You searched for:"Geraldo Duarte"
We found (53) results for your search.Summary
Rev Bras Ginecol Obstet. 2018;40(1):54-55
Summary
Rev Bras Ginecol Obstet. 2018;40(1):54-55
Summary
Rev Bras Ginecol Obstet. 2021;43(8):585-587
Summary
Rev Bras Ginecol Obstet. 2021;43(8):585-587
Summary
Rev Bras Ginecol Obstet. 2003;25(8):593-598
DOI 10.1590/S0100-72032003000800008
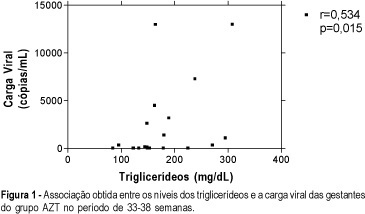
PURPOSE: to investigate the effect of antiretroviral drugs on the lipid metabolism in HIV-infected pregnant women. METHODS: a prospective study was conducted on 57 pregnant women. The women were divided into three groups: ZDV group, consisting of 20 HIV-infected women taking ZDV; TT group, consisting of 25 HIV-1-infected women on triple antiretroviral treatment (ZDV + 3TC + NFV), and control group, consisting of 12 pregnant women considered to be normal from a clinical and laboratory viewpoint. Demographic and anthropometric data were homogeneous. Patients with a personal and family history of hyperlipidemia were excluded. Blood samples were obtained for the determination of fasting lipids (total cholesterol, LDL and HDL, and triglycerides) at four periods during pregnancy (1st = 14-20 weeks; 2nd = 21-26 weeks; 3rd = 27-32 weeks and 4th = 33-38 weeks). Data were analyzed statistically using the nonparametric chi², Friedman and Kruskal-Wallis tests . RESULTS: the use of antiretroviral drugs during pregnancy induced no difference in total or HDL cholesterol but caused an increase from 76.5 and 84 mg/dL to 96 and 105 mg/dL in the concentration of the LDL fraction along gestation in ZDV and TT groups, respectively (p<0.01). A positive significant association was observed between triglycerides and viral burden in the ZDV group (r: 0.534; p=0.015). CONCLUSION: Antiretroviral agents during pregnancy increase serum LDL-colesterol levels. The risk of pregnancy regarding potentiation of long-term antiretroviral effects on lipid metabolism, remains to be established.
Summary
Rev Bras Ginecol Obstet. 2003;25(8):593-598
DOI 10.1590/S0100-72032003000800008
PURPOSE: to investigate the effect of antiretroviral drugs on the lipid metabolism in HIV-infected pregnant women. METHODS: a prospective study was conducted on 57 pregnant women. The women were divided into three groups: ZDV group, consisting of 20 HIV-infected women taking ZDV; TT group, consisting of 25 HIV-1-infected women on triple antiretroviral treatment (ZDV + 3TC + NFV), and control group, consisting of 12 pregnant women considered to be normal from a clinical and laboratory viewpoint. Demographic and anthropometric data were homogeneous. Patients with a personal and family history of hyperlipidemia were excluded. Blood samples were obtained for the determination of fasting lipids (total cholesterol, LDL and HDL, and triglycerides) at four periods during pregnancy (1st = 14-20 weeks; 2nd = 21-26 weeks; 3rd = 27-32 weeks and 4th = 33-38 weeks). Data were analyzed statistically using the nonparametric chi², Friedman and Kruskal-Wallis tests . RESULTS: the use of antiretroviral drugs during pregnancy induced no difference in total or HDL cholesterol but caused an increase from 76.5 and 84 mg/dL to 96 and 105 mg/dL in the concentration of the LDL fraction along gestation in ZDV and TT groups, respectively (p<0.01). A positive significant association was observed between triglycerides and viral burden in the ZDV group (r: 0.534; p=0.015). CONCLUSION: Antiretroviral agents during pregnancy increase serum LDL-colesterol levels. The risk of pregnancy regarding potentiation of long-term antiretroviral effects on lipid metabolism, remains to be established.
