Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):171-173
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):171-173
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(3):171-174
DOI 10.1590/S0100-72031999000300009
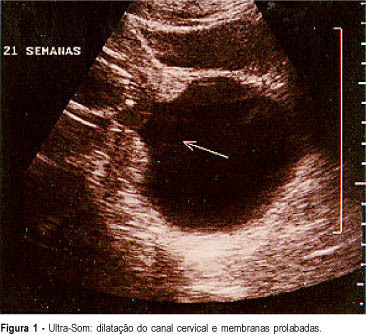
In pregnant women with cervical incompetence in whom there is also dilatation of the cervix and prolapsed membranes there are technical difficulties in performing cerclage in order to prolongate pregnancy until sufficient fetal maturity assures survival of the newborn. We describe a case of cervical incompetence with prolapsed membranes at 21 weeks of gestation, in which we caused the decrease of intrauterine pressure with drainage of amniotic fluid by amniocentesis, until reintroduction of membranes into the uterine cavity was possible. This procedure allowed traction of cervical lips and cerclage with less mechanical trauma, warranting the evolution of pregnancy for 12 weeks and fetal survival
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(3):171-174
DOI 10.1590/S0100-72031999000300009
In pregnant women with cervical incompetence in whom there is also dilatation of the cervix and prolapsed membranes there are technical difficulties in performing cerclage in order to prolongate pregnancy until sufficient fetal maturity assures survival of the newborn. We describe a case of cervical incompetence with prolapsed membranes at 21 weeks of gestation, in which we caused the decrease of intrauterine pressure with drainage of amniotic fluid by amniocentesis, until reintroduction of membranes into the uterine cavity was possible. This procedure allowed traction of cervical lips and cerclage with less mechanical trauma, warranting the evolution of pregnancy for 12 weeks and fetal survival
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):171-179
To evaluate the use of tocolysis in cases of preterm birth due to spontaneous preterm labor in a Brazilian sample.
A sample of 1,491 women with preterm birth due to spontaneous preterm labor were assessed, considering treatment with tocolysis or expectant management, according to gestational age at birth (< 34 weeks and 34 to 36 þ 6 weeks) and drugs prescribed. The study took place in 20 Brazilian hospitals from April 2011 to July 2012. Bivariate analyses were conducted to evaluate associations with sociodemographic and obstetric characteristics and odds ratios with their respective 95% confidence intervals were estimated for maternal and neonatal outcomes.
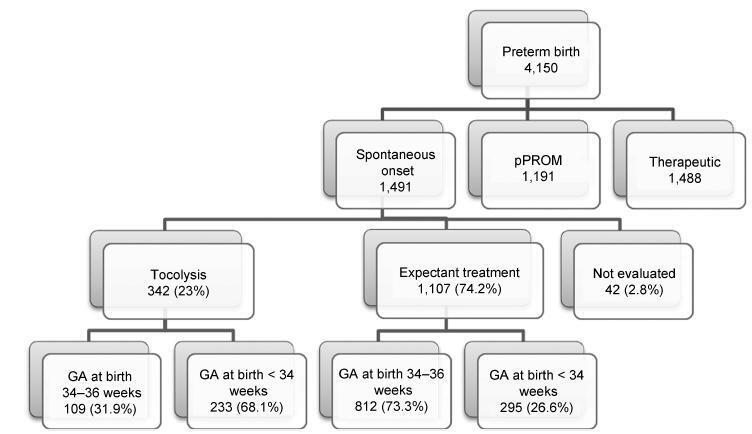
A total of 1,491 cases of preterm birth were considered. Tocolysis was performed in 342 cases (23%), 233 of which (68.1%) were delivered before 34 weeks. Within the expectant management group, 73% was late preterm and with more advanced labor at the time of admission. The most used drugs were calcium channel blockers (62.3%), followed by betamimetics (33%). Among the subjects in the tocolysis group, there were more neonatal and maternal complications (majority non-severe) and an occurrence of corticosteroid use that was 29 higher than in the expectant management group.
