The Odds Ratio (OR) was also used, with 95% confidence intervals. RESULTS: PROGINS genotypic frequencies were 75.4% T1/T1, 22.8% T1/T2 and 1.8% T2/T2 in the Group with Preterm Delivery and 80.7% T1/T1, 19.3% T1/T2 and 0% T2/T2 in the term Delivery Group. There were no differences between groups when genotype and allele frequencies were analyzed: p=0.4 (OR=0.7) and p=0.4 (OR=0.7). CONCLUSIONS: the present study suggests that the presence of PROGINS polymorphism in our population does not constitute a risk factor for premature birth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(12):584-590
DOI 10.1590/S0100-72032010001200004
PURPOSE: to evaluate the differences between the maternal and perinatal outcomes of pregnancies complicated by preeclampsia, according to the classification as the severe/mild form, and the early/late onset form. METHODS: a retrospective study with 211 pregnancies complicated by preeclampsia, assessed at a university reference center from 2000 to 2010. The diagnosis and disease severity were based on the values of blood pressure, proteinuria, and clinical and laboratory findings. The pregnant's age, skin color, parity, blood pressure, urine protein semiquantitative values, presence of bilateral notch in the uterine artery dopplervelocimetry and birth conditions were compared between patients with mild and severe disease, as well as between those of early/late onset. The disease was considered to be of early onset when diagnosed at less than 34 weeks of gestational age. RESULTS: most patients had the severe form of preeclampsia (82.8%), and the onset of the condition was early in 50.7%. Blood pressure values (133.6±14.8 versus 115.4 mmHg, p=0.0004 and 132.2±16.5 versus 125.7 mmHg, p=0.0004) and semiquantitative proteinuria (p=0.0003 and p=0.0005) were higher in the early and severe forms compared to mild and late forms. Infant birth weight (1,435.4±521.6 versus 2,710±605.0 g, 1,923.7±807.9 versus 2,415.0±925.0 g, p<0.0001 for both) and Apgar score (p=0.01 for both) were smaller for severe and early preeclampsia compared to mild and late preeclampsia. On the other hand, the presence of a bilateral notch in the uterine arteries was linked to the forms of early onset (69.2 versus 47.9%, p=0.02), whereas fetal growth restriction was more frequent in the severe forms of preeclampsia (30 versus 4.4%, p=0.008). CONCLUSION: the preeclampsia classification based on maternal clinical parameters better reflected the conditions of fetal nutrition, while the early onset of the condition was associated with placental vasculopathy detected by dopplervelocimetry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(12):584-590
DOI 10.1590/S0100-72032010001200004
PURPOSE: to evaluate the differences between the maternal and perinatal outcomes of pregnancies complicated by preeclampsia, according to the classification as the severe/mild form, and the early/late onset form. METHODS: a retrospective study with 211 pregnancies complicated by preeclampsia, assessed at a university reference center from 2000 to 2010. The diagnosis and disease severity were based on the values of blood pressure, proteinuria, and clinical and laboratory findings. The pregnant's age, skin color, parity, blood pressure, urine protein semiquantitative values, presence of bilateral notch in the uterine artery dopplervelocimetry and birth conditions were compared between patients with mild and severe disease, as well as between those of early/late onset. The disease was considered to be of early onset when diagnosed at less than 34 weeks of gestational age. RESULTS: most patients had the severe form of preeclampsia (82.8%), and the onset of the condition was early in 50.7%. Blood pressure values (133.6±14.8 versus 115.4 mmHg, p=0.0004 and 132.2±16.5 versus 125.7 mmHg, p=0.0004) and semiquantitative proteinuria (p=0.0003 and p=0.0005) were higher in the early and severe forms compared to mild and late forms. Infant birth weight (1,435.4±521.6 versus 2,710±605.0 g, 1,923.7±807.9 versus 2,415.0±925.0 g, p<0.0001 for both) and Apgar score (p=0.01 for both) were smaller for severe and early preeclampsia compared to mild and late preeclampsia. On the other hand, the presence of a bilateral notch in the uterine arteries was linked to the forms of early onset (69.2 versus 47.9%, p=0.02), whereas fetal growth restriction was more frequent in the severe forms of preeclampsia (30 versus 4.4%, p=0.008). CONCLUSION: the preeclampsia classification based on maternal clinical parameters better reflected the conditions of fetal nutrition, while the early onset of the condition was associated with placental vasculopathy detected by dopplervelocimetry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):504-509
