Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):697-704
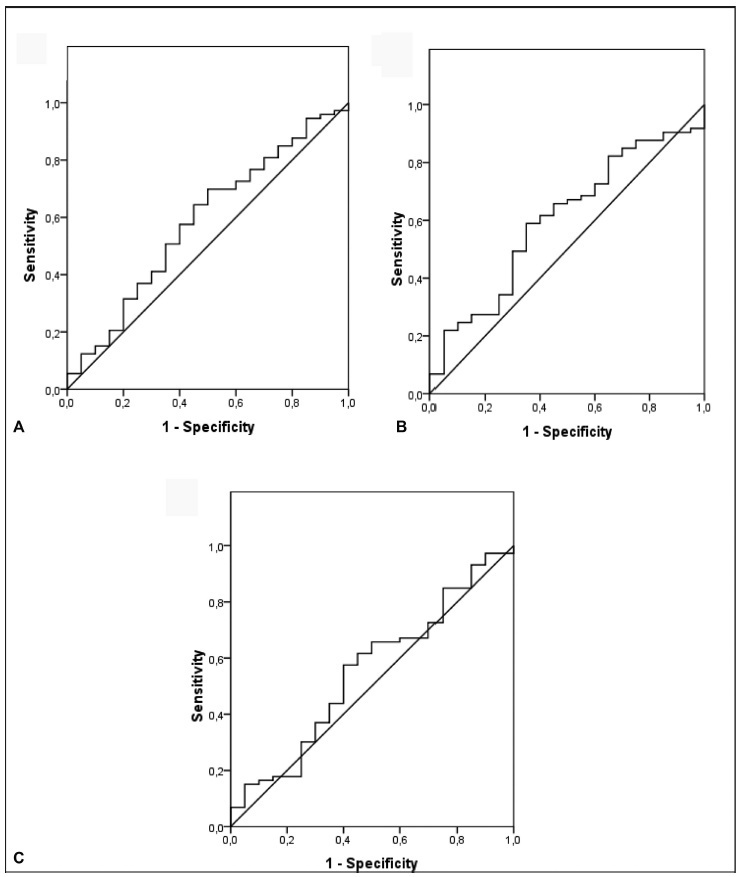
Recent observations support the hypothesis that an imbalance between angiogenic factors has a fundamental role in the pathogenesis of pre-eclampsia and is responsible for the clinical manifestations of the disease. The goal of the present study was to evaluate the sensitivity, specificity, and the best accuracy level of Soluble fms-like tyrosine kinase-1 (sFlt-1), placental growth factor (PlGF), and sFlt-1/PlGF ratio in maternal serum and protein/creatinine ratio in urine sample to define the best cutoff point of these tests to discriminate between the patients with gestational hypertension and the patients with pre-eclampsia, to evaluate the possibility of using them as diagnostic methods.
A prospective longitudinal study was performed, and blood samples were collected from 95 pregnant patients with hypertension to measure serum concentrations of biomarkers sFlt-1 and PlGF. Urine samples were collected for protein screening. Significance was set as p < 0.05.
The sFlt-1/PlGF ratio demonstrated a sensitivity of 57.5% and a specificity of 60% using 50.4 as a cutoff point. The test that showed the best accuracy in the diagnosis of pre-eclampsia was protein/creatinine ratio, with a sensitivity of 78.9% and a specificity of 70% using 0.4 as a cutoff point and showing an area under the receiver operating characteristic curve of 0.80 (p < 0.001).
No studied laboratory test proved to be fairly accurate for the diagnosis of pre-eclampsia, except for the protein/creatinine ratio. The evidence is insufficient to recommend biomarkers sFlt-1 and PlGF to be used for the diagnosis of pre-eclampsia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(11):697-704
Recent observations support the hypothesis that an imbalance between angiogenic factors has a fundamental role in the pathogenesis of pre-eclampsia and is responsible for the clinical manifestations of the disease. The goal of the present study was to evaluate the sensitivity, specificity, and the best accuracy level of Soluble fms-like tyrosine kinase-1 (sFlt-1), placental growth factor (PlGF), and sFlt-1/PlGF ratio in maternal serum and protein/creatinine ratio in urine sample to define the best cutoff point of these tests to discriminate between the patients with gestational hypertension and the patients with pre-eclampsia, to evaluate the possibility of using them as diagnostic methods.