Summary
Rev Bras Ginecol Obstet. 2010;32(2):61-65
DOI 10.1590/S0100-72032010000200002
PURPOSE: to analyze the occurrence of conjoined twins at a tertiary perinatology reference university hospital over a period of 25 years (January 1982 to January 2007) and to describe the successful separation of one of the pairs. METHODS: we consulted retrospectively the database of the University Hospital of the Medical School of Ribeirão Preto, University of São Paulo, Brazil, in order to determine the number of pairs of conjoined twins, their frequency, classification, gender, type of pregnancy resolution, attempted surgical separation, prenatal diagnosis and survival. RESULTS: we detected 14 pairs of conjoined twins (1/22,284 live births and 1/90 pairs of twin live births) born during this period (six males, seven females and one of indeterminate sex). The prenatal diagnosis was performed in all twins and all births were accomplished by cesarean section. The separation was possible in only one pair, which survives in excellent health conditions after eight years. Of the remaining 13, ten died on the day of birth and three survived only a few months (less than one year). CONCLUSION: Although our study revealed an abnormally high number of conjoined twins, this is a rare phenomenon, with a poor perinatal prognosis depending on the organs shared by the twins and associated malformations, especially those related to the fetal heart. Due to the poor prognosis of these pairs and to the maternal reproductive impairment caused by the need to perform body cesareans, we suggest that, based on these numbers, early interruption of these pregnancies be legally granted, as in the case of other diseases incompatible with fetal survival outside the uterus. Thus, the confirmation of a diagnosis of conjoined twins and the resolution of pregnancy should be performed at a tertiary obstetric and perinatal care center, and an authorization for the interruption of pregnancy should be obtained by judicial means.
Summary
Rev Bras Ginecol Obstet. 2010;32(2):61-65
DOI 10.1590/S0100-72032010000200002
PURPOSE: to analyze the occurrence of conjoined twins at a tertiary perinatology reference university hospital over a period of 25 years (January 1982 to January 2007) and to describe the successful separation of one of the pairs. METHODS: we consulted retrospectively the database of the University Hospital of the Medical School of Ribeirão Preto, University of São Paulo, Brazil, in order to determine the number of pairs of conjoined twins, their frequency, classification, gender, type of pregnancy resolution, attempted surgical separation, prenatal diagnosis and survival. RESULTS: we detected 14 pairs of conjoined twins (1/22,284 live births and 1/90 pairs of twin live births) born during this period (six males, seven females and one of indeterminate sex). The prenatal diagnosis was performed in all twins and all births were accomplished by cesarean section. The separation was possible in only one pair, which survives in excellent health conditions after eight years. Of the remaining 13, ten died on the day of birth and three survived only a few months (less than one year). CONCLUSION: Although our study revealed an abnormally high number of conjoined twins, this is a rare phenomenon, with a poor perinatal prognosis depending on the organs shared by the twins and associated malformations, especially those related to the fetal heart. Due to the poor prognosis of these pairs and to the maternal reproductive impairment caused by the need to perform body cesareans, we suggest that, based on these numbers, early interruption of these pregnancies be legally granted, as in the case of other diseases incompatible with fetal survival outside the uterus. Thus, the confirmation of a diagnosis of conjoined twins and the resolution of pregnancy should be performed at a tertiary obstetric and perinatal care center, and an authorization for the interruption of pregnancy should be obtained by judicial means.

Summary
Rev Bras Ginecol Obstet. 2005;27(2):64-68
DOI 10.1590/S0100-72032005000200004
PURPOSE: to determine the frequency of Mycoplasma hominis and Ureaplasma urealyticum infection, and relate it to the associated clinical variables of infertile women. METHODS: transversal study involving 322 infertile women, submitted to collection of endocervix swab for research of Mycoplasma hominis and Ureaplasma urealyticum infecction, from October 2002 to May 2004. All patients were submitted to a basic infertility investigation protocol. As control, a historical series of 51 non-pregnant women previously investigated as for the studied infectious agents, was used. RESULTS: the frequency of Mycoplasma hominis and Ureaplasma urealyticum infection was 4.9% in the infertile women and 13.8% in the control group. Among the infertile patients, a relationship between the presence of the two agents and changes in the histerosalpingography result (OR: 3.20; IC 95%: 1.05-9.73), presence of dyspareunia (OR: 10.72; IC 95%: 3.21-35.77) and vaginal discharge (OR: 8.5; IC 95%: 2.83-26.02), besides endocervical culture positive for Escherichia coli (OR: 6.09; IC 95%: 4.95-52.25) was observed. CONCLUSION: Mycoplasma hominis and Ureaplasma urealyticum infection rate is low in infertile patients and is associated with reproductive sequels.
