Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):673-679
The aim of this study was to analyze and compare obstetric and neonatal outcomes between Syrian refugees and ethnic Turkish women.
Retrospective, observational study. A total of 576 Syrian refugees and 576 ethnic Turkish women were included in this study, which was conducted between January 2015 and December 2015 at a tertiary maternity training hospital in Ankara, Turkey. The demographic characteristics, obstetric and neonatal outcomes were compared. The primary outcomes were pregnancy outcomes and cesarean rates between the groups
The mean age was significantly lower in the refugee group (p< 0.001). Mean gravidity, proportion of adolescent pregnancies, proportion of pregnant women aged 12 to 19 years, and number of pregnancies at < 18 years were significantly higher among the refugee women (p< 0.001). Rates of antenatal follow-up, double testing, triple testing, gestational diabetes mellitus (GDM) screening, and iron replacement therapy were significantly lower in the refugee group (p< 0.001). The primary Cesarean section rate was significantly lower in the refugee group (p= 0.034). Pregnancies in the refugee group were more complicated, with higher rates of preterm delivery (< 37 weeks), preterm premature rupture of membranes (PPROM), and low birth weight (< 2,500 g) when compared with the control group (4.2% versus 0.7%, p< 0.001; 1.6% versus 0.2%, p= 0.011; and 12% versus 5.8%, p< 0.001, respectively). Low education level (odds ratio [OR] = 1.7, 95% confidence interval [CI] = 0.5–0.1), and weight gain during pregnancy (OR = 1.7, 95% CI = 0.5–0.1) were found to be significant indicators for preterm birth/PPROM and low birthweight.
Syrian refugees had increased risks of certain adverse obstetric outcomes, including preterm delivery, PPROM, lower birth weight, and anemia. Several factors may influence these findings; thus, refugee women would benefit from more targeted care during pregnancy and childbirth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(11):673-679
The aim of this study was to analyze and compare obstetric and neonatal outcomes between Syrian refugees and ethnic Turkish women.
Retrospective, observational study. A total of 576 Syrian refugees and 576 ethnic Turkish women were included in this study, which was conducted between January 2015 and December 2015 at a tertiary maternity training hospital in Ankara, Turkey. The demographic characteristics, obstetric and neonatal outcomes were compared. The primary outcomes were pregnancy outcomes and cesarean rates between the groups
The mean age was significantly lower in the refugee group (p< 0.001). Mean gravidity, proportion of adolescent pregnancies, proportion of pregnant women aged 12 to 19 years, and number of pregnancies at < 18 years were significantly higher among the refugee women (p< 0.001). Rates of antenatal follow-up, double testing, triple testing, gestational diabetes mellitus (GDM) screening, and iron replacement therapy were significantly lower in the refugee group (p< 0.001). The primary Cesarean section rate was significantly lower in the refugee group (p= 0.034). Pregnancies in the refugee group were more complicated, with higher rates of preterm delivery (< 37 weeks), preterm premature rupture of membranes (PPROM), and low birth weight (< 2,500 g) when compared with the control group (4.2% versus 0.7%, p< 0.001; 1.6% versus 0.2%, p= 0.011; and 12% versus 5.8%, p< 0.001, respectively). Low education level (odds ratio [OR] = 1.7, 95% confidence interval [CI] = 0.5–0.1), and weight gain during pregnancy (OR = 1.7, 95% CI = 0.5–0.1) were found to be significant indicators for preterm birth/PPROM and low birthweight.
Syrian refugees had increased risks of certain adverse obstetric outcomes, including preterm delivery, PPROM, lower birth weight, and anemia. Several factors may influence these findings; thus, refugee women would benefit from more targeted care during pregnancy and childbirth.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(11):673-678
To evaluate whether the use of intraoperative ultrasound leads to more conservative surgeries for benign ovarian tumors.
Women who underwent surgery between 2007 and 2017 for benign ovarian tumors were retrospectively analyzed. The women were classified into two groups: those who underwent intraoperative ultrasound (group A) and those who did not (group B). In group A, minimally-invasive surgery was performed for most patients (a specific laparoscopic ultrasound probe was used), and four patients were submitted to laparotomy (a linear ultrasound probe was used). The primary endpoint was ovarian sparing surgery (oophoroplasty).
Among the 82 cases identified, only 36 met the inclusion criteria for the present study. Out of these cases, 25 underwent intraoperative ultrasound, and 11 did not. There were no significant differences in arterial hypertension, diabetes, smoking history, and body mass index for the two groups (p=0.450). Tumor diameter was also similar for both groups, ranging from 1 cm to 11 cm in group A and from 1.3 cm to 10 cm in group B (p=0.594). Tumor histology confirmed mature teratomas for all of the cases in group B and for 68.0% of the cases in group A. When the intraoperative ultrasound was performed, a more conservative surgery was performed (p<0.001).