Tocolysis is favored in cases of earlier labor and also among thosewith less than 34 weeks of gestation, using preferably calcium channel blockers, with success in achieving increased corticosteroid use. Tocolysis, in general, was related to higher maternal and neonatal complication rates, which may be due to the baseline difference between cases at admission. However, these results should raise awareness to tocolysis use.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(4):171-179
To evaluate the use of tocolysis in cases of preterm birth due to spontaneous preterm labor in a Brazilian sample.
A sample of 1,491 women with preterm birth due to spontaneous preterm labor were assessed, considering treatment with tocolysis or expectant management, according to gestational age at birth (< 34 weeks and 34 to 36 þ 6 weeks) and drugs prescribed. The study took place in 20 Brazilian hospitals from April 2011 to July 2012. Bivariate analyses were conducted to evaluate associations with sociodemographic and obstetric characteristics and odds ratios with their respective 95% confidence intervals were estimated for maternal and neonatal outcomes.
A total of 1,491 cases of preterm birth were considered. Tocolysis was performed in 342 cases (23%), 233 of which (68.1%) were delivered before 34 weeks. Within the expectant management group, 73% was late preterm and with more advanced labor at the time of admission. The most used drugs were calcium channel blockers (62.3%), followed by betamimetics (33%). Among the subjects in the tocolysis group, there were more neonatal and maternal complications (majority non-severe) and an occurrence of corticosteroid use that was 29 higher than in the expectant management group.
Tocolysis is favored in cases of earlier labor and also among thosewith less than 34 weeks of gestation, using preferably calcium channel blockers, with success in achieving increased corticosteroid use. Tocolysis, in general, was related to higher maternal and neonatal complication rates, which may be due to the baseline difference between cases at admission. However, these results should raise awareness to tocolysis use.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):172-177
DOI 10.1590/SO100-720320150005238
To evaluate the presence of podocyturia in chronic hypertensive pregnant women in the third trimester of pregnancy and its possible association with renal disease.
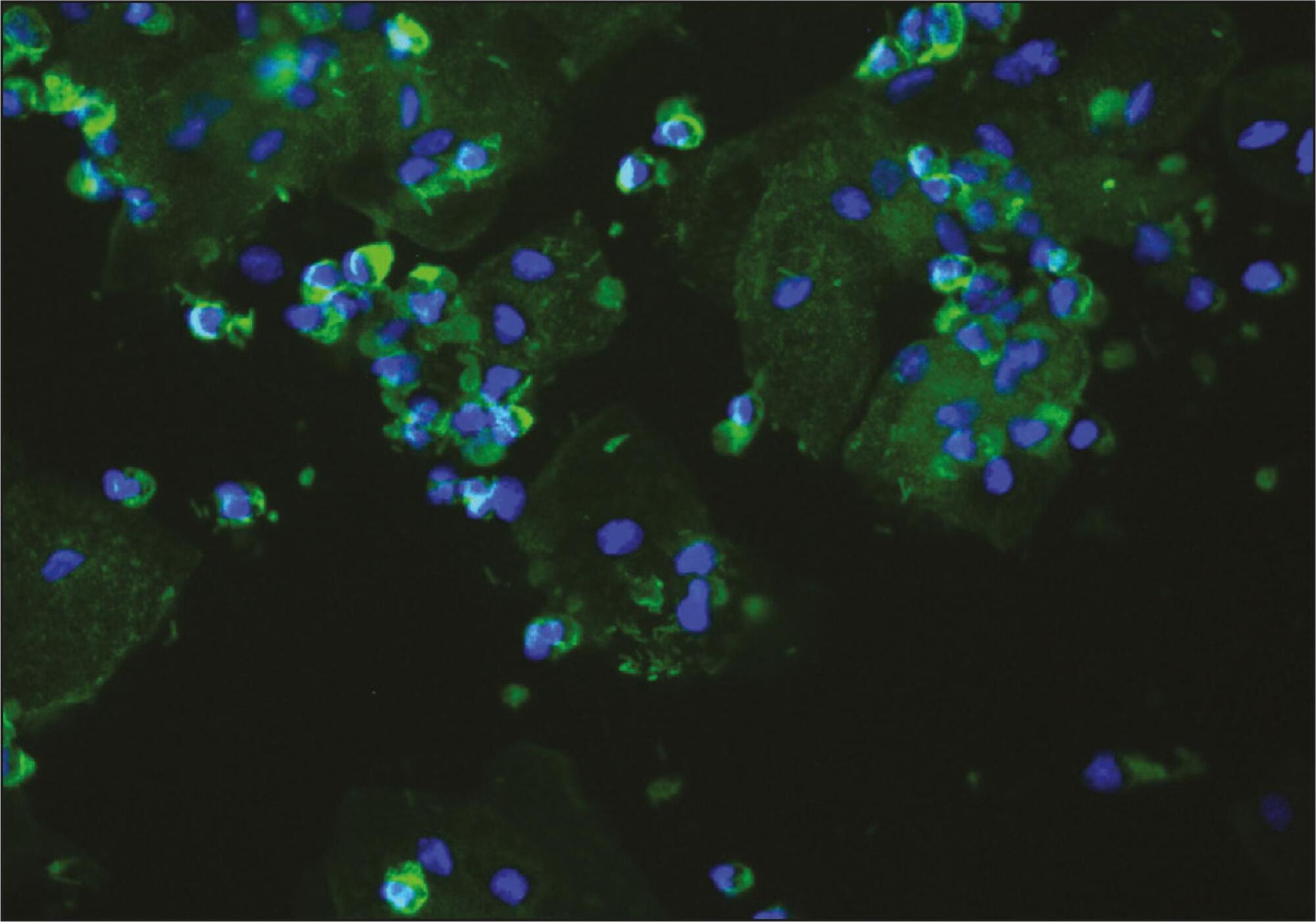
