Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(9):503-510
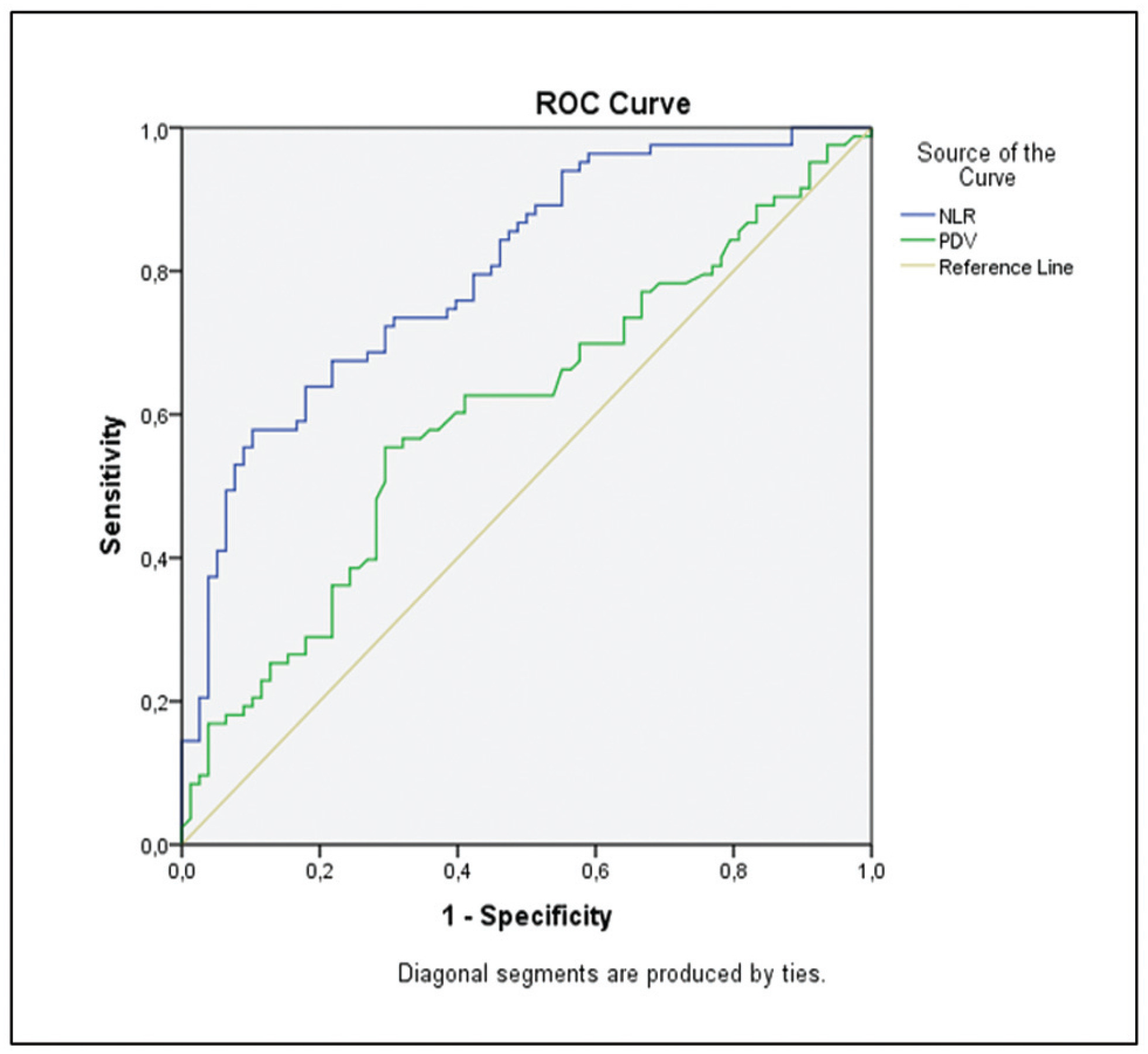
The availability of reliable and inexpensive markers that can be used to determine the risk of rupture during methotrexate (MTX) treatment in ectopic pregnancies (EPs) is considerable. The aim of the present study is to investigate the role of systemic inflammatory markers such as leukocytes (or white blood cells, WBCs), the neutrophil-to-lymphocyte ratio (NLR), and platelet distribution width (PDW), which are among the parameters of the complete blood count (CBC), in the prediction of rupture of EPs under MTX treatment.
