You searched for:"Geraldo Duarte"
We found (52) results for your search.Summary
Rev Bras Ginecol Obstet. 2005;27(12):768-778
DOI 10.1590/S0100-72032005001200010
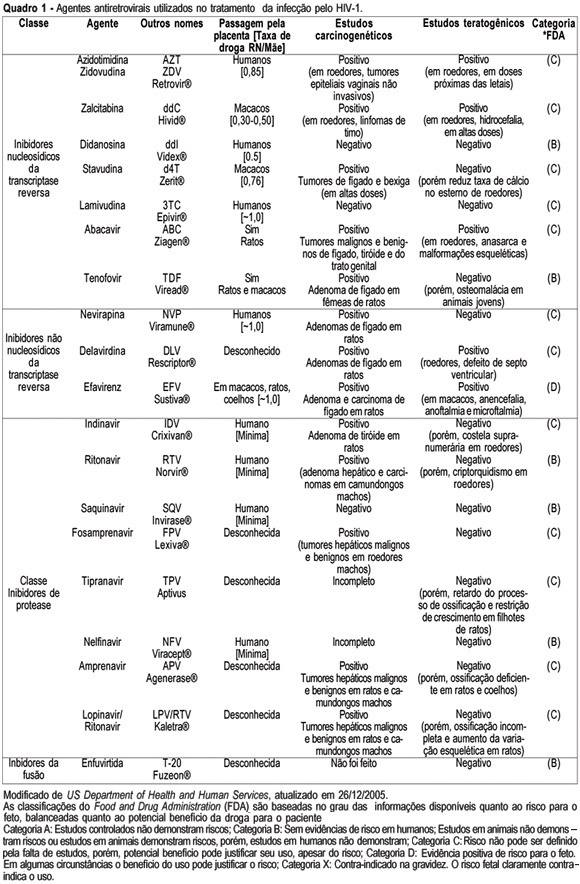
Knowledge about the factors or situations that influence the vertical transmission (VT) of human immunodeficiency type 1 (HIV-1) has led to the implementation of strategies which have promoted a rate decline along the years, from 40% to less than 3% nowadays. One of the major advances in the area has been the prophylactic administration of zidovudine (AZT), in the prenatal phase (oral route), in the predelivery phase (intravenous route) and to the newborn (oral route). This intervention may reduce HIV-1 VT 68%, thus being the most effective isolated strategy used so far. In the chronological sequence of advances, it has been observed that a high viral load is the main risk indicator for this type of transmission. As AZT does not reduce the viral load and does not control the residual rate observed in HIV-1 VT, the use of prophylactic schemes using three antiretroviral drugs has been encouraged. Elective caesarean section completes the range of obstetric strategies with major impact on the reduction of HIV-1 VT. Its effectiveness is linked to the observation of the criteria for its indication: viral load assessed after the 34th week of pregnancy with levels over 1000 copies/mL, gestation over 38 weeks confirmed by ultrasonography, intact chorioamniotic membranes, and performed before labor has started. In cases where normal delivery is indicated, it should be remembered that prolonged chorioamniorrhexis, invasive manipulation of the fetus, delivery with instruments and episiotomy are situations to be avoided. Among the postnatal interventions considered important for the reduction of HIV-1 VT are: pediatric reception (this should be done by trained professionals, avoiding microtraumas in the mucosa during the sucking maneuvers, use of neonatal AZT (for a period of six weeks) and bottle feeding. Special attention should be given to the orientation for the mother, in order to prevent acute infection by HIV-1 in this period, what would markedly increase virus VT rate.
