You searched for:"Manoel João Batista Castello Girão"
We found (31) results for your search.Summary
Rev Bras Ginecol Obstet. 2018;40(8):477-490
To compare surgical treatments for stress urinary incontinence in terms of efficiency and complications.
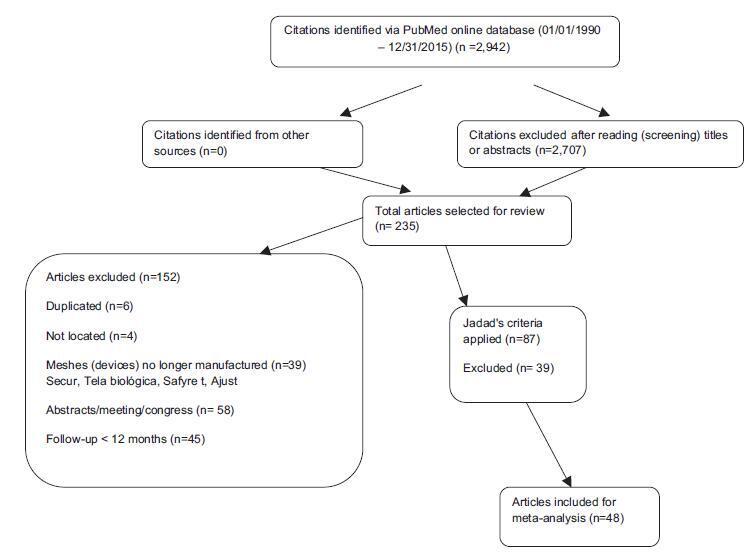
We searched the MEDLINE and COCHRANE databases using the terms stress urinary incontinence, surgical treatment for stress urinary incontinence and sling. Selection of Studies Forty-eight studies were selected, which amounted to a total of 6,881 patients with scores equal to or higher than 3 in the Jadad scale.
Each study was read by one of the authors, added to a standardized table and checked by a second author. We extracted data on intervention details, follow-up time, the results of treatment and adverse events.
Comparing retropubic versus transobturator slings, the former was superior for both objective (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.05-1.54) and subjective (OR, 1.23; 95% CI, 1.02-1.48) cures. Between minislings versus other slings, there was a difference favoring other slings for subjective cure (OR, 0.58; 95% CI, 0.39- 0.86). Between pubovaginal sling versus Burch surgery, there was a difference for both objective (OR, 2.04; 95% CI, 1.50-2.77) and subjective (OR, 1.64; 95% CI, 1.10-2.44) cures, favoring pubovaginal sling. Therewas no difference in the groups: midurethral slings versus Burch, pubovaginal sling versus midurethral slings, transobturator slings, minislings versus other slings (objective cure). Retropubic and pubovaginal slings are more retentionist. Retropubic slings have more bladder perforation, and transobturator slings, more leg and groin pain, neurological lesion and vaginal perforation.
Pubovaginal slings are superior to Burch colposuspension surgery but exhibit more retention. Retropubic slings are superior to transobturator slings, with more adverse events. Other slings are superior to minislings in the subjective aspect. There was no difference in the comparisons between midurethral slings versus Burch colposuspension surgery, pubovaginal versus midurethral slings, and inside-out versus outside-in transobturator slings.
Summary
Rev Bras Ginecol Obstet. 2018;40(8):477-490
To compare surgical treatments for stress urinary incontinence in terms of efficiency and complications.
We searched the MEDLINE and COCHRANE databases using the terms stress urinary incontinence, surgical treatment for stress urinary incontinence and sling. Selection of Studies Forty-eight studies were selected, which amounted to a total of 6,881 patients with scores equal to or higher than 3 in the Jadad scale.
Each study was read by one of the authors, added to a standardized table and checked by a second author. We extracted data on intervention details, follow-up time, the results of treatment and adverse events.