A prospective longitudinal study was performed, and blood samples were collected from 95 pregnant patients with hypertension to measure serum concentrations of biomarkers sFlt-1 and PlGF. Urine samples were collected for protein screening. Significance was set as p < 0.05.
The sFlt-1/PlGF ratio demonstrated a sensitivity of 57.5% and a specificity of 60% using 50.4 as a cutoff point. The test that showed the best accuracy in the diagnosis of pre-eclampsia was protein/creatinine ratio, with a sensitivity of 78.9% and a specificity of 70% using 0.4 as a cutoff point and showing an area under the receiver operating characteristic curve of 0.80 (p < 0.001).
No studied laboratory test proved to be fairly accurate for the diagnosis of pre-eclampsia, except for the protein/creatinine ratio. The evidence is insufficient to recommend biomarkers sFlt-1 and PlGF to be used for the diagnosis of pre-eclampsia.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(12):697-702
To evaluate the factors associated with the need for insulin as a complementary treatment to metformin in pregnant women with gestational diabetes mellitus (GDM).
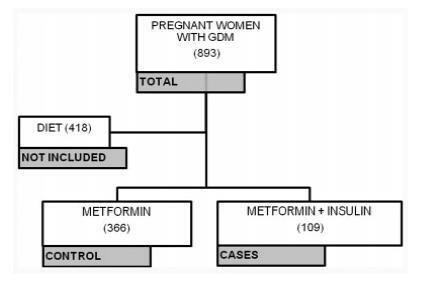
A case-control study was performed from April 2011 to February 2016 with pregnant women with GDM who needed complementary treatments besides diet and physical exercise. Those treated with metformin were compared with those who, in addition to metformin, also needed the combination with insulin. Maternal characteristics and glycemic control were evaluated. Multinomial logistic regression models were developed to evaluate the influence of different therapies on neonatal outcomes.
A total of 475 pregnant women who needed pharmacological therapy were evaluated. Of these, 366 (77.05%) were submitted to single therapy with metformin, and 109 (22.94%) needed insulin as a complementary treatment. In the analysis of the odds ratio (OR), fasting glucose (FG)<90 mg/dL reduced the odds of needing the combination (OR: 0.438 [0.235-0.815]; p=0.009], as well as primiparity (OR: 0.280 [0.111-0.704]; p=0.007]. In obese pregnant women, an increased chance of needing the combination was observed (OR: 2,072 [1,063-4,039]; p=0,032).
Obesity resulted in an increased chance of the mother needing insulin as a complementary treatment to metformin, while FG<90 mg/dL and primiparity were protective factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(12):697-702
To evaluate the factors associated with the need for insulin as a complementary treatment to metformin in pregnant women with gestational diabetes mellitus (GDM).
A case-control study was performed from April 2011 to February 2016 with pregnant women with GDM who needed complementary treatments besides diet and physical exercise. Those treated with metformin were compared with those who, in addition to metformin, also needed the combination with insulin. Maternal characteristics and glycemic control were evaluated. Multinomial logistic regression models were developed to evaluate the influence of different therapies on neonatal outcomes.
A total of 475 pregnant women who needed pharmacological therapy were evaluated. Of these, 366 (77.05%) were submitted to single therapy with metformin, and 109 (22.94%) needed insulin as a complementary treatment. In the analysis of the odds ratio (OR), fasting glucose (FG)<90 mg/dL reduced the odds of needing the combination (OR: 0.438 [0.235-0.815]; p=0.009], as well as primiparity (OR: 0.280 [0.111-0.704]; p=0.007]. In obese pregnant women, an increased chance of needing the combination was observed (OR: 2,072 [1,063-4,039]; p=0,032).