A total of 161 patients with tubal EP who underwent a single-dose methotrexate (MTX) protocol were retrospectively analyzed, and the control group (n = 83) included patients cured by MTX, while the ruptured group (n = 78) included patients who were operated on for tubal rupture during the MTX treatment. The features of EP, beta-human chorionic gonadotropin (β-hCG) levels, sonographic findings, and CBC-derived markers such as WBC, NLR, and PDW, were investigated by comparing both groups.
The NLR was found to be higher in the ruptured group, of 2.92 ± 0.86%, and significantly lower in the control group, of 2.09 ± 0.6%. Similarly, the PDW was higher (51 ± 9%) in the ruptured group, and it was significantly lower a (47 ± 13%) in the control group (p < 0.05). Other CBC parameters were similar in both groups (p > 0.05).
Systemic inflammation markers derived from CBC can be easily applied to predict the risk of tubal rupture in Eps, since the CBC is an inexpensive and easy-to-apply test, which is first requested from each patient during hospitalization.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(9):503-510
The availability of reliable and inexpensive markers that can be used to determine the risk of rupture during methotrexate (MTX) treatment in ectopic pregnancies (EPs) is considerable. The aim of the present study is to investigate the role of systemic inflammatory markers such as leukocytes (or white blood cells, WBCs), the neutrophil-to-lymphocyte ratio (NLR), and platelet distribution width (PDW), which are among the parameters of the complete blood count (CBC), in the prediction of rupture of EPs under MTX treatment.
A total of 161 patients with tubal EP who underwent a single-dose methotrexate (MTX) protocol were retrospectively analyzed, and the control group (n = 83) included patients cured by MTX, while the ruptured group (n = 78) included patients who were operated on for tubal rupture during the MTX treatment. The features of EP, beta-human chorionic gonadotropin (β-hCG) levels, sonographic findings, and CBC-derived markers such as WBC, NLR, and PDW, were investigated by comparing both groups.