Comparing retropubic versus transobturator slings, the former was superior for both objective (odds ratio [OR], 1.27; 95% confidence interval [CI], 1.05-1.54) and subjective (OR, 1.23; 95% CI, 1.02-1.48) cures. Between minislings versus other slings, there was a difference favoring other slings for subjective cure (OR, 0.58; 95% CI, 0.39- 0.86). Between pubovaginal sling versus Burch surgery, there was a difference for both objective (OR, 2.04; 95% CI, 1.50-2.77) and subjective (OR, 1.64; 95% CI, 1.10-2.44) cures, favoring pubovaginal sling. Therewas no difference in the groups: midurethral slings versus Burch, pubovaginal sling versus midurethral slings, transobturator slings, minislings versus other slings (objective cure). Retropubic and pubovaginal slings are more retentionist. Retropubic slings have more bladder perforation, and transobturator slings, more leg and groin pain, neurological lesion and vaginal perforation.
Pubovaginal slings are superior to Burch colposuspension surgery but exhibit more retention. Retropubic slings are superior to transobturator slings, with more adverse events. Other slings are superior to minislings in the subjective aspect. There was no difference in the comparisons between midurethral slings versus Burch colposuspension surgery, pubovaginal versus midurethral slings, and inside-out versus outside-in transobturator slings.
Summary
Rev Bras Ginecol Obstet. 2012;34(11):505-510
DOI 10.1590/S0100-72032012001100005
PURPOSE: To investigate the effect of adding biofeedback (BF) to the training of pelvic floor muscles (PFMT) for the treatment of stress urinary incontinence (SUI). METHODS: A prospective pilot study, randomized and controlled with women with SUI without sphincter deficiency, detected by urodynamic study and who performed the correct PFM contraction. Women with neuromuscular disorders and grade III and IV genital prolapse were excluded. Forty women were randomized into a Control Group and BF Group. The PFMT protocol with BF equipment consisted of three sets of ten slow contractions (tonic), with a holding time of six to eight seconds at each contraction followed by a rest period of equal duration. After each sustained contraction, they performed three to four fast contractions (phasic) in the supine and standing position twice a week, for a total of 12 sessions. We evaluated the effect of adding BF to PFMT on quality of life using King's Health Questionnaire (KHQ) regarding urinary symptoms based on a voiding diary and regarding the function of pelvic floor muscles by digital palpation. The evaluation was performed initially and after 12 treatment sessions. Data are reported as mean and standard deviation. The Mann-Whitney test was used for the analysis of homogeneity and to determine differences between groups, and the Wilcoxon test was used to determine possible differences between the times of observation, with the level of significance set at 0.05. RESULTS: A significant decrease in the scores of the domains assessed by the KHQ was observed in the comparison between groups, except for the general health domain (BF Group: 32.8±26.9 versus Control Group: 48.4±29.5, p<0.13). Accordingly, there was improvement in PFM function after treatment in the BF Group, regarding power (4.3±0.8, p= 0.001), endurance (6.0±2.2, p<0.001) and fast (9.3±1.9, p=0.001). When comparing the groups, the BF Group showed a positive result regarding power (BF Group 4.3±0.8 versus Control Group 2.5±0.9, p<0.001), endurance (6.0±2.2 BF Group versus Control Group 2.7±1.9, p<0.001) and fast (BF Group 9.3±1.9 versus Control Group 4.6 ± 3.2, p<0.001). Reduction of nocturnal urinary frequency (1.2±1.2 versus 0.7±0.9, p=0.02) and of effort urine loss (1.5±1.4 versus 0.6±0.8, p=0.001) was observed in the BF Group. CONCLUSION: The addition of BF to the PFMT for the treatment of SUI, applied according to the protocol described, improved PFM function, reduced urinary symptoms, and improved of the quality of life.