Obesity resulted in an increased chance of the mother needing insulin as a complementary treatment to metformin, while FG<90 mg/dL and primiparity were protective factors.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(9):697-701
DOI 10.1590/S0100-72032004000900004
PURPOSE: to evaluate perinatal results in pregnant women over 35 years old and to check differences between two groups: 35 to 39-year-old women and women older than 40. METHODS: a retrospective survey was made during the period between January/2000 and July/2003, through the analysis of obstetric charts of 3,093 pregnant women who delivered in the "Hospital do Servidor Público Estadual - Francisco Morato de Oliveira", excluding 933 patients. The patients were divided into 3 groups: 18 to 29 years old (control group), 35 to 39 years old, and over 40 years old. Data collection was done with standardized forms, and the data were transferred to an electronic spreadsheet (Excel - Microsoft Office 2000). Statistical analysis was performed using the chi2 test and the Fisher test. The alpha risk was less or equal to 5% and the confidence interval 95%. RESULTS: cesarean section was the most used method not only in the 35 to 39-year-old group (438/792; 55.3%) but also in the group of women over 40 (153/236; 64.8%). The rates of prematurity (39/236; 16.5%), low weight (37/236; 15.7%), and restriction of fetal growth (38/236; 16.1%) were significantly higher in the group of women over 40, when compared to the other groups. Concerning fetal death, a five times higher incidence was observed in the group over 40 years old, as compared to the other groups, a statistically significant difference. CONCLUSION: the only difference between the 35 to 39-year-old group and the control group was the cesarean section rate. This allows us to suggest a differentiated prenatal attendance for pregnant women over 40.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(9):697-701
DOI 10.1590/S0100-72032004000900004
PURPOSE: to evaluate perinatal results in pregnant women over 35 years old and to check differences between two groups: 35 to 39-year-old women and women older than 40. METHODS: a retrospective survey was made during the period between January/2000 and July/2003, through the analysis of obstetric charts of 3,093 pregnant women who delivered in the "Hospital do Servidor Público Estadual - Francisco Morato de Oliveira", excluding 933 patients. The patients were divided into 3 groups: 18 to 29 years old (control group), 35 to 39 years old, and over 40 years old. Data collection was done with standardized forms, and the data were transferred to an electronic spreadsheet (Excel - Microsoft Office 2000). Statistical analysis was performed using the chi2 test and the Fisher test. The alpha risk was less or equal to 5% and the confidence interval 95%. RESULTS: cesarean section was the most used method not only in the 35 to 39-year-old group (438/792; 55.3%) but also in the group of women over 40 (153/236; 64.8%). The rates of prematurity (39/236; 16.5%), low weight (37/236; 15.7%), and restriction of fetal growth (38/236; 16.1%) were significantly higher in the group of women over 40, when compared to the other groups. Concerning fetal death, a five times higher incidence was observed in the group over 40 years old, as compared to the other groups, a statistically significant difference. CONCLUSION: the only difference between the 35 to 39-year-old group and the control group was the cesarean section rate. This allows us to suggest a differentiated prenatal attendance for pregnant women over 40.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(11):698-705
DOI 10.1590/S0100-72032005001100011
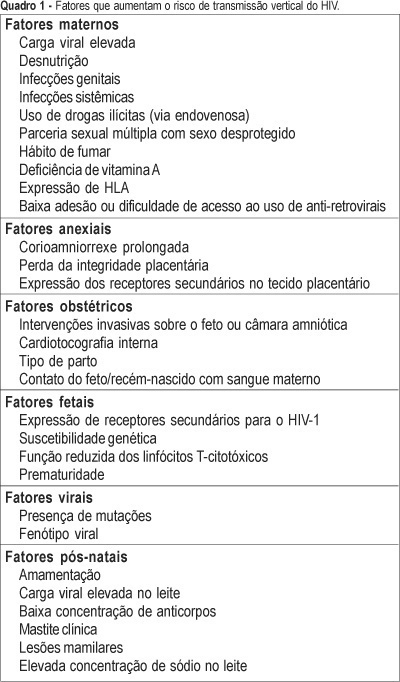
One of the most important advances in the control of the spread of infection with type 1 human immunodeficiency virus (HIV-1) occurred within the context of vertical transmission (VT), with a reduction from levels of more than 40% to levels of less than 3%. Technological progress together with a better physiopathological understanding of this infection has permitted the determination of the situations and factors that increase the rates of perinatal transmission of the virus, indicating which interventions are most adequate for its control. The situations of higher risk for VT of HIV involve maternal, adnexal, obstetrical, fetal, viral, and postnatal factors. Among maternal factors, particularly important is viral load, the major indicator of the risk of this form of transmission. However, despite