This was an observational study of a convenience sample of 38 chronic hypertensive pregnant women. The podocytes were labeled by the indirect immunofluorescence technique with anti-podocin and diamidino-phenylindole (DAPI). The count was made on 30 random fields analyzed and corrected according to urinary creatinine (podocytes/mg creatinine). The patients were assigned to two groups: NG (normal glomerular function), up to 100 podocytes, and GP (probable glomerulopathy), more than 100 podocytes. Urinary creatinine was measured by the alkaline picrate method. The variables analyzed were body mass index, gestational age, and systolic and diastolic blood pressure at the time of sample collection. Data were analyzed using the SPSS - version 16.0 (IBM - USA). Statistical analysis was performed by the χ2 test, and significant differences were considered when p<0.05.
The median podocyte count was 20.3 (0.0-98.1) for group GN, and 176.9 (109.1-490.6) for GP. The mean body mass index was 30.2 kg/m2 (SD=5.6), mean gestational age was 35.1 weeks (SD=2.5), median systolic blood pressure was 130.0 mmHg (100.0-160.0) and median diastolic blood pressure was 80.0 mmHg (60.0-110.0). There was no significant correlation between podocyturia and body mass index (p=0.305), gestational age (p=0.392), systolic blood pressure (p=0.540) or diastolic blood pressure (p=0.540).
In this study, there was no podocyturia pattern consistent with the presence of active renal disease, although some of the women studied (15.8%) exhibited a significant loss. We believe that it is premature to recommend the inclusion of the determination of podocyturia in routine prenatal clinical practice in chronically hypertensive pregnant women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(4):172-177
DOI 10.1590/SO100-720320150005238
To evaluate the presence of podocyturia in chronic hypertensive pregnant women in the third trimester of pregnancy and its possible association with renal disease.
This was an observational study of a convenience sample of 38 chronic hypertensive pregnant women. The podocytes were labeled by the indirect immunofluorescence technique with anti-podocin and diamidino-phenylindole (DAPI). The count was made on 30 random fields analyzed and corrected according to urinary creatinine (podocytes/mg creatinine). The patients were assigned to two groups: NG (normal glomerular function), up to 100 podocytes, and GP (probable glomerulopathy), more than 100 podocytes. Urinary creatinine was measured by the alkaline picrate method. The variables analyzed were body mass index, gestational age, and systolic and diastolic blood pressure at the time of sample collection. Data were analyzed using the SPSS - version 16.0 (IBM - USA). Statistical analysis was performed by the χ2 test, and significant differences were considered when p<0.05.