Summary
Rev Bras Ginecol Obstet. 2012;34(11):505-510
DOI 10.1590/S0100-72032012001100005
PURPOSE: To investigate the effect of adding biofeedback (BF) to the training of pelvic floor muscles (PFMT) for the treatment of stress urinary incontinence (SUI). METHODS: A prospective pilot study, randomized and controlled with women with SUI without sphincter deficiency, detected by urodynamic study and who performed the correct PFM contraction. Women with neuromuscular disorders and grade III and IV genital prolapse were excluded. Forty women were randomized into a Control Group and BF Group. The PFMT protocol with BF equipment consisted of three sets of ten slow contractions (tonic), with a holding time of six to eight seconds at each contraction followed by a rest period of equal duration. After each sustained contraction, they performed three to four fast contractions (phasic) in the supine and standing position twice a week, for a total of 12 sessions. We evaluated the effect of adding BF to PFMT on quality of life using King's Health Questionnaire (KHQ) regarding urinary symptoms based on a voiding diary and regarding the function of pelvic floor muscles by digital palpation. The evaluation was performed initially and after 12 treatment sessions. Data are reported as mean and standard deviation. The Mann-Whitney test was used for the analysis of homogeneity and to determine differences between groups, and the Wilcoxon test was used to determine possible differences between the times of observation, with the level of significance set at 0.05. RESULTS: A significant decrease in the scores of the domains assessed by the KHQ was observed in the comparison between groups, except for the general health domain (BF Group: 32.8±26.9 versus Control Group: 48.4±29.5, p<0.13). Accordingly, there was improvement in PFM function after treatment in the BF Group, regarding power (4.3±0.8, p= 0.001), endurance (6.0±2.2, p<0.001) and fast (9.3±1.9, p=0.001). When comparing the groups, the BF Group showed a positive result regarding power (BF Group 4.3±0.8 versus Control Group 2.5±0.9, p<0.001), endurance (6.0±2.2 BF Group versus Control Group 2.7±1.9, p<0.001) and fast (BF Group 9.3±1.9 versus Control Group 4.6 ± 3.2, p<0.001). Reduction of nocturnal urinary frequency (1.2±1.2 versus 0.7±0.9, p=0.02) and of effort urine loss (1.5±1.4 versus 0.6±0.8, p=0.001) was observed in the BF Group. CONCLUSION: The addition of BF to the PFMT for the treatment of SUI, applied according to the protocol described, improved PFM function, reduced urinary symptoms, and improved of the quality of life.
Summary
Rev Bras Ginecol Obstet. 2016;38(10):518-523
To translate into Portuguese, culturally adapt and validate the Uterine Fibroid Symptom - Quality of Life (UFS-QoL) questionnaire for Brazilian women with uterine leiomyoma.
Initially, the UFS-QoL questionnaire was translated into Brazilian Portuguese in accordance with international standards, with subsequent cultural, structural, conceptual and semantic adaptations, so that patients were able to properly answer the questionnaire. Fifty patients with uterine leiomyoma and 19 patients without the disease, confirmed by abdominal pelvic examination and/or transvaginal ultrasound, were selected at the outpatient clinics of the Department of Gynecology of the Universidade Federal de São Paulo (Unifesp). The UFS-QoL questionnaire was administered to all women twice on the same day, with two different interviewers, with an interval of 15 minutes between interviews. After 15 days, the questionnaire was readministered by the first interviewer. Reliability (internal consistency and test-retest), construct and discriminative validity were tested to ratify the questionnaire.
The reliability of the instrument was assessed by Cronbach’s α coefficient with an overall result of 0.97, indicating high reliability. The survey results showed a high correlation (p= 0.94; p 0.001).
The UFS-QoL questionnaire was successfully adapted to the Brazilian Portuguese language and Brazilian culture, showing reliability and validity.
Summary
Rev Bras Ginecol Obstet. 2016;38(10):518-523
To translate into Portuguese, culturally adapt and validate the Uterine Fibroid Symptom - Quality of Life (UFS-QoL) questionnaire for Brazilian women with uterine leiomyoma.
Initially, the UFS-QoL questionnaire was translated into Brazilian Portuguese in accordance with international standards, with subsequent cultural, structural, conceptual and semantic adaptations, so that patients were able to properly answer the questionnaire. Fifty patients with uterine leiomyoma and 19 patients without the disease, confirmed by abdominal pelvic examination and/or transvaginal ultrasound, were selected at the outpatient clinics of the Department of Gynecology of the Universidade Federal de São Paulo (Unifesp). The UFS-QoL questionnaire was administered to all women twice on the same day, with two different interviewers, with an interval of 15 minutes between interviews. After 15 days, the questionnaire was readministered by the first interviewer. Reliability (internal consistency and test-retest), construct and discriminative validity were tested to ratify the questionnaire.
