Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(10):620-621
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(10):620-621
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):621-628
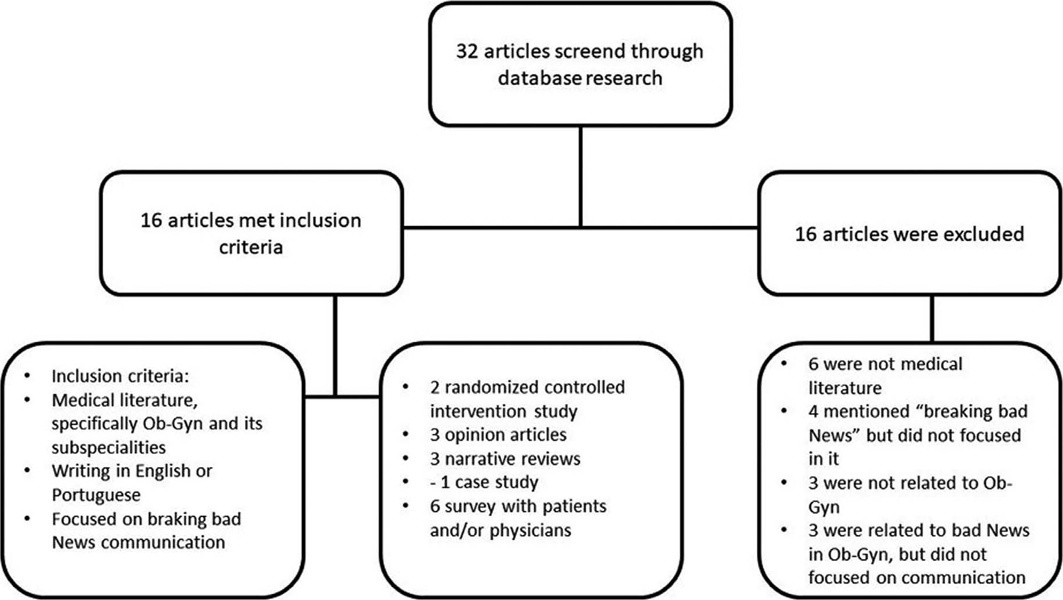
Breaking bad news is common in obstetrics and gynecology (ob-gyn). However, it is difficult, and few doctors receive training on how to deal with this situation. This narrative review aims to gather, analyze, and synthesize part of the knowledge on the area, focused on Ob-Gyn. Among the 16 selected articles, two are randomized controlled intervention studies, and most studies refer to obstetrics. The results found by us pointed out that simulation, feedback/debriefing, lectures, and protocols could improve doctors’ performance in communicating bad news. For patients, the context and how the information is transmitted seem to impact more than the content of the news. Ob-Gyn doctors could benefit from specific protocols and education, given the specialty’s particularities. There is a lack of evidence about the most effective way to conduct such training. Finding validated ways to quantify and classify studies’ results in the area, which would allow for the objective analysis of outcomes, is one of the biggest challenges concerning this topic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):621-628
Breaking bad news is common in obstetrics and gynecology (ob-gyn). However, it is difficult, and few doctors receive training on how to deal with this situation. This narrative review aims to gather, analyze, and synthesize part of the knowledge on the area, focused on Ob-Gyn. Among the 16 selected articles, two are randomized controlled intervention studies, and most studies refer to obstetrics. The results found by us pointed out that simulation, feedback/debriefing, lectures, and protocols could improve doctors’ performance in communicating bad news. For patients, the context and how the information is transmitted seem to impact more than the content of the news. Ob-Gyn doctors could benefit from specific protocols and education, given the specialty’s particularities. There is a lack of evidence about the most effective way to conduct such training. Finding validated ways to quantify and classify studies’ results in the area, which would allow for the objective analysis of outcomes, is one of the biggest challenges concerning this topic.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(10):621-629
The present study aims to determine if the use of cervical pessary plus progesterone in short-cervix (≤ 25 mm) dichorionic-diamniotic (DC-DA) twin pregnancies is equivalent to the rate of preterm births (PBs) with no intervention in unselected DC-DA twin pregnancies.