The median podocyte count was 20.3 (0.0-98.1) for group GN, and 176.9 (109.1-490.6) for GP. The mean body mass index was 30.2 kg/m2 (SD=5.6), mean gestational age was 35.1 weeks (SD=2.5), median systolic blood pressure was 130.0 mmHg (100.0-160.0) and median diastolic blood pressure was 80.0 mmHg (60.0-110.0). There was no significant correlation between podocyturia and body mass index (p=0.305), gestational age (p=0.392), systolic blood pressure (p=0.540) or diastolic blood pressure (p=0.540).
In this study, there was no podocyturia pattern consistent with the presence of active renal disease, although some of the women studied (15.8%) exhibited a significant loss. We believe that it is premature to recommend the inclusion of the determination of podocyturia in routine prenatal clinical practice in chronically hypertensive pregnant women.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(3):172-177
To evaluate the acceptability of postplacental placement of intrauterine devices (PPIUD), reasons for refusal and suggested policies to increase its use.
Cross-sectional study conducted at the Women Hospital of the Universidade de Campinas, Campinas, SP, Brazil. Postplacental placement of intrauterine devices was offered to women admitted in labor who did not present infections, uterinemalformation, twin pregnancy, preterm birth, and were at least 18 years old. In case of refusal, the parturient was asked to give their reasons and the answers were classified as misinformation about contraception or other reasons. The following were considered misinformation: fear of pain, bleeding, contraception failure and future infertility. Bivariate analysis was performed.
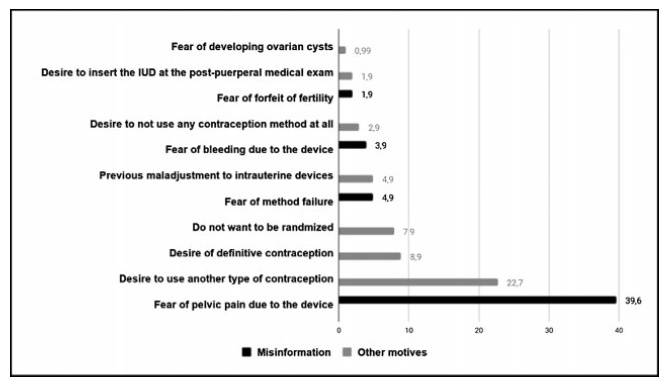
Amongst 241 invited women, the refusal rate was of 41.9%. Misinformation corresponded to 50.5% of all refusals, and the reasons were: fear of pain (39.9%); fear of contraception failure (4.9%); fear of bleeding (3.9%); fear of future infertility (1.9%); other reasons for refusal were 49.5%. Parturients aged between 18 and 27 years old refused the PPIUD more frequently due to misinformation (67.4%), and older parturients (between 28 and 43 years old) refused frequently due to other reasons (63.6%) (p=0.002). Themean age of those who declined the PPIUD due to misinformation was 27.3 ± 6.4 years old, while those who declined for other reasons had a mean age of 29.9 ± 5.9 years old (p=0.017).
The refusal of the PPIUD was high, especially amongst young women and due to misinformation. It is necessary to develop educative measures during antenatal care to counsel women about contraception, reproductive health and consequences of unintended pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(3):172-177
To evaluate the acceptability of postplacental placement of intrauterine devices (PPIUD), reasons for refusal and suggested policies to increase its use.
Cross-sectional study conducted at the Women Hospital of the Universidade de Campinas, Campinas, SP, Brazil. Postplacental placement of intrauterine devices was offered to women admitted in labor who did not present infections, uterinemalformation, twin pregnancy, preterm birth, and were at least 18 years old. In case of refusal, the parturient was asked to give their reasons and the answers were classified as misinformation about contraception or other reasons. The following were considered misinformation: fear of pain, bleeding, contraception failure and future infertility. Bivariate analysis was performed.