The reliability of the instrument was assessed by Cronbach’s α coefficient with an overall result of 0.97, indicating high reliability. The survey results showed a high correlation (p= 0.94; p 0.001).
The UFS-QoL questionnaire was successfully adapted to the Brazilian Portuguese language and Brazilian culture, showing reliability and validity.
Summary
Rev Bras Ginecol Obstet. 2007;29(10):519-524
DOI 10.1590/S0100-72032007001000005
PURPOSE: to identify the impact of pelvic reconstructive surgery on female sexual function, as well as the changes in vaginal anatomy, and to detect possible correlations between them. METHODS: a prospective, descriptive study, including 43 sexually active women with genital dystopy, undergoing surgery for pelvic organ prolapse, conducted between October 2004 and September 2006. The women completed the same multiple-choice questionnaire regarding sexual function, and analogic scales to quantify the degree of desire, arousal and satisfaction, and were clinically assessed using the pelvic organ prolapse quantification (POP-Q) staging system, before the surgery and three and six months after it. Statistical analysis was performed through the Bowker test for symmetry, Wilcoxon test, Student t test, chi2 and analysis of variance (ANOVA) as appropriate, with statistical significance set at 5% (p<0.05). RESULTS: all 43 women completed the follow-up at three and six months after the surgery, but two of them lost their partners after the surgery. Quality of sexual life improved significantly (p=0.03). Symptoms such as dyspareunia (25.6% before versus 17.1% after surgery), discomfort (27.9 versus 0%), embarrassment (20.9% versus 0%) and fear (2.3% versus 0%) significantly improved (p<0.001). Analogical scales scores regarding desire (5 versus 7, p=0.001), arousal (6 versus 8, p<0.001) and satisfaction with sexual life (5 versus 7, p<0.001) also improved. There was a statistically significant improvement (p<0.001) of the POP-Q stages after the surgery. However, there was no statistically significant correlation between changes in vaginal dimensions and changes in sexual function. CONCLUSIONS: after pelvic reconstructive surgery, there was a significant improvement in the quality of sexual life and of the POP-Q stages. However, there was no correlation between them.
Summary
Rev Bras Ginecol Obstet. 2007;29(10):519-524
DOI 10.1590/S0100-72032007001000005
PURPOSE: to identify the impact of pelvic reconstructive surgery on female sexual function, as well as the changes in vaginal anatomy, and to detect possible correlations between them. METHODS: a prospective, descriptive study, including 43 sexually active women with genital dystopy, undergoing surgery for pelvic organ prolapse, conducted between October 2004 and September 2006. The women completed the same multiple-choice questionnaire regarding sexual function, and analogic scales to quantify the degree of desire, arousal and satisfaction, and were clinically assessed using the pelvic organ prolapse quantification (POP-Q) staging system, before the surgery and three and six months after it. Statistical analysis was performed through the Bowker test for symmetry, Wilcoxon test, Student t test, chi2 and analysis of variance (ANOVA) as appropriate, with statistical significance set at 5% (p<0.05). RESULTS: all 43 women completed the follow-up at three and six months after the surgery, but two of them lost their partners after the surgery. Quality of sexual life improved significantly (p=0.03). Symptoms such as dyspareunia (25.6% before versus 17.1% after surgery), discomfort (27.9 versus 0%), embarrassment (20.9% versus 0%) and fear (2.3% versus 0%) significantly improved (p<0.001). Analogical scales scores regarding desire (5 versus 7, p=0.001), arousal (6 versus 8, p<0.001) and satisfaction with sexual life (5 versus 7, p<0.001) also improved. There was a statistically significant improvement (p<0.001) of the POP-Q stages after the surgery. However, there was no statistically significant correlation between changes in vaginal dimensions and changes in sexual function. CONCLUSIONS: after pelvic reconstructive surgery, there was a significant improvement in the quality of sexual life and of the POP-Q stages. However, there was no correlation between them.