DOI 10.1590/S0100-72032010001000006
PURPOSE: to investigate the application of a multidisciplinary educational program to high-risk pregnancies due to endocrine diseases. METHODS: we retrospectively evaluated the application of a multidisciplinary educational program to 185 pregnant women with endocrine diseases referred to a maternity specialized in high-risk pregnancy. All pregnant women received multidisciplinary prenatal care from a team consisting of endocrinologists, obstetricians, sonographers, nurses and dietitians. Oral and written information about healthy habits, diabetes care, use of artificial sweeteners and exercise during pregnancy was given to all patients at the first endocrine consultation. An individualized nutrition plan was prepared on the occasion of the first visit to the nutritionist. In bi-weekly and monthly endocrine and nutritional visits, respectively, information about healthy changes in lifestyle was emphasized and the weight was recorded. Adherence to physical activity and nutritional counseling was self-reported. We compared the weekly weight before and after the intervention, fetal weight at birth, rate of macrosomia and low birth weight, and frequency of cesarean delivery among the four categories of body mass index (BMI) before pregnancy (<18.5, from 18.5 to 24.9, from 25 to 29.9 and >30 kg/m²). RESULTS: the main disease of referral was diabetes (84.9%). One third of the pregnant women (31.2%) were overweight and 42.5% were obese before pregnancy. Most women was first seen by the multidisciplinary team in the third trimester of pregnancy (64.1%) and 50.5% exceeded the recommended weight gain at first evaluation. Obese women exceeded the recommended weight gain in 62.5% of cases. After the intervention, the percentage of women who exceeded the recommended weekly weight gain was reduced in all categories of pre-pregnancy BMI, although a statistically significant difference was found only in the group with normal pre-pregnancy BMI (40.6 versus 21.9%, p = 0.03). At birth, average fetal weight was similar among the various BMI categories (p=0.277). Macrosomia was more frequent in women who were overweight and obese before pregnancy. Cesarean delivery was the most frequent route of delivery, regardless of pre-pregnancy BMI. CONCLUSIONS: in high-risk pregnancies due to endocrine disorders, a multidisciplinary educational approach limits excessive weekly weight gain despite the advanced gestational age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(10):504-509
DOI 10.1590/S0100-72032010001000006
PURPOSE: to investigate the application of a multidisciplinary educational program to high-risk pregnancies due to endocrine diseases. METHODS: we retrospectively evaluated the application of a multidisciplinary educational program to 185 pregnant women with endocrine diseases referred to a maternity specialized in high-risk pregnancy. All pregnant women received multidisciplinary prenatal care from a team consisting of endocrinologists, obstetricians, sonographers, nurses and dietitians. Oral and written information about healthy habits, diabetes care, use of artificial sweeteners and exercise during pregnancy was given to all patients at the first endocrine consultation. An individualized nutrition plan was prepared on the occasion of the first visit to the nutritionist. In bi-weekly and monthly endocrine and nutritional visits, respectively, information about healthy changes in lifestyle was emphasized and the weight was recorded. Adherence to physical activity and nutritional counseling was self-reported. We compared the weekly weight before and after the intervention, fetal weight at birth, rate of macrosomia and low birth weight, and frequency of cesarean delivery among the four categories of body mass index (BMI) before pregnancy (<18.5, from 18.5 to 24.9, from 25 to 29.9 and >30 kg/m²). RESULTS: the main disease of referral was diabetes (84.9%). One third of the pregnant women (31.2%) were overweight and 42.5% were obese before pregnancy. Most women was first seen by the multidisciplinary