The NLR was found to be higher in the ruptured group, of 2.92 ± 0.86%, and significantly lower in the control group, of 2.09 ± 0.6%. Similarly, the PDW was higher (51 ± 9%) in the ruptured group, and it was significantly lower a (47 ± 13%) in the control group (p < 0.05). Other CBC parameters were similar in both groups (p > 0.05).
Systemic inflammation markers derived from CBC can be easily applied to predict the risk of tubal rupture in Eps, since the CBC is an inexpensive and easy-to-apply test, which is first requested from each patient during hospitalization.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1014-1020
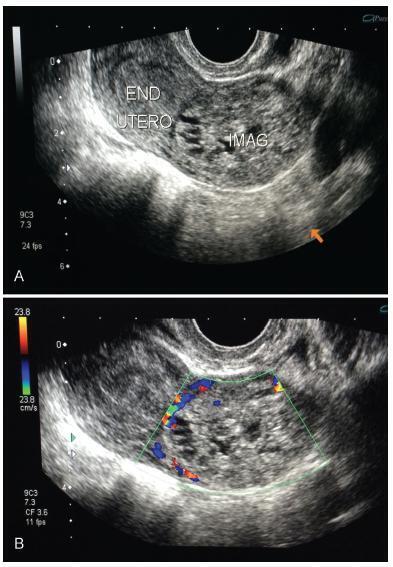
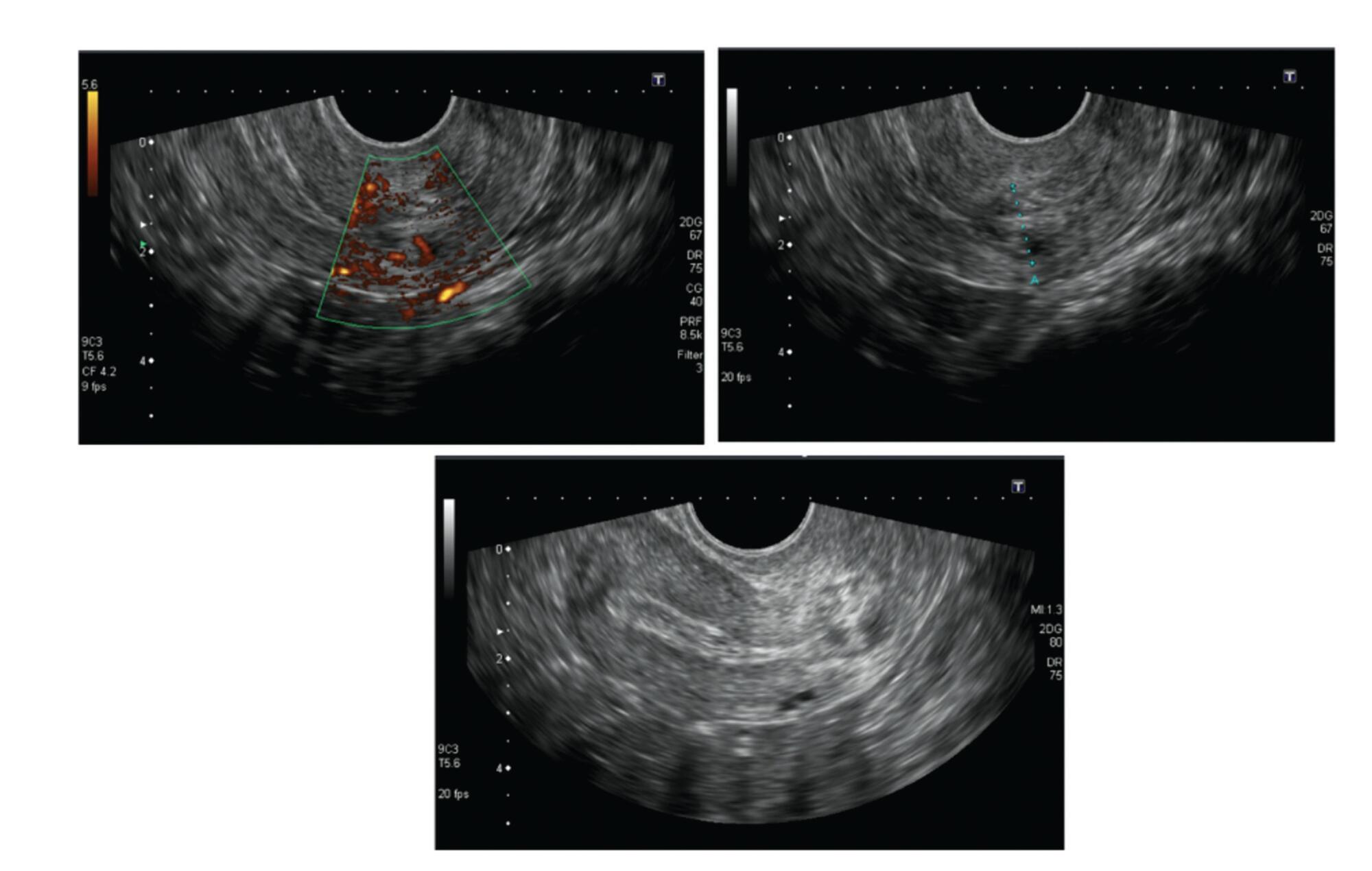
Cervical pregnancy is challenging for the medical community, as it is potentially fatal. The treatment can be medical or surgical; however, there are no protocols that establish the best option for each case. The objective of the present study was to describe the cases of cervical pregnancy admitted to a tertiary university hospital over a period of 18 years.
A retrospective study based on a review of the medical records of all cervical pregnancies admitted to the Women's Hospital at Universidade Estadual de Campinas, Southeastern Brazil, from 2000 to 2018.
We identified 13 cases of cervical pregnancy out of a total of 673 ectopic pregnancies; only 1 case was initially treated with surgery because of hemodynamic instability. Of the 12 cases treated conservatively, 7 were treated with single-dose intramuscular methotrexate, 1, with intravenous and intramuscular methotrexate, 1, with intravenous methotrexate, 1, with 2 doses of intramuscular methotrexate, and 2, with intra-amniotic methotrexate. Of these cases, one had a therapeutic failure that required a hysterectomy. Two women received blood transfusions. Four women required cervical tamponade with a Foley catheter balloon for hemostasis. There was no fatal outcome.