The use of intraoperative ultrasound resulted in more conservative surgeries for the resection of benign ovarian tumors at our center.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(11):673-678
To evaluate whether the use of intraoperative ultrasound leads to more conservative surgeries for benign ovarian tumors.
Women who underwent surgery between 2007 and 2017 for benign ovarian tumors were retrospectively analyzed. The women were classified into two groups: those who underwent intraoperative ultrasound (group A) and those who did not (group B). In group A, minimally-invasive surgery was performed for most patients (a specific laparoscopic ultrasound probe was used), and four patients were submitted to laparotomy (a linear ultrasound probe was used). The primary endpoint was ovarian sparing surgery (oophoroplasty).
Among the 82 cases identified, only 36 met the inclusion criteria for the present study. Out of these cases, 25 underwent intraoperative ultrasound, and 11 did not. There were no significant differences in arterial hypertension, diabetes, smoking history, and body mass index for the two groups (p=0.450). Tumor diameter was also similar for both groups, ranging from 1 cm to 11 cm in group A and from 1.3 cm to 10 cm in group B (p=0.594). Tumor histology confirmed mature teratomas for all of the cases in group B and for 68.0% of the cases in group A. When the intraoperative ultrasound was performed, a more conservative surgery was performed (p<0.001).
The use of intraoperative ultrasound resulted in more conservative surgeries for the resection of benign ovarian tumors at our center.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):674-674
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):674-674
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):674-674
DOI 10.1590/S0100-72032001001000010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):674-674
DOI 10.1590/S0100-72032001001000010
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(10):675-680
DOI 10.1590/S0100-72032002001000007
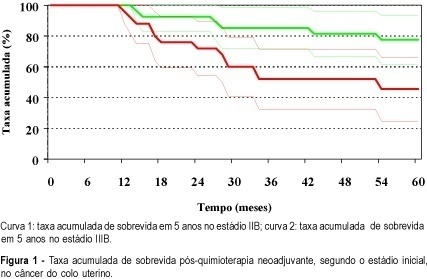
PURPOSE: to evaluate neoadjuvant chemotherapy in locally advanced cervical cancer as to its acceptability, tolerability, toxicity, surgical complications, operability, response rate, and overall survival in 5 years. METHODS: sixty women with locally advanced cervical cancer (stages IIB and IIIB), who were submitted to neoadjuvant chemotherapy, were included. All patients were treated with doxorubicin-bleomycin-cisplatin. Those who had a good response, allowing a surgical approach, underwent the Wertheim-Meigs procedure. After surgery, they were submitted to pelvic radiotherapy. Those that could not be submitted to surgery after chemotherapy underwent total radiotherapy. RESULTS: the average follow-up was 108 months, and 80% of the patients had an overall response to neoadjuvant chemotherapy. In the IIB group, the response rate was 100%, and in the IIIB group it was 60%. The operability rate after neoadjuvant chemotherapy was 65%. The overall survival in 5 years was 62%. Comparing the operated group (n=34) with the nonoperated group (n=18), the overall survival in 5 years was 82.14 and 16.67%, respectively. CONCLUSIONS: neoadjuvant chemotherapy with doxorubicin-bleomycin-cisplatin for locally advanced cervical cancer is safe, with a low rate of side effects, and allowed a high operability rate.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(10):675-680
DOI 10.1590/S0100-72032002001000007
PURPOSE: to evaluate neoadjuvant chemotherapy in locally advanced cervical cancer as to its acceptability, tolerability, toxicity, surgical complications, operability, response rate, and overall survival in 5 years. METHODS: sixty women with locally advanced cervical cancer (stages IIB and IIIB), who were submitted to neoadjuvant chemotherapy, were included. All patients were treated with doxorubicin-bleomycin-cisplatin. Those who had a good response, allowing a surgical approach, underwent the Wertheim-Meigs procedure. After surgery, they were submitted to pelvic radiotherapy. Those that could not be submitted to surgery after chemotherapy underwent total radiotherapy. RESULTS: the average follow-up was 108 months, and 80% of the patients had an overall response to neoadjuvant chemotherapy. In the IIB group, the response rate was 100%, and in the IIIB group it was 60%. The operability rate after neoadjuvant chemotherapy was 65%. The overall survival in 5 years was 62%. Comparing the operated group (n=34) with the nonoperated group (n=18), the overall survival in 5 years was 82.14 and 16.67%, respectively. CONCLUSIONS: neoadjuvant chemotherapy with doxorubicin-bleomycin-cisplatin for locally advanced cervical cancer is safe, with a low rate of side effects, and allowed a high operability rate.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):675-675
DOI 10.1590/S0100-72032001001000013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):675-675
DOI 10.1590/S0100-72032001001000013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):675-675
DOI 10.1590/S0100-72032001001000012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):675-675
DOI 10.1590/S0100-72032001001000012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):676-677
DOI 10.1590/S0100-72032001001000015
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):676-677
DOI 10.1590/S0100-72032001001000015