Summary
Rev Bras Ginecol Obstet. 2005;27(12):768-778
DOI 10.1590/S0100-72032005001200010
Knowledge about the factors or situations that influence the vertical transmission (VT) of human immunodeficiency type 1 (HIV-1) has led to the implementation of strategies which have promoted a rate decline along the years, from 40% to less than 3% nowadays. One of the major advances in the area has been the prophylactic administration of zidovudine (AZT), in the prenatal phase (oral route), in the predelivery phase (intravenous route) and to the newborn (oral route). This intervention may reduce HIV-1 VT 68%, thus being the most effective isolated strategy used so far. In the chronological sequence of advances, it has been observed that a high viral load is the main risk indicator for this type of transmission. As AZT does not reduce the viral load and does not control the residual rate observed in HIV-1 VT, the use of prophylactic schemes using three antiretroviral drugs has been encouraged. Elective caesarean section completes the range of obstetric strategies with major impact on the reduction of HIV-1 VT. Its effectiveness is linked to the observation of the criteria for its indication: viral load assessed after the 34th week of pregnancy with levels over 1000 copies/mL, gestation over 38 weeks confirmed by ultrasonography, intact chorioamniotic membranes, and performed before labor has started. In cases where normal delivery is indicated, it should be remembered that prolonged chorioamniorrhexis, invasive manipulation of the fetus, delivery with instruments and episiotomy are situations to be avoided. Among the postnatal interventions considered important for the reduction of HIV-1 VT are: pediatric reception (this should be done by trained professionals, avoiding microtraumas in the mucosa during the sucking maneuvers, use of neonatal AZT (for a period of six weeks) and bottle feeding. Special attention should be given to the orientation for the mother, in order to prevent acute infection by HIV-1 in this period, what would markedly increase virus VT rate.
Summary
Rev Bras Ginecol Obstet. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
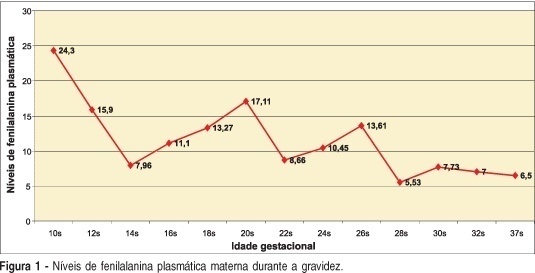
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.
Summary
Rev Bras Ginecol Obstet. 2004;26(10):813-817
DOI 10.1590/S0100-72032004001000009
Maternal phenylketonuria is an aminoacid pathology characterized by elevated plasma levels of phenylalanine in the pregnant woman that may cause abnormalities in fetus development, and which is called maternal phenylketonuria syndrome. As the clinical manifestations are non-specific, the disease should be diagnosed by laboratory screening. We present a case of a second pregnancy in a woman with a history of psycho-cognitive development retardation without previous obstetric history, with diagnosis of phenylketonuria in the present gestation, treated with specific phenylalanine-free diet. The newborn did not present congenital defects. The previous gestation without maternal treatment resulted in a child with serious developmental disturbances, microcephalia and auditory-speaking deficits. Early diagnosis and treatment of hyperphenylalaninemia during pregnancy are essential, mainly because of the negative impact on fetal development. In the here reported case, there were fetal benefits from the maternal dietary treatment, which demonstrates the importance of the maternal diagnosis of phenylketonuria in women in reproductive age.
Summary
Rev Bras Ginecol Obstet. 2005;27(2):92-97
DOI 10.1590/S0100-72032005000200009
Visceral leishmaniasis (VL) is an endemic disease in the state of Mato Grosso do Sul, Brazil, mainly in the areas near the Paraguay and Paraná rivers. An increasing number of cases have been occurring especially in the state capital Campo Grande, with consequent occurrence of VL cases in pregnant women. This situation causes an elevated risk of vertical transmission of the parasite. In this report, we describe a case of VL in a pregnant woman followed up by our group, who was treated with liposomal amphotericin B, with no vertical transmission of the parasite. In our report, we demonstrate a therapeutic option for kala-azar during pregnancy, since antimoniate, the first-choice drug, is not prescribed during the gestational period.
Summary
Rev Bras Ginecol Obstet. 2005;27(2):92-97
DOI 10.1590/S0100-72032005000200009
Visceral leishmaniasis (VL) is an endemic disease in the state of Mato Grosso do Sul, Brazil, mainly in the areas near the Paraguay and Paraná rivers. An increasing number of cases have been occurring especially in the state capital Campo Grande, with consequent occurrence of VL cases in pregnant women. This situation causes an elevated risk of vertical transmission of the parasite. In this report, we describe a case of VL in a pregnant woman followed up by our group, who was treated with liposomal amphotericin B, with no vertical transmission of the parasite. In our report, we demonstrate a therapeutic option for kala-azar during pregnancy, since antimoniate, the first-choice drug, is not prescribed during the gestational period.