Cervical pregnancy is a rare and challenging condition from diagnosis to treatment. Conservative treatment was the primary method of therapy used, with satisfactory results. In cases of increased bleeding, cervical curettage was the initial treatment, and it was associated with the use of a cervical balloon for hemostasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(11):1014-1020
Cervical pregnancy is challenging for the medical community, as it is potentially fatal. The treatment can be medical or surgical; however, there are no protocols that establish the best option for each case. The objective of the present study was to describe the cases of cervical pregnancy admitted to a tertiary university hospital over a period of 18 years.
A retrospective study based on a review of the medical records of all cervical pregnancies admitted to the Women's Hospital at Universidade Estadual de Campinas, Southeastern Brazil, from 2000 to 2018.
We identified 13 cases of cervical pregnancy out of a total of 673 ectopic pregnancies; only 1 case was initially treated with surgery because of hemodynamic instability. Of the 12 cases treated conservatively, 7 were treated with single-dose intramuscular methotrexate, 1, with intravenous and intramuscular methotrexate, 1, with intravenous methotrexate, 1, with 2 doses of intramuscular methotrexate, and 2, with intra-amniotic methotrexate. Of these cases, one had a therapeutic failure that required a hysterectomy. Two women received blood transfusions. Four women required cervical tamponade with a Foley catheter balloon for hemostasis. There was no fatal outcome.
Cervical pregnancy is a rare and challenging condition from diagnosis to treatment. Conservative treatment was the primary method of therapy used, with satisfactory results. In cases of increased bleeding, cervical curettage was the initial treatment, and it was associated with the use of a cervical balloon for hemostasis.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(12):800-804
In recent years, there has been an increase in the incidence of ectopic pregnancies; therefore, it is important for tertiary centers to report their approaches and outcomes to expand and improve treatment modalities. The aim of the present study was to evaluate the general characteristics, treatment and outcomes of cases diagnosed with ectopic pregnancy.
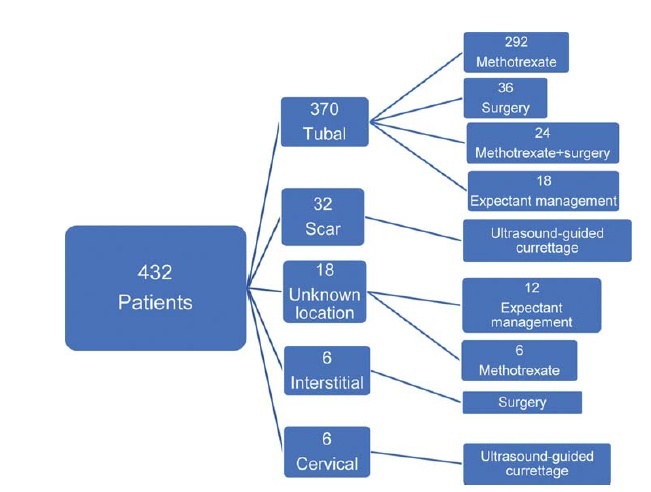
In total, 432 patients treated for ectopic pregnancy between February 2016 and June 2019 were retrospectively evaluated.
Overall, 370 patients had tubal pregnancy, 32 had cesarean scar pregnancy, 18 had pregnancy of unknown location, 6 had cervical pregnancy, and 6 had interstitial pregnancy. The most important risk factors were advanced age (> 35 years; prevalence: 31.2%) and smoking (prevalence: 27.1%). Thirty patients who did not have any symptoms of rupture and whose human chorionic gonadotropin (β-hCG) levels were ≤ 200 mIU/ml were followed-up with expectant management, while 316 patients whose β-hCG levels were between 1,500 mIU/ml and 5,000 mIU/ml did not have an intrauterine gestational sac on the transvaginal or abdominal ultrasound, did not demonstrate findings of rupture, and were treated with a systemic multi-dose methotrexate treatment protocol. In total, 24 patients who did not respond to the medical treatment, 20 patients whose β-hCG levels were > 5,000 mIU/ml, 16 patients who had shown symptoms of rupture at the initial presentation, and 6 patients diagnosed with interstitial pregnancy underwent surgery. Patients with cervical and scar pregnancies underwent ultrasound-guided curettage, and no additional treatment was needed.