Amongst 241 invited women, the refusal rate was of 41.9%. Misinformation corresponded to 50.5% of all refusals, and the reasons were: fear of pain (39.9%); fear of contraception failure (4.9%); fear of bleeding (3.9%); fear of future infertility (1.9%); other reasons for refusal were 49.5%. Parturients aged between 18 and 27 years old refused the PPIUD more frequently due to misinformation (67.4%), and older parturients (between 28 and 43 years old) refused frequently due to other reasons (63.6%) (p=0.002). Themean age of those who declined the PPIUD due to misinformation was 27.3 ± 6.4 years old, while those who declined for other reasons had a mean age of 29.9 ± 5.9 years old (p=0.017).
The refusal of the PPIUD was high, especially amongst young women and due to misinformation. It is necessary to develop educative measures during antenatal care to counsel women about contraception, reproductive health and consequences of unintended pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):174-180
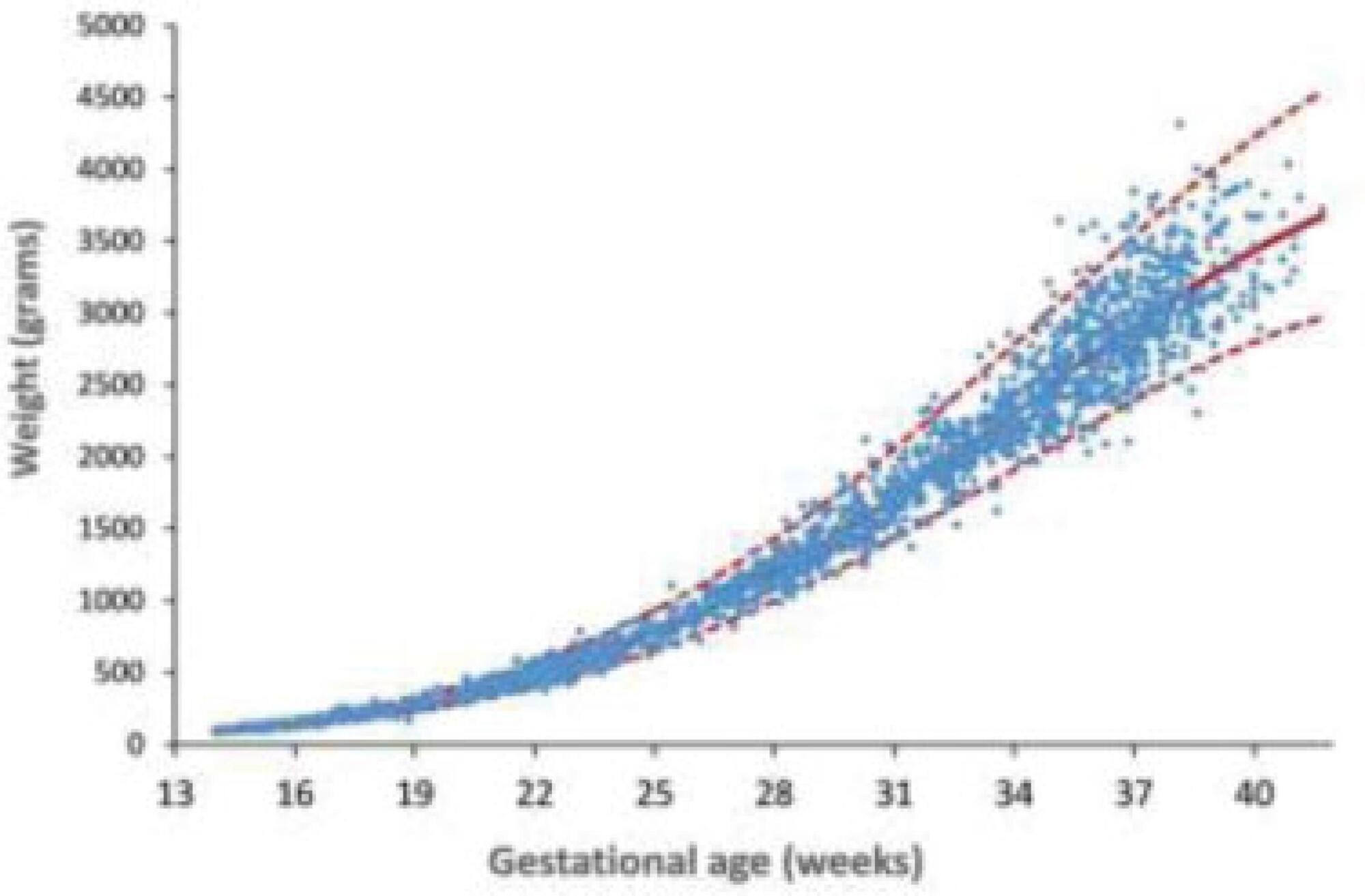
To develop reference curves of estimated fetal weight for a local population in Curitiba, South of Brazil, and compare them with the curves established for other populations.