its relevance, viral load is not the only variable in this equation, with the following factors also playing important roles: use of illicit drugs, multiple sex partners and unprotected sex, malnutrition, smoking habit, advanced maternal disease, and lack af access or compliance with antiretroviral drugs. Among the adnexal factors are prolonged chorion-amniorrhexis, loss of placental integrity, and the expression of secondary receptors in placental tissue. Among the obstetrical factors, it should be remembered that invasive interventions in the fetus or amniotic chamber, internal cardiotocography, type of delivery, and contact of the fetus/newborn infant with maternal blood are also important elements to be controlled. Among the fetal factors are the expression of secondary HIV-1 receptors, genetic susceptibility, reduced cytotoxic T-lymphocyte function, and prematurity. Among the viral factors, mutations and syncytium-inducing strains are believed to be risk factors for VT. Finally, there are postnatal factors represented by an elevated viral load in maternal milk, a low antibody concentration in this fluid, clinical mastitis and nipple lesions, which can be grouped within the context of breast-feeding.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(11):698-705
DOI 10.1590/S0100-72032005001100011
One of the most important advances in the control of the spread of infection with type 1 human immunodeficiency virus (HIV-1) occurred within the context of vertical transmission (VT), with a reduction from levels of more than 40% to levels of less than 3%. Technological progress together with a better physiopathological understanding of this infection has permitted the determination of the situations and factors that increase the rates of perinatal transmission of the virus, indicating which interventions are most adequate for its control. The situations of higher risk for VT of HIV involve maternal, adnexal, obstetrical, fetal, viral, and postnatal factors. Among maternal factors, particularly important is viral load, the major indicator of the risk of this form of transmission. However, despite its relevance, viral load is not the only variable in this equation, with the following factors also playing important roles: use of illicit drugs, multiple sex partners and unprotected sex, malnutrition, smoking habit, advanced maternal disease, and lack af access or compliance with antiretroviral drugs. Among the adnexal factors are prolonged chorion-amniorrhexis, loss of placental integrity, and the expression of secondary receptors in placental tissue. Among the obstetrical factors, it should be remembered that invasive interventions in the fetus or amniotic chamber, internal cardiotocography, type of delivery, and contact of the fetus/newborn infant with maternal blood are also important elements to be controlled. Among the fetal factors are the expression of secondary HIV-1 receptors, genetic susceptibility, reduced cytotoxic T-lymphocyte function, and prematurity. Among the viral factors, mutations and syncytium-inducing strains are believed to be risk factors for VT. Finally, there are postnatal factors represented by an elevated viral load in maternal milk, a low antibody concentration in this fluid, clinical mastitis and nipple lesions, which can be grouped within the context of breast-feeding.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(9):699-709
To evaluate the effects of vitamin D supplementation in the postpartum period of women with previous gestational diabetes mellitus (GDM).
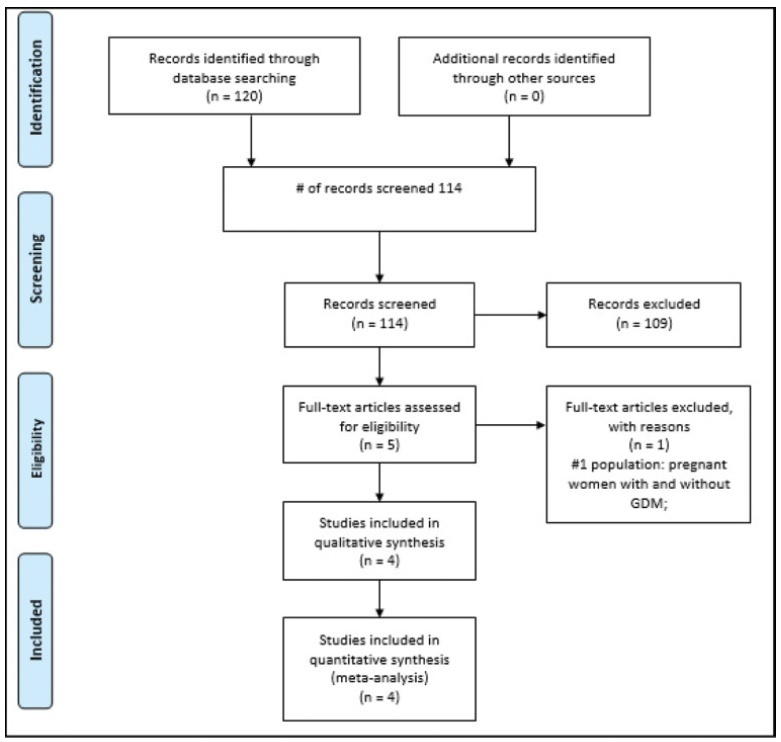
Randomized clinical trials of pregnant women with GDM of any chronological, gestational age and parity, with no history of previous disease who received vitamin D supplementation in the prenatal and/or postpartum period and were evaluated in the postpartum period were included. The PubMed, EMBASE, Cochrane, and LILACS databases were consulted until July 2019. Serum vitamin D concentration (25- hydroxyvitamin D in nmol/L), fasting blood glucose, glycated hemoglobin, serum calcium concentration, homeostatic model assessment of insulin resistance (HOMAIR), quantitative insulin sensitivity check index (QUICKI), parathyroid hormone (PTH) and body mass index (BMI) were evaluated. Similar results in at least two trials were plotted using the RevMan 5; Cochrane Collaboration, Oxford, Reino Unido. The quality of the evidence was generated according to the classification, development, and evaluation of the classification of the recommendations.