The fertility status of the patients, the clinical and laboratory findings, and the levels of β-hCG are the factors that must be considered in planning the appropriate treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(12):800-804
In recent years, there has been an increase in the incidence of ectopic pregnancies; therefore, it is important for tertiary centers to report their approaches and outcomes to expand and improve treatment modalities. The aim of the present study was to evaluate the general characteristics, treatment and outcomes of cases diagnosed with ectopic pregnancy.
In total, 432 patients treated for ectopic pregnancy between February 2016 and June 2019 were retrospectively evaluated.
Overall, 370 patients had tubal pregnancy, 32 had cesarean scar pregnancy, 18 had pregnancy of unknown location, 6 had cervical pregnancy, and 6 had interstitial pregnancy. The most important risk factors were advanced age (> 35 years; prevalence: 31.2%) and smoking (prevalence: 27.1%). Thirty patients who did not have any symptoms of rupture and whose human chorionic gonadotropin (β-hCG) levels were ≤ 200 mIU/ml were followed-up with expectant management, while 316 patients whose β-hCG levels were between 1,500 mIU/ml and 5,000 mIU/ml did not have an intrauterine gestational sac on the transvaginal or abdominal ultrasound, did not demonstrate findings of rupture, and were treated with a systemic multi-dose methotrexate treatment protocol. In total, 24 patients who did not respond to the medical treatment, 20 patients whose β-hCG levels were > 5,000 mIU/ml, 16 patients who had shown symptoms of rupture at the initial presentation, and 6 patients diagnosed with interstitial pregnancy underwent surgery. Patients with cervical and scar pregnancies underwent ultrasound-guided curettage, and no additional treatment was needed.
The fertility status of the patients, the clinical and laboratory findings, and the levels of β-hCG are the factors that must be considered in planning the appropriate treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):59-61
Lithopedion (lithos = rock and paidion = child) is a rare condition that only occurs in 1.5 to 1.8% of extrauterine pregnancies and in 0.00045% of all pregnancies. It consists of an ectopic pregnancy in which the fetus dies but cannot be reabsorbed by the mother’s body, which then coats it in a calcium-rich substance.We present the case of a 77-year-old woman with an incidental diagnosis of a lithopedion, which had been retained in her left pelvis for presumably 40 years.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(1):59-61
Lithopedion (lithos = rock and paidion = child) is a rare condition that only occurs in 1.5 to 1.8% of extrauterine pregnancies and in 0.00045% of all pregnancies. It consists of an ectopic pregnancy in which the fetus dies but cannot be reabsorbed by the mother’s body, which then coats it in a calcium-rich substance.We present the case of a 77-year-old woman with an incidental diagnosis of a lithopedion, which had been retained in her left pelvis for presumably 40 years.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):129-132
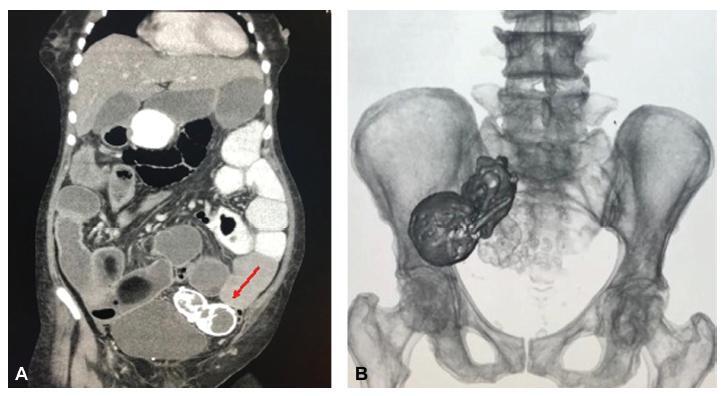
Ectopic pregnancy is the leading cause of pregnancy-related death during the first trimester, and it occurs in 1 to 2% of pregnancies. Over 90% of ectopic pregnancies are located in the fallopian tube. Abdominal pregnancy refers to an ectopic pregnancy that has implanted in the peritoneal cavity, external to the uterine cavity and fallopian tubes. The estimated incidence is 1 per 10,000 births and 1.4%of ectopic pregnancies. Lithopedion is a rare type of ectopic pregnancy, and it occurs when the fetus from an unrecognized abdominal pregnancymay die and calcify. The resulting “stone baby” may not be detected for decades andmay cause a variety of complications. Lithopedion is a very rare event that occurs in 0.0054% of all gestations. About 1.5 to 1.8% of the abdominal babies develop into lithopedion. There are only ~ 330 known cases of lithopedion in the world. We describe a lithopedion that complicated as intestinal obstruction in a 71-year-old woman.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(2):129-132