An observational, cross-sectional, retrospective study was conducted. A reference model for estimated fetal weight was developed using a local sample of 2,211 singleton pregnancies with low risk of growth disorders and well-defined gestational age. This model was compared graphically with the Hadlock and Intergrowth 21st curves.
Reference curves for estimated fetal weight were developed for a local population. The coefficient of determination was R2 = 99.11%, indicating that 99.11% of the fetal weight variations were explained by the model. Compared with Hadlock curves, the 50th, 90th, and 97th percentiles in this model were lower, whereas the 10th percentile nearly overlapped, and the 3rd percentile was slightly higher in the proposed model. The percentiles were higher in the proposed model compared with the Intergrowth 21st curves, particularly for the 3rd, 10th, and 50th percentiles.
We provide a local reference curve for estimated fetal weight. The proposed model was different from other models, and these differences might be due to the use of different populations for model construction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(4):174-180
To develop reference curves of estimated fetal weight for a local population in Curitiba, South of Brazil, and compare them with the curves established for other populations.
An observational, cross-sectional, retrospective study was conducted. A reference model for estimated fetal weight was developed using a local sample of 2,211 singleton pregnancies with low risk of growth disorders and well-defined gestational age. This model was compared graphically with the Hadlock and Intergrowth 21st curves.
Reference curves for estimated fetal weight were developed for a local population. The coefficient of determination was R2 = 99.11%, indicating that 99.11% of the fetal weight variations were explained by the model. Compared with Hadlock curves, the 50th, 90th, and 97th percentiles in this model were lower, whereas the 10th percentile nearly overlapped, and the 3rd percentile was slightly higher in the proposed model. The percentiles were higher in the proposed model compared with the Intergrowth 21st curves, particularly for the 3rd, 10th, and 50th percentiles.
We provide a local reference curve for estimated fetal weight. The proposed model was different from other models, and these differences might be due to the use of different populations for model construction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(4):174-180
DOI 10.1590/S0100-72032005000400003
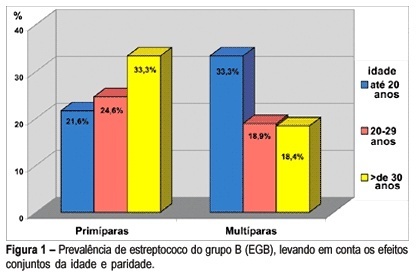
PURPOSE: to determine the prevalence of group B Streptococcus (GBS) in pregnant women in the third trimester of pregnancy and explore the factors potentially associated with colonization. METHODS: a sample of 273 pregnant women in the third trimester of pregnancy, from the prenatal care center in Southern Brasil, was investigated. Vaginal and anorectal samples were collected and innoculated in Todd-Hewitt selective broth supplemented with 10 µg/mL colistin and 15 µg/mL nalidixic acid and afterwards cultured on defibrinated sheep blood agar plates. All suspected colonies were submitted to the agglutination test for detection of the specific group B antigen. The Camp test was used for GBS identification in non-hemolytic varieties. Demographic, socioeconomic, reproductive, and clinico-obstetric data were also analyzed. Prevalence ratio (PR) was used as risk measurement. Confidence interval was considered significant at the level of 95% (alpha=0.05). RESULTS: prevalence of Streptococcus (GBS) colonization amounted to 21.6% (59), 9.9% (27) of pregnant women showing positivity in both sites; vaginal site colonization was found in 6.95% (19) of the women and 4.75% (13) of the samples showed positivity only in the anal site. GBS prevalence was slightly higher in pregnant women under 20 years, in those with less schooling and in primiparae and was twice as high among those who did not reported spontaneous abortion, but with no statistical significance. No difference was found in GBS prevalence according to the history of sexually transmittted diseases and tabagism. When analyzed together, the factors detected as potentially associated with colonization by GBS were: primiparae over 30 years (PR=1.55) and women with more than one sexual partner and increased frequency of sexual activity (p<0.05) (55,6 vs 20.5%; p<0.05). No difference regarding prevalence was found to exist in relation to the history of sexually transmitted diseases, previous spontaneous abortion and tabagism. CONCLUSION: these results confirm the need for routine collection for GBS culture from both sites (vaginal and anal) in all pregnant women in the third trimester of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(4):174-180