Summary
Rev Bras Ginecol Obstet. 2005;27(2):64-68
DOI 10.1590/S0100-72032005000200004
PURPOSE: to determine the frequency of Mycoplasma hominis and Ureaplasma urealyticum infection, and relate it to the associated clinical variables of infertile women. METHODS: transversal study involving 322 infertile women, submitted to collection of endocervix swab for research of Mycoplasma hominis and Ureaplasma urealyticum infecction, from October 2002 to May 2004. All patients were submitted to a basic infertility investigation protocol. As control, a historical series of 51 non-pregnant women previously investigated as for the studied infectious agents, was used. RESULTS: the frequency of Mycoplasma hominis and Ureaplasma urealyticum infection was 4.9% in the infertile women and 13.8% in the control group. Among the infertile patients, a relationship between the presence of the two agents and changes in the histerosalpingography result (OR: 3.20; IC 95%: 1.05-9.73), presence of dyspareunia (OR: 10.72; IC 95%: 3.21-35.77) and vaginal discharge (OR: 8.5; IC 95%: 2.83-26.02), besides endocervical culture positive for Escherichia coli (OR: 6.09; IC 95%: 4.95-52.25) was observed. CONCLUSION: Mycoplasma hominis and Ureaplasma urealyticum infection rate is low in infertile patients and is associated with reproductive sequels.
Summary
Rev Bras Ginecol Obstet. 2002;24(10):647-652
DOI 10.1590/S0100-72032002001000003
PURPOSE: to evaluate experimentally the effects of antiretroviral drugs used alone and in association upon the fertility of pregnant Wistar rats and the perinatal effects on the offspring. METHODS: adult female pregnant Wistar rats weighing 200-230 g were used. The antiretroviral drugs zidovudine (AZT), lamivudine (3TC) and nelfinavir (NFV) were used alone and in association at daily doses of ten times the dose normally used in pregnant women, proportionally to the animal's body weight. Seven groups were studied, including the control one. The experiment started on day 0 and the pregnant animals were sacrificed on day 21. The alive and dead fetuses, the total implantation sites and the total numbers of corporea lutea were used to calculate the fertility values. The statistical analysis was performed by Student's t test and by the Mann-Whitney test. RESULTS: there were no significant statistical differences regarding preimplantation loss and implantation efficiency values of the rats treated with isolated and associated antiretroviral drugs. There was a significant increase in the postimplantation loss values (control group: 7.6%; drug groups variation: 20.2-26.7%), a decrease in the fetal viability values (control group: 92.4%, drug groups variation: 73.3-79.8%), and a decreasing number of fetuses per animal (control group: 14.7; drug groups variation: 11.1-12.7). There was a significant weight reduction of the female rats and of the offspring of animals treated with 3TC, AZT + 3TC and AZT + 3TC + NFV. CONCLUSION: with the administration of high antiretroviral doses, important fertility effects could be observed, which showed that less histotoxic antiretroviral drugs must be studied in order to warrant the safety of using these medicines in pregnant HIV-1 - infected women.