Ectopic pregnancy is the leading cause of pregnancy-related death during the first trimester, and it occurs in 1 to 2% of pregnancies. Over 90% of ectopic pregnancies are located in the fallopian tube. Abdominal pregnancy refers to an ectopic pregnancy that has implanted in the peritoneal cavity, external to the uterine cavity and fallopian tubes. The estimated incidence is 1 per 10,000 births and 1.4%of ectopic pregnancies. Lithopedion is a rare type of ectopic pregnancy, and it occurs when the fetus from an unrecognized abdominal pregnancymay die and calcify. The resulting “stone baby” may not be detected for decades andmay cause a variety of complications. Lithopedion is a very rare event that occurs in 0.0054% of all gestations. About 1.5 to 1.8% of the abdominal babies develop into lithopedion. There are only ~ 330 known cases of lithopedion in the world. We describe a lithopedion that complicated as intestinal obstruction in a 71-year-old woman.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(3):142-146
Frozen section examination is a rapid method for identifying products of conception in endometrial curetting, yet its accuracy is inconclusive. The purposes of this study is to determine the accuracy of frozen section analysis of endometrial curetting in pregnancies of unknown location, and to verify the relation of β-human chorionic gonadotrophin (hCG) level and endometrial thickness to the assessed accuracy.
We reviewed data from January 2009 to December 2014 of diagnostic curettages from women with suspected ectopic pregnancies sent for frozen section examination at a medical center. A frozen section diagnosis was considered accurate if it concurred with the final pathologic diagnosis.
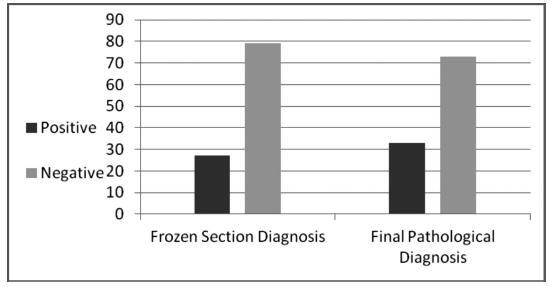
Of 106 frozen section studies, the diagnosis was accurate in 94 (88.7%). Of 79 specimens interpreted as negative on frozen sections (no products of conception noted), 9 (11.4%) were positive on final pathologic review. Three of the 27 (11.1%) specimens interpreted as positive by a frozen section failed to demonstrate products of conception on a final pathologic section. The sensitivity of frozen sections in the diagnosis of ectopic pregnancy was 72.7%, specificity 95.9%, positive predictive value 88.9%, negative predictive value 88.6%, and accuracy 88.6%. A statically significant correlation was found between β-hCG level and high accuracy of the frozen section technique (p< 0.001). No correlation was found between endometrial thickness and the accuracy of the frozen section technique.
The accuracy of frozen section examination was high and was found to correlate with β-hCG level, but not with endometrial thickness.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(3):142-146
Frozen section examination is a rapid method for identifying products of conception in endometrial curetting, yet its accuracy is inconclusive. The purposes of this study is to determine the accuracy of frozen section analysis of endometrial curetting in pregnancies of unknown location, and to verify the relation of β-human chorionic gonadotrophin (hCG) level and endometrial thickness to the assessed accuracy.
We reviewed data from January 2009 to December 2014 of diagnostic curettages from women with suspected ectopic pregnancies sent for frozen section examination at a medical center. A frozen section diagnosis was considered accurate if it concurred with the final pathologic diagnosis.
Of 106 frozen section studies, the diagnosis was accurate in 94 (88.7%). Of 79 specimens interpreted as negative on frozen sections (no products of conception noted), 9 (11.4%) were positive on final pathologic review. Three of the 27 (11.1%) specimens interpreted as positive by a frozen section failed to demonstrate products of conception on a final pathologic section. The sensitivity of frozen sections in the diagnosis of ectopic pregnancy was 72.7%, specificity 95.9%, positive predictive value 88.9%, negative predictive value 88.6%, and accuracy 88.6%. A statically significant correlation was found between β-hCG level and high accuracy of the frozen section technique (p< 0.001). No correlation was found between endometrial thickness and the accuracy of the frozen section technique.