DOI 10.1590/S0100-72032005000400003
PURPOSE: to determine the prevalence of group B Streptococcus (GBS) in pregnant women in the third trimester of pregnancy and explore the factors potentially associated with colonization. METHODS: a sample of 273 pregnant women in the third trimester of pregnancy, from the prenatal care center in Southern Brasil, was investigated. Vaginal and anorectal samples were collected and innoculated in Todd-Hewitt selective broth supplemented with 10 µg/mL colistin and 15 µg/mL nalidixic acid and afterwards cultured on defibrinated sheep blood agar plates. All suspected colonies were submitted to the agglutination test for detection of the specific group B antigen. The Camp test was used for GBS identification in non-hemolytic varieties. Demographic, socioeconomic, reproductive, and clinico-obstetric data were also analyzed. Prevalence ratio (PR) was used as risk measurement. Confidence interval was considered significant at the level of 95% (alpha=0.05). RESULTS: prevalence of Streptococcus (GBS) colonization amounted to 21.6% (59), 9.9% (27) of pregnant women showing positivity in both sites; vaginal site colonization was found in 6.95% (19) of the women and 4.75% (13) of the samples showed positivity only in the anal site. GBS prevalence was slightly higher in pregnant women under 20 years, in those with less schooling and in primiparae and was twice as high among those who did not reported spontaneous abortion, but with no statistical significance. No difference was found in GBS prevalence according to the history of sexually transmittted diseases and tabagism. When analyzed together, the factors detected as potentially associated with colonization by GBS were: primiparae over 30 years (PR=1.55) and women with more than one sexual partner and increased frequency of sexual activity (p<0.05) (55,6 vs 20.5%; p<0.05). No difference regarding prevalence was found to exist in relation to the history of sexually transmitted diseases, previous spontaneous abortion and tabagism. CONCLUSION: these results confirm the need for routine collection for GBS culture from both sites (vaginal and anal) in all pregnant women in the third trimester of pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):174-181
DOI 10.1590/S0100-72032011000800002
PURPOSE: To describe the maternal and perinatal outcomes of pregnant women diagnosed with leukemia who were followed up for prenatal care and delivery at a university hospital. METHODS: A retrospective study of the period from 2001 to 2011, which included 16 pregnant women with a diagnosis of leukemia followed by antenatal care specialists in hematological diseases and pregnancy. For acute leukemia diagnosed after the first trimester, the recommendation was to perform chemotherapy despite the current pregnancy. For chronic leukemia, patients who were controlled in hematological terms were maintained without medication during pregnancy, or chemotherapy was introduced after the first trimester. We analyzed the maternal and perinatal outcome. RESULTS: Acute lymphoblastic leukemia (ALL) was diagnosed in five cases (31.3%), acute myeloid leukemia (AML) in two cases (12.5%) and chronic myeloid leukemia (CML) in nine cases (56.3%). Of the cases of acute leukemia, two (28.6%) were diagnosed in the first trimester, two (28.6%) in the second and three (42.9%) in the third. Two patients with ALL diagnosed in the first trimester opted for therapeutic abortion. Four patients with acute leukemia received chemotherapy during pregnancy, with a diagnosis established after the 20th week. In one case of ALL with a late diagnosis (30 weeks), chemotherapy was started after delivery. All pregnant