Summary
Rev Bras Ginecol Obstet. 2017;39(10):534-540
The presence of bacteria in urine is called bacteriuria, which may be symptomatic or asymptomatic. The manipulation of the urinary tract during urodynamic study (UDS), which is an invasive procedure, can result in urinary tract infection (UTI). Studies on the use of prophylactic antibiotics for UDSs are contradictory. Some investigators concluded that they were valuable and others did not. The objective of this study is to evaluate the efficacy of antibiotic prophylaxis before UDS. This is a placebo-control randomized double-blind study.
Two-hundred and seventeen women affected by urinary incontinence were eligible for this study. All patients had presented negative urine culture previous to the UDS. They were randomized in four groups: group A received placebo, group B received 500 mg of levofloxacin, group C received 80 mg trimethoprim and 400 mg sulfamethoxazole and group D received 100 mg of nitrofurantoin. A urine culture was performed 14 days after the UDS.
We observed asymptomatic bacteriuria after the UDS in five patients in group A, one in group B, one in group C and one in group D. Only one patient on group A had symptomatic bacteriuria.We didn’t observe statistical difference between the groups. When we recategorized the patients in two groups, the incidence of bacteriuria was significantly higher in the placebo group compared with the antibiotic group.
The conclusion is that antibiotic prophylaxis before the UDS did not reduce the incidence of UTI in women within the target population.
Summary
Rev Bras Ginecol Obstet. 2017;39(10):534-540
The presence of bacteria in urine is called bacteriuria, which may be symptomatic or asymptomatic. The manipulation of the urinary tract during urodynamic study (UDS), which is an invasive procedure, can result in urinary tract infection (UTI). Studies on the use of prophylactic antibiotics for UDSs are contradictory. Some investigators concluded that they were valuable and others did not. The objective of this study is to evaluate the efficacy of antibiotic prophylaxis before UDS. This is a placebo-control randomized double-blind study.
Two-hundred and seventeen women affected by urinary incontinence were eligible for this study. All patients had presented negative urine culture previous to the UDS. They were randomized in four groups: group A received placebo, group B received 500 mg of levofloxacin, group C received 80 mg trimethoprim and 400 mg sulfamethoxazole and group D received 100 mg of nitrofurantoin. A urine culture was performed 14 days after the UDS.
We observed asymptomatic bacteriuria after the UDS in five patients in group A, one in group B, one in group C and one in group D. Only one patient on group A had symptomatic bacteriuria.We didn’t observe statistical difference between the groups. When we recategorized the patients in two groups, the incidence of bacteriuria was significantly higher in the placebo group compared with the antibiotic group.
The conclusion is that antibiotic prophylaxis before the UDS did not reduce the incidence of UTI in women within the target population.
Summary
Rev Bras Ginecol Obstet. 2006;28(1):54-62
DOI 10.1590/S0100-72032006000100010
Female lower urinary tract symptoms are nonspecific and a clinical evaluation is required to establish the correct diagnosis. Such evaluation should consist of a structured micturition history or questionnaire, physical examination, micturition diary, pad test, and urodynamic evaluation. Urodynamic investigation was developed as an extension of patient history and physical examination in order to reveal the etiology of the patient's complaints. The goal of the present article is to review clinical and subsidiary diagnosis of urinary incontinence.
Summary
Rev Bras Ginecol Obstet. 2006;28(1):54-62
DOI 10.1590/S0100-72032006000100010
Female lower urinary tract symptoms are nonspecific and a clinical evaluation is required to establish the correct diagnosis. Such evaluation should consist of a structured micturition history or questionnaire, physical examination, micturition diary, pad test, and urodynamic evaluation. Urodynamic investigation was developed as an extension of patient history and physical examination in order to reveal the etiology of the patient's complaints. The goal of the present article is to review clinical and subsidiary diagnosis of urinary incontinence.