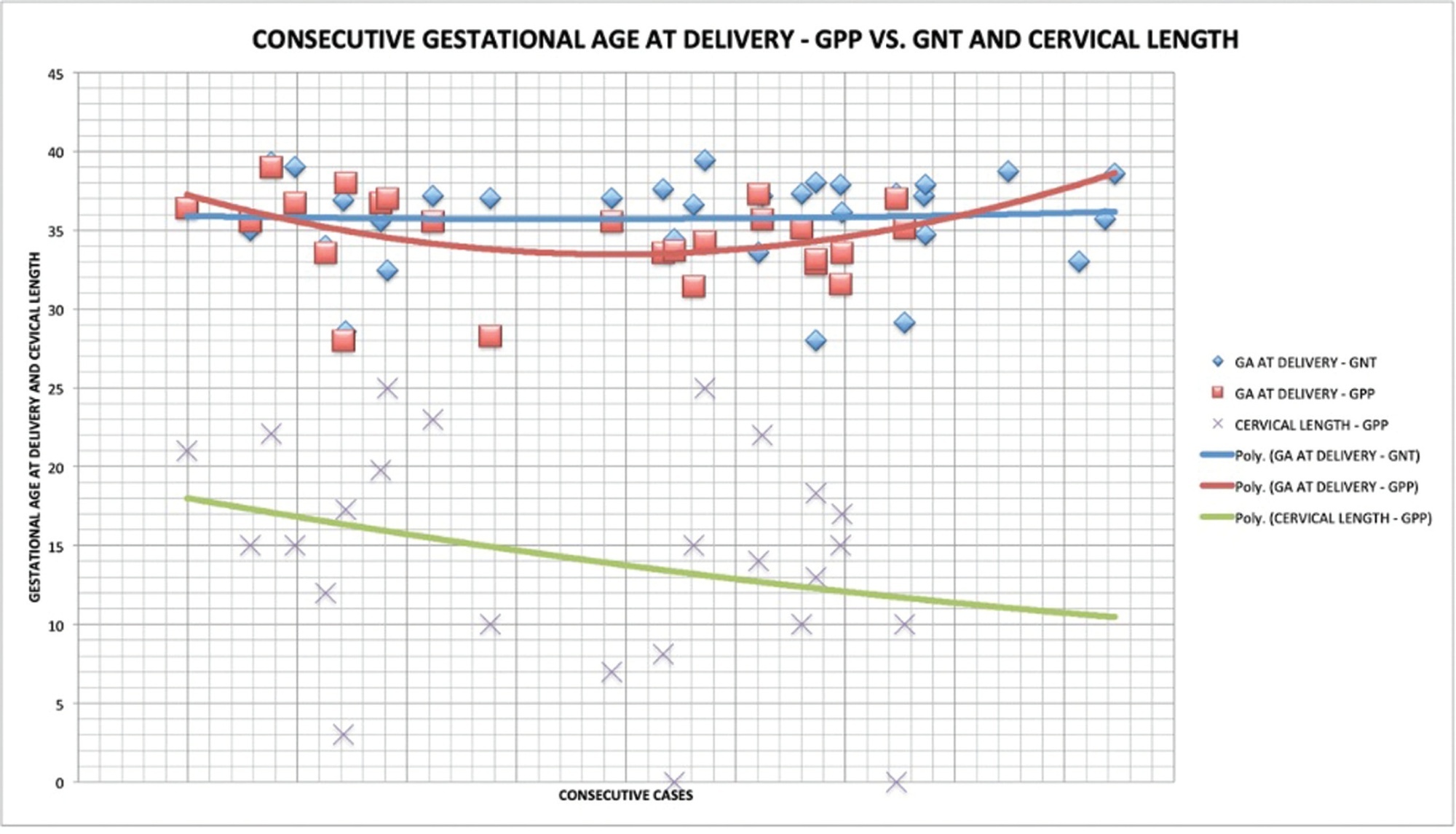
A historical cohort study was performed between 2010 and 2018, including a total of 57 pregnant women with DC-DA twin pregnancies. The women admitted from 2010 to 2012 (n = 32) received no treatment, and were not selected by cervical length (Non-Treated group, NTG), whereas those admitted from 2013 to 2018 (n = 25), were routinely submitted to cervical pessary plus progesterone after the diagnosis of short cervix from the 18th to the 27th weeks of gestation (Pessary-Progesterone group, PPG). The primary outcome analyzed was the rate of PBs before 34 weeks.
There were no statistical differences between the NTG and the PPG regarding PB < 34 weeks (18.8%; versus 40.0%; respectively; p = 0.07) and the mean birthweight of the smallest twin (2,037 ± 425 g versus 2,195 ± 665 g; p = 0.327). The Kaplan-Meyer Survival analysis was performed, and there were no differences between the groups before 31.5 weeks. Logistic regression showed that a previous PB (< 37 weeks) presented an odds ratio (OR) of 15.951 (95%; confidence interval [95%;CI]: 1.294-196.557; p = 0.031*) for PB < 34 weeks in the PPG.