Summary
Rev Bras Ginecol Obstet. 2002;24(10):647-652
DOI 10.1590/S0100-72032002001000003
PURPOSE: to evaluate experimentally the effects of antiretroviral drugs used alone and in association upon the fertility of pregnant Wistar rats and the perinatal effects on the offspring. METHODS: adult female pregnant Wistar rats weighing 200-230 g were used. The antiretroviral drugs zidovudine (AZT), lamivudine (3TC) and nelfinavir (NFV) were used alone and in association at daily doses of ten times the dose normally used in pregnant women, proportionally to the animal's body weight. Seven groups were studied, including the control one. The experiment started on day 0 and the pregnant animals were sacrificed on day 21. The alive and dead fetuses, the total implantation sites and the total numbers of corporea lutea were used to calculate the fertility values. The statistical analysis was performed by Student's t test and by the Mann-Whitney test. RESULTS: there were no significant statistical differences regarding preimplantation loss and implantation efficiency values of the rats treated with isolated and associated antiretroviral drugs. There was a significant increase in the postimplantation loss values (control group: 7.6%; drug groups variation: 20.2-26.7%), a decrease in the fetal viability values (control group: 92.4%, drug groups variation: 73.3-79.8%), and a decreasing number of fetuses per animal (control group: 14.7; drug groups variation: 11.1-12.7). There was a significant weight reduction of the female rats and of the offspring of animals treated with 3TC, AZT + 3TC and AZT + 3TC + NFV. CONCLUSION: with the administration of high antiretroviral doses, important fertility effects could be observed, which showed that less histotoxic antiretroviral drugs must be studied in order to warrant the safety of using these medicines in pregnant HIV-1 - infected women.
Summary
Rev Bras Ginecol Obstet. 2007;29(12):647-653
DOI 10.1590/S0100-72032007001200008
Screening for major chromosomal abnormalities can be provided in the first trimester of pregnancy. Screening by a combination of fetal nuchal translucency and maternal serum free human chorionic gonadotropin and pregnancy-associated plasma protein-A can identify 90% of fetuses with trisomy 21 and other major chromosomal abnormalities for a false-positive rate of 5%. This is superior to the 30% detection rate achieved by maternal age and 65% by second-trimester maternal serum biochemistry. A further improvement in the effectiveness of first-trimester screening is likely to be achieved by a risk-orientated two-stage approach. In this approach, the patients are subdivided into a high-risk group, requiring invasive testing; a low-risk group, which can be reassured that an abnormality is unlikely, and an intermediate-risk group (risk of 1 in 101 to 1 in 1000), in which further assessment is performed by first-trimester ultrasound examination (for presence/absence of the nasal bone or presence/absence of tricuspid regurgitation or normal/abnormal Doppler velocity waveform in the ductus venosus), and chorionic villus sampling is performed if their adjusted risk becomes 1 in 100 or more. Those performing first-trimester scans should be appropriately trained and their results subjected to external quality assurance. This process was well established by the Fetal Medical Foundation several years ago and is widely accepted internationally.
Summary
Rev Bras Ginecol Obstet. 2007;29(12):647-653
DOI 10.1590/S0100-72032007001200008
Screening for major chromosomal abnormalities can be provided in the first trimester of pregnancy. Screening by a combination of fetal nuchal translucency and maternal serum free human chorionic gonadotropin and pregnancy-associated plasma protein-A can identify 90% of fetuses with trisomy 21 and other major chromosomal abnormalities for a false-positive rate of 5%. This is superior to the 30% detection rate achieved by maternal age and 65% by second-trimester maternal serum biochemistry. A further improvement in the effectiveness of first-trimester screening is likely to be achieved by a risk-orientated two-stage approach. In this approach, the patients are subdivided into a high-risk group, requiring invasive testing; a low-risk group, which can be reassured that an abnormality is unlikely, and an intermediate-risk group (risk of 1 in 101 to 1 in 1000), in which further assessment is performed by first-trimester ultrasound examination (for presence/absence of the nasal bone or presence/absence of tricuspid regurgitation or normal/abnormal Doppler velocity waveform in the ductus venosus), and chorionic villus sampling is performed if their adjusted risk becomes 1 in 100 or more. Those performing first-trimester scans should be appropriately trained and their results subjected to external quality assurance. This process was well established by the Fetal Medical Foundation several years ago and is widely accepted internationally.