Summary
Rev Bras Ginecol Obstet. 2008;30(2):93-100
DOI 10.1590/S0100-72032008000200008
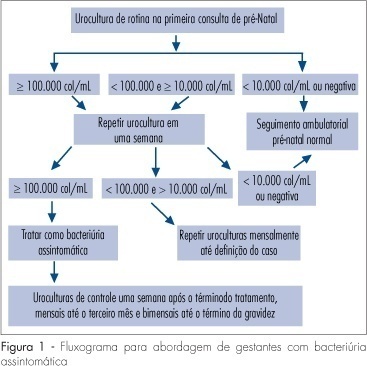
Several factors cause urinary tract infection (UTI) to be a relevant complication of the gestational period, aggravating both the maternal and perinatal prognosis. For many years, pregnancy has been considered to be a factor predisposing to all forms of UTI. Today, it is known that pregnancy, as an isolated event, is not responsible for a higher incidence of UTI, but that the anatomical and physiological changes imposed on the urinary tract by pregnancy predispose women with asymptomatic bacteriuria (AB) to become pregnant women with symptomatic UTI. AB affects 2 to 10% of all pregnant women and approximately 30% of these will develop pyelonephritis if not properly treated. However, a difficult to understand resistance against the identification of AB during this period is observed among prenatalists. The diagnosis of UTI is microbiological and it is based on two urine cultures presenting more than 10(5) colonies/mL urine of the same germ. Treatment is facilitated by the fact that it is based on an antibiogram, with no scientific foundation for the notion that a pre-established therapeutic scheme is an adequate measure. For the treatment of pyelonephritis, it is not possible to wait for the result of culture and previous knowledge of the resistance profile of the antibacterial agents available for the treatment of pregnant women would be the best measure. Another important variable is the use of an intravenous bactericidal antibiotic during the acute phase, with the possibility of oral administration at home after clinical improvement of the patient. At our hospital, the drug that best satisfies all of these requirements is cefuroxime, administered for 10-14 days. Third-generation cephalosporins do not exist in the oral form, all of them involving the inconvenience of parenteral administration. In view of their side effects, aminoglycosides are considered to be inadequate for administration to pregnant women. The inconsistent insinuation of contraindication of monofluorinated quinolones, if there is an indication, norfloxacin is believed to be a good alternative to cefuroxime. In cases in which UTI prophylaxis is indicated, chemotherapeutic agents are preferred, among them nitrofurantoin, with care taken to avoid its use at the end of pregnancy due to the risk of kernicterus for the neonate.
Summary
Rev Bras Ginecol Obstet. 2008;30(2):93-100
DOI 10.1590/S0100-72032008000200008
Several factors cause urinary tract infection (UTI) to be a relevant complication of the gestational period, aggravating both the maternal and perinatal prognosis. For many years, pregnancy has been considered to be a factor predisposing to all forms of UTI. Today, it is known that pregnancy, as an isolated event, is not responsible for a higher incidence of UTI, but that the anatomical and physiological changes imposed on the urinary tract by pregnancy predispose women with asymptomatic bacteriuria (AB) to become pregnant women with symptomatic UTI. AB affects 2 to 10% of all pregnant women and approximately 30% of these will develop pyelonephritis if not properly treated. However, a difficult to understand resistance against the identification of AB during this period is observed among prenatalists. The diagnosis of UTI is microbiological and it is based on two urine cultures presenting more than 10(5) colonies/mL urine of the same germ. Treatment is facilitated by the fact that it is based on an antibiogram, with no scientific foundation for the notion that a pre-established therapeutic scheme is an adequate measure. For the treatment of pyelonephritis, it is not possible to wait for the result of culture and previous knowledge of the resistance profile of the antibacterial agents available for the treatment of pregnant women would be the best measure. Another important variable is the use of an intravenous bactericidal antibiotic during the acute phase, with the possibility of oral administration at home after clinical improvement of the patient. At our hospital, the drug that best satisfies all of these requirements is cefuroxime, administered for 10-14 days. Third-generation cephalosporins do not exist in the oral form, all of them involving the inconvenience of parenteral administration. In view of their side effects, aminoglycosides are considered to be inadequate for administration to pregnant women. The inconsistent insinuation of contraindication of monofluorinated quinolones, if there is an indication, norfloxacin is believed to be a good alternative to cefuroxime. In cases in which UTI prophylaxis is indicated, chemotherapeutic agents are preferred, among them nitrofurantoin, with care taken to avoid its use at the end of pregnancy due to the risk of kernicterus for the neonate.