Four studies were included in the present review (200 women). The findings indicate that there is no difference in the postpartum period in women diagnosed with previous GDM who received vitamin D supplementation in the prenatal and/or in the postpartum period, showing only that there was a significant increase in the concentration of vitamin D (relative risk [RR]: 1.85; 95% confidence interval [CI]: 1.02-2.68).
This increase in the concentration of vitamin D should be interpreted with caution, since the assessment of the quality of the evidence was very low. For the other analyzed outcomes, there was no significance between the intervention and control groups, and the outcomes, when analyzed in their strength of evidence, were considered very low and low in their evaluation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(9):699-709
To evaluate the effects of vitamin D supplementation in the postpartum period of women with previous gestational diabetes mellitus (GDM).
Randomized clinical trials of pregnant women with GDM of any chronological, gestational age and parity, with no history of previous disease who received vitamin D supplementation in the prenatal and/or postpartum period and were evaluated in the postpartum period were included. The PubMed, EMBASE, Cochrane, and LILACS databases were consulted until July 2019. Serum vitamin D concentration (25- hydroxyvitamin D in nmol/L), fasting blood glucose, glycated hemoglobin, serum calcium concentration, homeostatic model assessment of insulin resistance (HOMAIR), quantitative insulin sensitivity check index (QUICKI), parathyroid hormone (PTH) and body mass index (BMI) were evaluated. Similar results in at least two trials were plotted using the RevMan 5; Cochrane Collaboration, Oxford, Reino Unido. The quality of the evidence was generated according to the classification, development, and evaluation of the classification of the recommendations.
Four studies were included in the present review (200 women). The findings indicate that there is no difference in the postpartum period in women diagnosed with previous GDM who received vitamin D supplementation in the prenatal and/or in the postpartum period, showing only that there was a significant increase in the concentration of vitamin D (relative risk [RR]: 1.85; 95% confidence interval [CI]: 1.02-2.68).
This increase in the concentration of vitamin D should be interpreted with caution, since the assessment of the quality of the evidence was very low. For the other analyzed outcomes, there was no significance between the intervention and control groups, and the outcomes, when analyzed in their strength of evidence, were considered very low and low in their evaluation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):699-704
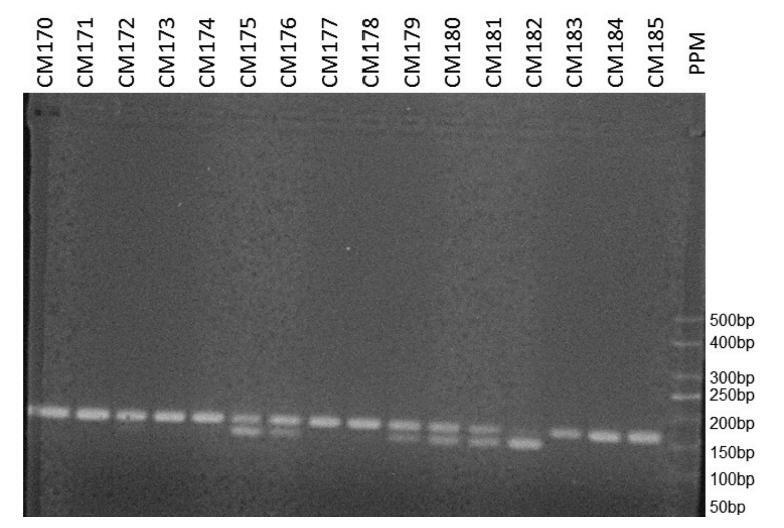
Epidemiological studies have shown evidence of the effect of sex hormones in the pathogenesis of breast cancer, and have suggested a relationship of the disease with variations in genes involved in estrogen synthesis and/or metabolism. The aim of the present study was to evaluate the association between the CYP3A4*1B gene polymorphism (rs2740574) and the risk of developing breast cancer.