Summary
Rev Bras Ginecol Obstet. 2005;27(11):698-705
DOI 10.1590/S0100-72032005001100011
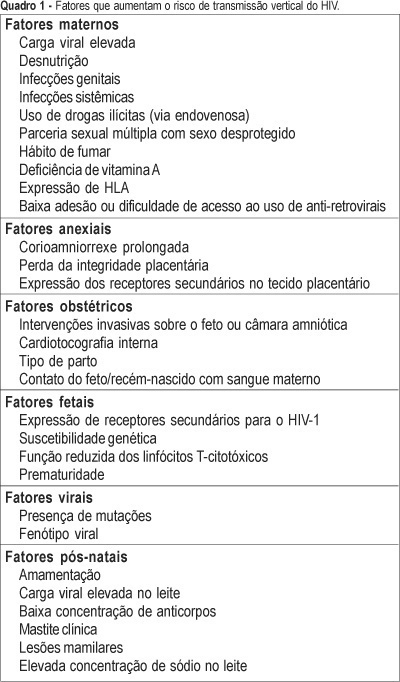
One of the most important advances in the control of the spread of infection with type 1 human immunodeficiency virus (HIV-1) occurred within the context of vertical transmission (VT), with a reduction from levels of more than 40% to levels of less than 3%. Technological progress together with a better physiopathological understanding of this infection has permitted the determination of the situations and factors that increase the rates of perinatal transmission of the virus, indicating which interventions are most adequate for its control. The situations of higher risk for VT of HIV involve maternal, adnexal, obstetrical, fetal, viral, and postnatal factors. Among maternal factors, particularly important is viral load, the major indicator of the risk of this form of transmission. However, despite its relevance, viral load is not the only variable in this equation, with the following factors also playing important roles: use of illicit drugs, multiple sex partners and unprotected sex, malnutrition, smoking habit, advanced maternal disease, and lack af access or compliance with antiretroviral drugs. Among the adnexal factors are prolonged chorion-amniorrhexis, loss of placental integrity, and the expression of secondary receptors in placental tissue. Among the obstetrical factors, it should be remembered that invasive interventions in the fetus or amniotic chamber, internal cardiotocography, type of delivery, and contact of the fetus/newborn infant with maternal blood are also important elements to be controlled. Among the fetal factors are the expression of secondary HIV-1 receptors, genetic susceptibility, reduced cytotoxic T-lymphocyte function, and prematurity. Among the viral factors, mutations and syncytium-inducing strains are believed to be risk factors for VT. Finally, there are postnatal factors represented by an elevated viral load in maternal milk, a low antibody concentration in this fluid, clinical mastitis and nipple lesions, which can be grouped within the context of breast-feeding.
Summary
Rev Bras Ginecol Obstet. 2005;27(11):698-705
DOI 10.1590/S0100-72032005001100011
One of the most important advances in the control of the spread of infection with type 1 human immunodeficiency virus (HIV-1) occurred within the context of vertical transmission (VT), with a reduction from levels of more than 40% to levels of less than 3%. Technological progress together with a better physiopathological understanding of this infection has permitted the determination of the situations and factors that increase the rates of perinatal transmission of the virus, indicating which interventions are most adequate for its control. The situations of higher risk for VT of HIV involve maternal, adnexal, obstetrical, fetal, viral, and postnatal factors. Among maternal factors, particularly important is viral load, the major indicator of the risk of this form of transmission. However, despite its relevance, viral load is not the only variable in this equation, with the following factors also playing important roles: use of illicit drugs, multiple sex partners and unprotected sex, malnutrition, smoking habit, advanced maternal disease, and lack af access or compliance with antiretroviral drugs. Among the adnexal factors are prolonged chorion-amniorrhexis, loss of placental integrity, and the expression of secondary receptors in placental tissue. Among the obstetrical factors, it should be remembered that invasive interventions in the fetus or amniotic chamber, internal cardiotocography, type of delivery, and contact of the fetus/newborn infant with maternal blood are also important elements to be controlled. Among the fetal factors are the expression of secondary HIV-1 receptors, genetic susceptibility, reduced cytotoxic T-lymphocyte function, and prematurity. Among the viral factors, mutations and syncytium-inducing strains are believed to be risk factors for VT. Finally, there are postnatal factors represented by an elevated viral load in maternal milk, a low antibody concentration in this fluid, clinical mastitis and nipple lesions, which can be grouped within the context of breast-feeding.