In DC-DA twin pregnancies with a short cervix, (which means a higher risk of PB), the treatment with cervical pessary plus progesterone could be considered equivalent in several aspects related to PB in the NTG, despite the big difference between these groups.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(10):621-629
The present study aims to determine if the use of cervical pessary plus progesterone in short-cervix (≤ 25 mm) dichorionic-diamniotic (DC-DA) twin pregnancies is equivalent to the rate of preterm births (PBs) with no intervention in unselected DC-DA twin pregnancies.
A historical cohort study was performed between 2010 and 2018, including a total of 57 pregnant women with DC-DA twin pregnancies. The women admitted from 2010 to 2012 (n = 32) received no treatment, and were not selected by cervical length (Non-Treated group, NTG), whereas those admitted from 2013 to 2018 (n = 25), were routinely submitted to cervical pessary plus progesterone after the diagnosis of short cervix from the 18th to the 27th weeks of gestation (Pessary-Progesterone group, PPG). The primary outcome analyzed was the rate of PBs before 34 weeks.
There were no statistical differences between the NTG and the PPG regarding PB < 34 weeks (18.8%; versus 40.0%; respectively; p = 0.07) and the mean birthweight of the smallest twin (2,037 ± 425 g versus 2,195 ± 665 g; p = 0.327). The Kaplan-Meyer Survival analysis was performed, and there were no differences between the groups before 31.5 weeks. Logistic regression showed that a previous PB (< 37 weeks) presented an odds ratio (OR) of 15.951 (95%; confidence interval [95%;CI]: 1.294-196.557; p = 0.031*) for PB < 34 weeks in the PPG.
In DC-DA twin pregnancies with a short cervix, (which means a higher risk of PB), the treatment with cervical pessary plus progesterone could be considered equivalent in several aspects related to PB in the NTG, despite the big difference between these groups.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(10):621-627
Antiphospholipid antibody syndrome (APS) is a systemic, autoimmune, prothrombotic disease characterized by persistent antiphospholipid antibodies (aPLs), thrombosis, recurrent abortion, complications during pregnancy, and occasionally thrombocytopenia. The objective of the present study was to review the pathophysiology of APS and its association with female infertility. A bibliographic review of articles of the past 20 yearswas performed at the PubMed, Scielo, and Bireme databases. Antiphospholipid antibody syndrome may be associated with primary infertility, interfering with endometrial decidualization and with decreased ovarian reserve. Antiphospholipid antibodies also have direct negative effects on placentation, when they bind to the trophoblast, reducing their capacity for invasion, and proinflammatory effects, such as complement activation and neutrophil recruitment, contributing to placental insufficiency, restricted intrauterine growth, and fetal loss. In relation to thrombosis, APS results in a diffuse thrombotic diathesis, with global and diffuse dysregulation of the homeostatic balance. Knowing the pathophysiology of APS, which is closely linked to female infertility, is essential for new therapeutic approaches, specialized in immunomodulation andinflammatory signaling pathways, to provide important advances in its treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(10):621-627
Antiphospholipid antibody syndrome (APS) is a systemic, autoimmune, prothrombotic disease characterized by persistent antiphospholipid antibodies (aPLs), thrombosis, recurrent abortion, complications during pregnancy, and occasionally thrombocytopenia. The objective of the present study was to review the pathophysiology of APS and its association with female infertility. A bibliographic review of articles of the past 20 yearswas performed at the PubMed, Scielo, and Bireme databases. Antiphospholipid antibody syndrome may be associated with primary infertility, interfering with endometrial decidualization and with decreased ovarian reserve. Antiphospholipid antibodies also have direct negative effects on placentation, when they bind to the trophoblast, reducing their capacity for invasion, and proinflammatory effects, such as complement activation and neutrophil recruitment, contributing to placental insufficiency, restricted intrauterine growth, and fetal loss. In relation to thrombosis, APS results in a diffuse thrombotic diathesis, with global and diffuse dysregulation of the homeostatic balance. Knowing the pathophysiology of APS, which is closely linked to female infertility, is essential for new therapeutic approaches, specialized in immunomodulation andinflammatory signaling pathways, to provide important advances in its treatment.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(12):621-625
DOI 10.1590/S0100-72032009001200008
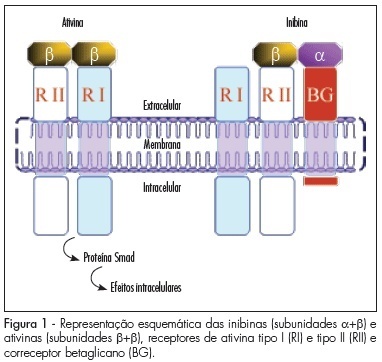
The main source of inhibin B in women is the growing follicle granulosa cells, while inhibin A is mainly produced by the corpus luteum and the placenta. In infertile women submitted to therapies of assisted reproduction, inhibin B has shown to be useful to predict a poor ovulatory response, though it has not yet overcome the performance of other markers. In the pre-natal screening of the Down syndrome, inhibin A has been repeatedly confirmed as useful in the second trimester and has also started to be considered in the first trimester test battery. Besides the two applications above, the dosage of total inhibin may contribute to the identification of cases of autoimmune ovarian insufficiency. Total inhibin may also be an auxiliary marker in the diagnosis of ovarian epithelial tumors, while the amount of inhibin B helps in the diagnosis of granulosa cells tumors. The use of inhibin A may be extended to the evaluation of pregnant women with risk of abortion, with a history of repeated abortion, with increased risk of pre-eclampsia, or even in the first days of follow-up of hydatiform mole post-emptying. All those applications are still under study, but with a real possibility of helping to extend the diagnostic spectrum of inhibin dosage in Gynecology and Obstetrics.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(12):621-625