In the present case-control study, the frequency of the CYP3A4*1B gene polymorphism was determined in 148 women with breast cancer and in 245 women without the disease. The DNA of the participants was extracted from plasma samples, and the gene was amplified by polymerase chain reaction. The presence of the polymorphism was determined using restriction enzymes.
After adjusting for confounding variables, we have found that the polymorphism was not associated with the occurrence of breast cancer (odds ratio = 1.151; 95% confidence interval: 0.714–1.856; p= 0.564). We have also found no association with the presence of hormone receptors, with human epidermal growth factor receptor 2 (HER2) overexpression, or with the rate of tumor cell proliferation.
We have not observed a relationship between the CYP3A4*1B gene polymorphism and the occurrence of breast cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):699-704
Epidemiological studies have shown evidence of the effect of sex hormones in the pathogenesis of breast cancer, and have suggested a relationship of the disease with variations in genes involved in estrogen synthesis and/or metabolism. The aim of the present study was to evaluate the association between the CYP3A4*1B gene polymorphism (rs2740574) and the risk of developing breast cancer.
In the present case-control study, the frequency of the CYP3A4*1B gene polymorphism was determined in 148 women with breast cancer and in 245 women without the disease. The DNA of the participants was extracted from plasma samples, and the gene was amplified by polymerase chain reaction. The presence of the polymorphism was determined using restriction enzymes.
After adjusting for confounding variables, we have found that the polymorphism was not associated with the occurrence of breast cancer (odds ratio = 1.151; 95% confidence interval: 0.714–1.856; p= 0.564). We have also found no association with the presence of hormone receptors, with human epidermal growth factor receptor 2 (HER2) overexpression, or with the rate of tumor cell proliferation.
We have not observed a relationship between the CYP3A4*1B gene polymorphism and the occurrence of breast cancer.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(11):699-705
To evaluate the effectiveness of an educational intervention among gynecologists about recommendations of the Total Acceleration of Postoperative Recovery (ACERTO, in the Portuguese acronym) project derived from the solid foundations of Enhanced Recovery After Surgery (ERAS) guidelines to optimize hospital care for surgical-gynecological patients.
Educational intervention through monthly 1-hour long meetings (3 months), with the application of an objective questionnaire about specific knowledge of the ACERTO project between before and after educational intervention phases, for gynecologists, after approval by the ethics committee and signature of informed consent by participants, in a federal university hospital.
Among the 25 gynecologists who agreed to participate, the educational intervention could be effective with a statistically significant difference between the phases before and after the intervention for the main recommendations of the ACERTO project, such as abbreviation of preoperative fasting (p = 0.006), venous thromboembolism prophylaxis (p = 0.024), knowledge and replication of ACERTO (p = 0.034), and multimodal analgesia (p = 0.021).
An educational intervention, through clinical meetings with exposition and discussion of the recommendations of the ACERTO project based on the ERAS protocol can be effective for the knowledge and possibility of practical application of the main measures, such as abbreviation of preoperative fasting, multimodal analgesia, and prophylaxis of thrombosis among gynecologists.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(11):699-705
To evaluate the effectiveness of an educational intervention among gynecologists about recommendations of the Total Acceleration of Postoperative Recovery (ACERTO, in the Portuguese acronym) project derived from the solid foundations of Enhanced Recovery After Surgery (ERAS) guidelines to optimize hospital care for surgical-gynecological patients.