Summary
Rev Bras Ginecol Obstet. 2002;24(9):573-577
DOI 10.1590/S0100-72032002000900002
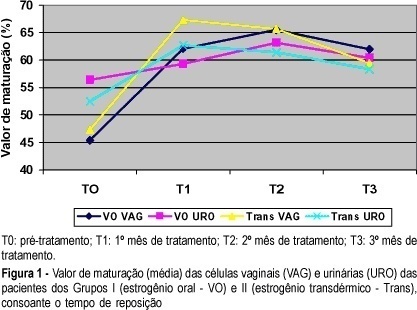
Objective: to study the effects of oral or transdermal estrogen replacement on the lower urinary tract and vagina in postmenopausal women. Methods: we studied 25 postmenopausal women evaluating the oral or transdermic estrogen replacement effects on the vaginal cells and urinary sediment during 3 months. The patients were randomly distributed into 2 groups: Group I, n = 14, treated orally with 0.625 mg equine conjugated estrogen plus 5 mg medroxyprogesterone acetate, daily for 3 months; Group II, n = 11, treated transdermally with 50 mug 17-ß-estradiol, once a week, plus 5 mg medroxyprogesterone. Daily, for 3 months, urinary samples were collected from the first miction in the morning after urogenital antisepsis into sterile tubes. The sample was centrifuged and the sediment was smeared. Vaginal and urinary smears were then fixed in absoluted alcohol and stained by the method of Shorr. Results: the patients who used the oral route presented maturation of the vaginal cells (from 45.4 to 65.5% after 2 months of treatment, maintaing 62% afterwards) but this did not occur with urinary cells (56.4 before treatment versus 60.4% at the end of the period). The transdermal route promoted maturation of vaginal and urinary cells. Conclusion: we have concluded that transdermal estrogens have satisfactory effects both on vaginal and urethral sites. However, with the oral route we did not find the expected results in the urinary tract in all cases.
Summary
Rev Bras Ginecol Obstet. 2002;24(9):573-577
DOI 10.1590/S0100-72032002000900002
Objective: to study the effects of oral or transdermal estrogen replacement on the lower urinary tract and vagina in postmenopausal women. Methods: we studied 25 postmenopausal women evaluating the oral or transdermic estrogen replacement effects on the vaginal cells and urinary sediment during 3 months. The patients were randomly distributed into 2 groups: Group I, n = 14, treated orally with 0.625 mg equine conjugated estrogen plus 5 mg medroxyprogesterone acetate, daily for 3 months; Group II, n = 11, treated transdermally with 50 mug 17-ß-estradiol, once a week, plus 5 mg medroxyprogesterone. Daily, for 3 months, urinary samples were collected from the first miction in the morning after urogenital antisepsis into sterile tubes. The sample was centrifuged and the sediment was smeared. Vaginal and urinary smears were then fixed in absoluted alcohol and stained by the method of Shorr. Results: the patients who used the oral route presented maturation of the vaginal cells (from 45.4 to 65.5% after 2 months of treatment, maintaing 62% afterwards) but this did not occur with urinary cells (56.4 before treatment versus 60.4% at the end of the period). The transdermal route promoted maturation of vaginal and urinary cells. Conclusion: we have concluded that transdermal estrogens have satisfactory effects both on vaginal and urethral sites. However, with the oral route we did not find the expected results in the urinary tract in all cases.