DOI 10.1590/S0100-72032009001200008
The main source of inhibin B in women is the growing follicle granulosa cells, while inhibin A is mainly produced by the corpus luteum and the placenta. In infertile women submitted to therapies of assisted reproduction, inhibin B has shown to be useful to predict a poor ovulatory response, though it has not yet overcome the performance of other markers. In the pre-natal screening of the Down syndrome, inhibin A has been repeatedly confirmed as useful in the second trimester and has also started to be considered in the first trimester test battery. Besides the two applications above, the dosage of total inhibin may contribute to the identification of cases of autoimmune ovarian insufficiency. Total inhibin may also be an auxiliary marker in the diagnosis of ovarian epithelial tumors, while the amount of inhibin B helps in the diagnosis of granulosa cells tumors. The use of inhibin A may be extended to the evaluation of pregnant women with risk of abortion, with a history of repeated abortion, with increased risk of pre-eclampsia, or even in the first days of follow-up of hydatiform mole post-emptying. All those applications are still under study, but with a real possibility of helping to extend the diagnostic spectrum of inhibin dosage in Gynecology and Obstetrics.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):621-626
DOI 10.1590/S0100-72032001001000002
Purpose: to compare bone mineral density (BMD) of postmenopausal women with and without the antecedent of tubal ligation, as well as to evaluate the associated factors that affect the bone mineral density of femur and lumbar spine of both groups. Methods: 70 postmenopausal women in each group were analyzed at CAISM-UNICAMP, during the year of 1998. All women answered a questionnaire about some clinical and reproductive characteristics and underwent bone densitometry (Lunar DPX) to measure bone mineral density of the femur and lumbar spine. Statistical analyses were performed using Student's t-test, Fisher`s exact test, Pearson c² test, Bonferroni`s test and multiple regression analysis. Results: mean age of patients was 53.2 years and for controls it was 52.6 years. Mean age of 48 years at menopause was similar in both groups. Mean age at tubal ligation surgery was 33.7 years and time since surgery was 18 years. The multiple comparison of the average bone mineral density of femur and lumbar spine did not show statistical differences between the groups. The percentage distribution of the T-score categories of femur and lumbar spine, classified into normal and altered, also did not show statistical differences between both groups. Multiple regression analysis showed that bone mineral density of femur was directly associated with body mass index, but age was indirectly associated. The variables dark skin, parity, age at menopause, educational level and body mass index were directly associated with bone mineral density of lumbar spine, but age at menarche was inversely associated. Conclusion: these findings suggest that tubal ligation does not seem to cause an additional reduction in bone mineral density when evaluated in postmenopause.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(10):621-626
DOI 10.1590/S0100-72032001001000002
Purpose: to compare bone mineral density (BMD) of postmenopausal women with and without the antecedent of tubal ligation, as well as to evaluate the associated factors that affect the bone mineral density of femur and lumbar spine of both groups. Methods: 70 postmenopausal women in each group were analyzed at CAISM-UNICAMP, during the year of 1998. All women answered a questionnaire about some clinical and reproductive characteristics and underwent bone densitometry (Lunar DPX) to measure bone mineral density of the femur and lumbar spine. Statistical analyses were performed using Student's t-test, Fisher`s exact test, Pearson c² test, Bonferroni`s test and multiple regression analysis. Results: mean age of patients was 53.2 years and for controls it was 52.6 years. Mean age of 48 years at menopause was similar in both groups. Mean age at tubal ligation surgery was 33.7 years and time since surgery was 18 years. The multiple comparison of the average bone mineral density of femur and lumbar spine did not show statistical differences between the groups. The percentage distribution of the T-score categories of femur and lumbar spine, classified into normal and altered, also did not show statistical differences between both groups. Multiple regression analysis showed that bone mineral density of femur was directly associated with body mass index, but age was indirectly associated. The variables dark skin, parity, age at menopause, educational level and body mass index were directly associated with bone mineral density of lumbar spine, but age at menarche was inversely associated. Conclusion: these findings suggest that tubal ligation does not seem to cause an additional reduction in bone mineral density when evaluated in postmenopause.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(10):622-631
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(10):622-631
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(8):622-626
To analyze the effect of the One-minute Preceptor model for preceptors who work at the emergency department of a maternity teaching hospital.