Educational intervention through monthly 1-hour long meetings (3 months), with the application of an objective questionnaire about specific knowledge of the ACERTO project between before and after educational intervention phases, for gynecologists, after approval by the ethics committee and signature of informed consent by participants, in a federal university hospital.
Among the 25 gynecologists who agreed to participate, the educational intervention could be effective with a statistically significant difference between the phases before and after the intervention for the main recommendations of the ACERTO project, such as abbreviation of preoperative fasting (p = 0.006), venous thromboembolism prophylaxis (p = 0.024), knowledge and replication of ACERTO (p = 0.034), and multimodal analgesia (p = 0.021).
An educational intervention, through clinical meetings with exposition and discussion of the recommendations of the ACERTO project based on the ERAS protocol can be effective for the knowledge and possibility of practical application of the main measures, such as abbreviation of preoperative fasting, multimodal analgesia, and prophylaxis of thrombosis among gynecologists.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):7-11
DOI 10.1590/S0100-72032005000100003
PURPOSE: to compare pregnancy rates and mean endometrial thickness obtained with three protocols for induction of ovulation in cycles of intrauterine insemination (IUI). METHODS: one hundred and ten IUI cycles were retrospectively evaluated in the study, divided into three groups, according to the used ovulation induction protocols: 100 mg clomiphene citrate (CC) on days 3 to 7 of the cycle (CC group, n=24), 100 mg/day CC on days 3 to 7 of the cycle + 75 IU/day of human menopausal gonadotrophin (hMG) on days 3, 5 and 7 of the cycle (CC+hMG group, n=29), and 75 IU/day of hMG on days 3 to 8 of the cycle (hMG group, n=57). Statistical analysis was performed using Student's t test to compare the means and the c² test to compare the rates. Results were considered statistically significant at p<0.05. RESULTS: the patients' average age at the onset of the first cycle was 2340 years (mean age, 33.3 years). There were no statistically significant differences between groups. The mean endometrial thickness on the day of the human chorionic gonadotrophin (hCG) administration was significantly higher in the hMG group (10.2±0.2 mm), as compared with the CC and CC+hMG group (7.9±0.4 and 8.7±0.2 mm, respectively, p<0.001). The overall clinical pregnancy rate was 18.2%, and there were no statistically significant differences between the groups (CC group=12.5%; CC+hMG group=24.1% and hMG group=19.3%). CONCLUSION: the results indicate higher mean endometrial thickness in the hMG group as compared with the CC group and the CC+hMG group. There were no significant differences between clinical pregnancy rates obtained with each protocol (CC, CC+hMG and hMG).
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):7-11
DOI 10.1590/S0100-72032005000100003
PURPOSE: to compare pregnancy rates and mean endometrial thickness obtained with three protocols for induction of ovulation in cycles of intrauterine insemination (IUI). METHODS: one hundred and ten IUI cycles were retrospectively evaluated in the study, divided into three groups, according to the used ovulation induction protocols: 100 mg clomiphene citrate (CC) on days 3 to 7 of the cycle (CC group, n=24), 100 mg/day CC on days 3 to 7 of the cycle + 75 IU/day of human menopausal gonadotrophin (hMG) on days 3, 5 and 7 of the cycle (CC+hMG group, n=29), and 75 IU/day of hMG on days 3 to 8 of the cycle (hMG group, n=57). Statistical analysis was performed using Student's t test to compare the means and the c² test to compare the rates. Results were considered statistically significant at p<0.05. RESULTS: the patients' average age at the onset of the first cycle was 2340 years (mean age, 33.3 years). There were no statistically significant differences between groups. The mean endometrial thickness on the day of the human chorionic gonadotrophin (hCG) administration was significantly higher in the hMG group (10.2±0.2 mm), as compared with the CC and CC+hMG group (7.9±0.4 and 8.7±0.2 mm, respectively, p<0.001). The overall clinical pregnancy rate was 18.2%, and there were no statistically significant differences between the groups (CC group=12.5%; CC+hMG group=24.1% and hMG group=19.3%). CONCLUSION: the results indicate higher mean endometrial thickness in the hMG group as compared with the CC group and the CC+hMG group. There were no significant differences between clinical pregnancy rates obtained with each protocol (CC, CC+hMG and hMG).