team in the third trimester of pregnancy (64.1%) and 50.5% exceeded the recommended weight gain at first evaluation. Obese women exceeded the recommended weight gain in 62.5% of cases. After the intervention, the percentage of women who exceeded the recommended weekly weight gain was reduced in all categories of pre-pregnancy BMI, although a statistically significant difference was found only in the group with normal pre-pregnancy BMI (40.6 versus 21.9%, p = 0.03). At birth, average fetal weight was similar among the various BMI categories (p=0.277). Macrosomia was more frequent in women who were overweight and obese before pregnancy. Cesarean delivery was the most frequent route of delivery, regardless of pre-pregnancy BMI. CONCLUSIONS: in high-risk pregnancies due to endocrine disorders, a multidisciplinary educational approach limits excessive weekly weight gain despite the advanced gestational age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(6):281-286
DOI 10.1590/S0100-72032008000600003
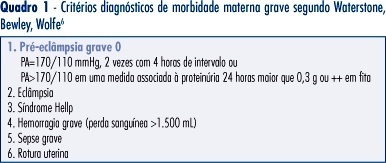
PURPOSE: to assess the prevalence and risk factors associated with near miss and other severe maternal morbidity at a reference tertiary maternity. METHODS: this is a cross-sectional study on severe maternal morbidity at the Hospital e Maternidade Celso Pierro, Campinas, São Paulo, between October 2005 and July 2006, identified from infirmary, admission and delivery unit logbooks. Pregnant and post-partum women with severe maternal morbidity were identified according to clinical criteria proposed by Waterstone. Later, cases with more severe morbidity, called extremely severe maternal morbidity, were reclassified using Mantel criteria, based on organic dysfunction and clinical management. RESULTS: there were 114 severe maternal morbidity cases among 2,207 birth deliveries, with a ratio of other severe morbidity and extremely severe morbidity near miss of 44.9 and 6.8 cases/1,000 live births, respectively. Mean gestational age at delivery was 35 weeks, and 87% came from the reference area for the maternity service. Hypertension (severe pre-eclampsia) represented 96% of other severe morbidity, while hemorrhage represented 60% of all extremely severe cases, followed by hypertension. The prevalence of extremely severe morbidity among the severe morbidity cases was not associated with marital status, schooling, maternal age, type of delivery, parity, gestational age at birth and home place. CONCLUSIONS: the other morbidities were 6.6 times more frequent than near miss, and it was not possible to differentiate both groups by epidemiological risk factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2008;30(6):281-286
DOI 10.1590/S0100-72032008000600003
PURPOSE: to assess the prevalence and risk factors associated with near miss and other severe maternal morbidity at a reference tertiary maternity. METHODS: this is a cross-sectional study on severe maternal morbidity at the Hospital e Maternidade Celso Pierro, Campinas, São Paulo, between October 2005 and July 2006, identified from infirmary, admission and delivery unit logbooks. Pregnant and post-partum women with severe maternal morbidity were identified according to clinical criteria proposed by Waterstone. Later, cases with more severe morbidity, called extremely severe maternal morbidity, were reclassified using Mantel criteria, based on organic dysfunction and clinical management. RESULTS: there were 114 severe maternal morbidity cases among 2,207 birth deliveries, with a ratio of other severe morbidity and extremely severe morbidity near miss of 44.9 and 6.8 cases/1,000 live births, respectively. Mean gestational age at delivery was 35 weeks, and 87% came from the reference area for the maternity service. Hypertension (severe pre-eclampsia) represented 96% of other severe morbidity, while hemorrhage represented 60% of all extremely severe cases, followed by hypertension. The prevalence of extremely severe morbidity among the severe morbidity cases was not associated with marital status, schooling, maternal age, type of delivery, parity, gestational age at birth and home place. CONCLUSIONS: the other morbidities were 6.6 times more frequent than near miss, and it was not possible to differentiate both groups by epidemiological risk factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(11):561-567
DOI 10.1590/S0100-72032007001100003