women with acute leukemia developed anemia and thrombocytopenia, and four (57.1%) developed febrile neutropenia. Of nine pregnant women with CML, four were treated with imatinib mesylate when they became pregnant, with treatment being interrupted in the first trimester in three of them and in the second trimester in one. During pregnancy, three patients (33.3%) required no chemotherapy after discontinuation of imatinib, and six (66.7%) were treated with the following drugs: interferon (n=5) and/or hydroxyurea (n=3 ). In the group of pregnant women with CML, anemia occurred in four (44.4%) cases and thrombocytopenia in one (11.1%). The perinatal outcomes of pregnancies complicated by acute leukemia were as follows: mean gestational age at delivery was 32 weeks (standard deviation - SD=4.4) and the mean birth weight was 1476 g (SD=657 g), there were 2 (40.0%) perinatal deaths (a fetal one and a neonatal one). In pregnancies complicated by CML, the mean gestational age at delivery was 37.6 weeks (SD=1.1) and the mean birth weight was 2870 g (SD=516 g). There was no perinatal death and no fetal abnormality was detected. CONCLUSIONS: Maternal and fetal morbidity is high in pregnancies complicated by acute leukemia. Whereas, in pregnancies complicated by CML, the maternal and fetal prognosis appears to be more favorable, with greater ease in management of complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(8):174-181
DOI 10.1590/S0100-72032011000800002
PURPOSE: To describe the maternal and perinatal outcomes of pregnant women diagnosed with leukemia who were followed up for prenatal care and delivery at a university hospital. METHODS: A retrospective study of the period from 2001 to 2011, which included 16 pregnant women with a diagnosis of leukemia followed by antenatal care specialists in hematological diseases and pregnancy. For acute leukemia diagnosed after the first trimester, the recommendation was to perform chemotherapy despite the current pregnancy. For chronic leukemia, patients who were controlled in hematological terms were maintained without medication during pregnancy, or chemotherapy was introduced after the first trimester. We analyzed the maternal and perinatal outcome. RESULTS: Acute lymphoblastic leukemia (ALL) was diagnosed in five cases (31.3%), acute myeloid leukemia (AML) in two cases (12.5%) and chronic myeloid leukemia (CML) in nine cases (56.3%). Of the cases of acute leukemia, two (28.6%) were diagnosed in the first trimester, two (28.6%) in the second and three (42.9%) in the third. Two patients with ALL diagnosed in the first trimester opted for therapeutic abortion. Four patients with acute leukemia received chemotherapy during pregnancy, with a diagnosis established after the 20th week. In one case of ALL with a late diagnosis (30 weeks), chemotherapy was started after delivery. All pregnant women with acute leukemia developed anemia and thrombocytopenia, and four (57.1%) developed febrile neutropenia. Of nine pregnant women with CML, four were treated with imatinib mesylate when they became pregnant, with treatment being interrupted in the first trimester in three of them and in the second trimester in one. During pregnancy, three patients (33.3%) required no chemotherapy after discontinuation of imatinib, and six (66.7%) were treated with the following drugs: interferon (n=5) and/or hydroxyurea (n=3 ). In the group of pregnant women with CML, anemia occurred in four (44.4%) cases and thrombocytopenia in one (11.1%). The perinatal outcomes of pregnancies complicated by acute leukemia were as follows: mean gestational age at delivery was 32 weeks (standard deviation - SD=4.4) and the mean birth weight was 1476 g (SD=657 g), there were 2 (40.0%) perinatal deaths (a fetal one and a neonatal one). In pregnancies complicated by CML, the mean gestational age at delivery was 37.6 weeks (SD=1.1) and the mean birth weight was 2870 g (SD=516 g). There was no perinatal death and no fetal abnormality was detected. CONCLUSIONS: Maternal and fetal morbidity is high in pregnancies complicated by acute leukemia. Whereas, in pregnancies complicated by CML, the maternal and fetal prognosis appears to be more favorable, with greater ease in management of complications.