A quantitative intervention study conducted with Obstetrics and Gynecology residency preceptors at amaternity teaching hospital in northeastern Brazil. Three stages were performed: 1) a preintervention survey with the residents; 2) planning and execution of a pedagogical training course for the preceptors, which involved a lecture and a dramatization about the One-Minute Preceptor model; and 3) thirty days after the intervention, the residents answered another survey about the model and its repercussions and advantages.
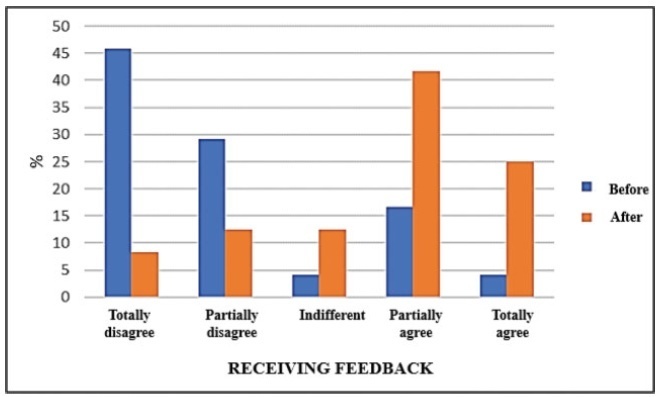
The preintervention assessment with the residents showed that 91.7% agreed that there were discrepancies regarding the teaching model among the preceptors. After the training, all preceptors agreed that the model engages the student in the decision-making process, and that they would apply it to their routine. The postintervention results showed that 95.8% agreed that themodel ismore inviting than traditional teaching approaches. There was a perception of improvement in learning among 70.9% of the residents. In addition, the present study found a significant change in feedback before and after implementing the model, from 20.8% to 66.7%.
The training course of preceptors in the One-Minute Preceptor model proved to be efficient in providing formative feedback to residents in the emergency department of a maternity school. Further studies are needed to assess the consolidation of the methodology in the long term.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(8):622-626
To analyze the effect of the One-minute Preceptor model for preceptors who work at the emergency department of a maternity teaching hospital.
A quantitative intervention study conducted with Obstetrics and Gynecology residency preceptors at amaternity teaching hospital in northeastern Brazil. Three stages were performed: 1) a preintervention survey with the residents; 2) planning and execution of a pedagogical training course for the preceptors, which involved a lecture and a dramatization about the One-Minute Preceptor model; and 3) thirty days after the intervention, the residents answered another survey about the model and its repercussions and advantages.
The preintervention assessment with the residents showed that 91.7% agreed that there were discrepancies regarding the teaching model among the preceptors. After the training, all preceptors agreed that the model engages the student in the decision-making process, and that they would apply it to their routine. The postintervention results showed that 95.8% agreed that themodel ismore inviting than traditional teaching approaches. There was a perception of improvement in learning among 70.9% of the residents. In addition, the present study found a significant change in feedback before and after implementing the model, from 20.8% to 66.7%.
The training course of preceptors in the One-Minute Preceptor model proved to be efficient in providing formative feedback to residents in the emergency department of a maternity school. Further studies are needed to assess the consolidation of the methodology in the long term.