PURPOSE: to verify the association of abortion, recurrent fetal loss, miscarriage and severe pre-eclampsia with the presence of hereditary thrombophilias and antiphospholipid antibodies in pregnant women. METHODS: observational and transverse study of 48 pregnant women with past medical record of miscarriage, repeated abortion and fetal loss story (AB Group) and severe pre-eclampsia (PE Group), attended to in the High Risk Pregnancy Ambulatory of the Faculdade de Medicina (Famed) from the Universidade Federal de Mato Grosso do Sul (UFMS) from November 2006 to July 2007. The pregnant women of both groups were screened for the presence of antiphospholipid antibodies (anticardiolipin IgG and IgM, lupic anticoagulant and anti-beta2-glycoprotein I) and hereditary thrombophilias (protein C and S deficiency, antithrombin deficiency, hyperhomocysteinemia and factor V Leiden mutation). The laboratorial screening was performed during the pregnancy. The parametric data (maternal age and parity) were analyzed with Student’s tau test. The non-parametric data (presence/absence of hereditary thrombophilias and antiphospholipid antibodies, presence/absence of pre-eclampsia, fetal loss, miscarriage and repeated abortion) were analyzed with Fisher’s exact test in contingency tables. It was considered significant the association with p value <0.05. RESULTS: out of the 48 pregnant women, 31 (65%) were included in AB Group and 17 (35%) in PE Group. There was no significant difference between maternal age and parity within the groups. There was significant statistical association between recurrent fetal loss, recurrent abortions and previous miscarriages and maternal hereditary thrombophilias (p<0.05). There was no statistical association between the AB Group and the presence of antiphospholipid antibodies. Neither there were associations of the PE Group with maternal hereditary thrombophilias and the presence of antiphospholipid antibodies. CONCLUSIONS: the data obtained suggest routine laboratorial investigation for hereditary thrombophilias in pregnant women with previous obstetrical story of recurrent fetal loss, repeated abortion and miscarriage.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2007;29(11):561-567
DOI 10.1590/S0100-72032007001100003
PURPOSE: to verify the association of abortion, recurrent fetal loss, miscarriage and severe pre-eclampsia with the presence of hereditary thrombophilias and antiphospholipid antibodies in pregnant women. METHODS: observational and transverse study of 48 pregnant women with past medical record of miscarriage, repeated abortion and fetal loss story (AB Group) and severe pre-eclampsia (PE Group), attended to in the High Risk Pregnancy Ambulatory of the Faculdade de Medicina (Famed) from the Universidade Federal de Mato Grosso do Sul (UFMS) from November 2006 to July 2007. The pregnant women of both groups were screened for the presence of antiphospholipid antibodies (anticardiolipin IgG and IgM, lupic anticoagulant and anti-beta2-glycoprotein I) and hereditary thrombophilias (protein C and S deficiency, antithrombin deficiency, hyperhomocysteinemia and factor V Leiden mutation). The laboratorial screening was performed during the pregnancy. The parametric data (maternal age and parity) were analyzed with Student’s tau test. The non-parametric data (presence/absence of hereditary thrombophilias and antiphospholipid antibodies, presence/absence of pre-eclampsia, fetal loss, miscarriage and repeated abortion) were analyzed with Fisher’s exact test in contingency tables. It was considered significant the association with p value <0.05. RESULTS: out of the 48 pregnant women, 31 (65%) were included in AB Group and 17 (35%) in PE Group. There was no significant difference between maternal age and parity within the groups. There was significant statistical association between recurrent fetal loss, recurrent abortions and previous miscarriages and maternal hereditary thrombophilias (p<0.05). There was no statistical association between the AB Group and the presence of antiphospholipid antibodies. Neither there were associations of the PE Group with maternal hereditary thrombophilias and the presence of antiphospholipid antibodies. CONCLUSIONS: the data obtained suggest routine laboratorial investigation for hereditary thrombophilias in pregnant women with previous obstetrical story of recurrent fetal loss, repeated abortion and miscarriage.