The accuracy of frozen section examination was high and was found to correlate with β-hCG level, but not with endometrial thickness.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):680-685
Our aim is to demonstrate the importance of methotrexate (MTX) therapy for the treatment of ectopic pregnancy (EP).
This retrospective study consisted of 99 patients (72 tubal EPs, 20 pregnancies of unknown location (PUL), 4 cesarean section (CS) scar EPs and 3 cervical EPs) treated with MTX.
Methotrexate therapy was successful in 68.5% of EPs. There were statistically significant differences between the MTX success and failure groups based on ultrasonographic findings, patient complaints, gestational week and serum human chorionic gonadotropin (hCG) values. The MTX success rates in PUL and tubal pregnancies were 95% and 61.1%, respectively. The MTX success rates in single-dose, two-dose and multi-dose protocol groups were 86.9%, 28.6% and 40%, respectively. All cervical and CS scar ectopic pregnancies were treated successfully with MTX therapy.
Methotrexate might be the first-line treatment option for EPs under certain conditions. Physicians must be more cautious in cases with higher hCG values, the presence of abdominal-pelvic pain, the presence of fetal cardiac activity, larger gestational sac (GS) diameters, and more advanced gestational weeks according to the last menstrual period.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):680-685
Our aim is to demonstrate the importance of methotrexate (MTX) therapy for the treatment of ectopic pregnancy (EP).
This retrospective study consisted of 99 patients (72 tubal EPs, 20 pregnancies of unknown location (PUL), 4 cesarean section (CS) scar EPs and 3 cervical EPs) treated with MTX.
Methotrexate therapy was successful in 68.5% of EPs. There were statistically significant differences between the MTX success and failure groups based on ultrasonographic findings, patient complaints, gestational week and serum human chorionic gonadotropin (hCG) values. The MTX success rates in PUL and tubal pregnancies were 95% and 61.1%, respectively. The MTX success rates in single-dose, two-dose and multi-dose protocol groups were 86.9%, 28.6% and 40%, respectively. All cervical and CS scar ectopic pregnancies were treated successfully with MTX therapy.
Methotrexate might be the first-line treatment option for EPs under certain conditions. Physicians must be more cautious in cases with higher hCG values, the presence of abdominal-pelvic pain, the presence of fetal cardiac activity, larger gestational sac (GS) diameters, and more advanced gestational weeks according to the last menstrual period.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(5):294-299
This report presents the case of a patient with gestational trophoblastic neoplasia after a partial hydatidiform mole formed in the Fallopian tube. Ectopic molar pregnancy is a rare condition, with an estimated incidence of 1 in every 20,000 to 100,000 pregnancies; less than 300 cases of it have been reported in the Western literature. The present report is important because it presents current diagnostic criteria for this rare condition, which has been incorrectly diagnosed in the past, not only morphologically but also immunohistochemically. It also draws the attention of obstetricians to the occurrence of ectopic molar pregnancy, which tends to progress to Fallopian tube rupture more often than in cases of ectopic non-molar pregnancy. Progression to gestational trophoblastic neoplasia ensures that patients with ectopic molar pregnancy must undergo postmolar monitoring, which must be just as thorough as that of patients with intrauterine hydatidiform moles, even if chemotherapy results in high cure rates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(5):294-299
This report presents the case of a patient with gestational trophoblastic neoplasia after a partial hydatidiform mole formed in the Fallopian tube. Ectopic molar pregnancy is a rare condition, with an estimated incidence of 1 in every 20,000 to 100,000 pregnancies; less than 300 cases of it have been reported in the Western literature. The present report is important because it presents current diagnostic criteria for this rare condition, which has been incorrectly diagnosed in the past, not only morphologically but also immunohistochemically. It also draws the attention of obstetricians to the occurrence of ectopic molar pregnancy, which tends to progress to Fallopian tube rupture more often than in cases of ectopic non-molar pregnancy. Progression to gestational trophoblastic neoplasia ensures that patients with ectopic molar pregnancy must undergo postmolar monitoring, which must be just as thorough as that of patients with intrauterine hydatidiform moles, even if chemotherapy results in high cure rates.