Summary
Rev Bras Ginecol Obstet. 2023;45(10):584-593
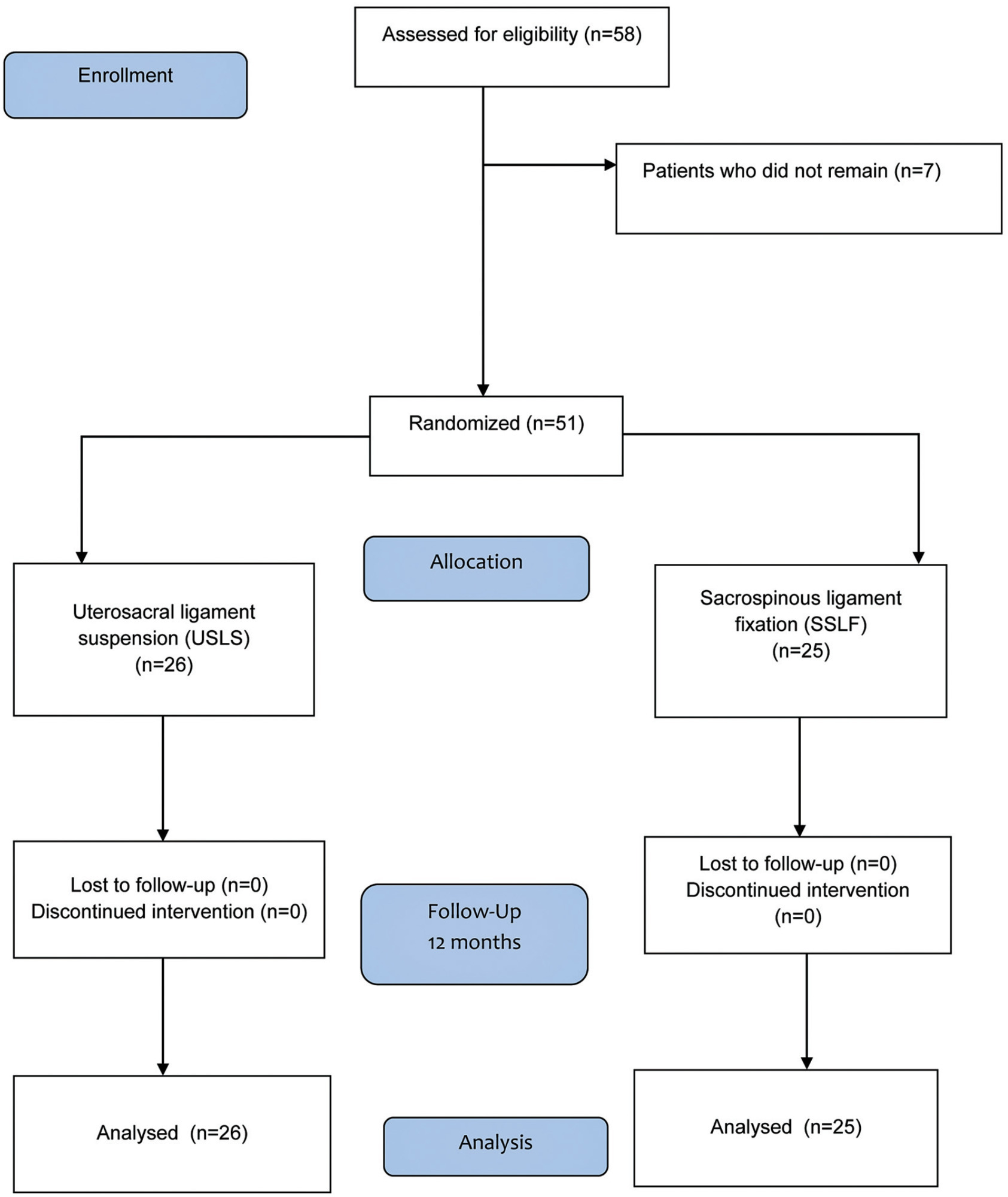
To evaluate the efficacy and outcomes of the surgical treatment for pelvic organ prolapse (POP) in stages III and IV by sacrospinous ligament fixation (SSLF) or uterosacral ligament suspension (USLS) by comparing anatomical and subjective cure rates and quality-of-life parameters (through the version validated for the Portuguese language of the Prolapse Quality of Life [P-QoL] questionnaire) under two definitions: genital prolapse Ba, Bp, and C< −1 (stage I) and Ba, Bp, and C ≤ 0 (stage II).
After we obtained approval from the Ethics Committee (under CAAE 0833/06) and registered the study in ClinicalTrials.gov (NCT 01347021), 51 patients were randomized into two groups: the USLS group (N = 26) and the SSLF group (N = 25), with follow-up 6 and 12 months after the procedures.
There was a significant improvement in the P-QoL score and anatomical measurements of all compartments in both groups after 12 months (p< 0.001). The anatomical cure rates in the USLS and SSLF groups, considering stage 1, were of 34.6% and 40% (anterior) respectively; of 100% both for groups (apical); and of 73.1% and 92% (posterior) respectively. The rates of adverse outcomes were of 42% (N = 11) and 36% (N = 11) for the USLS and SSLF groups respectively (p = 0.654), and those outcomes were excessive bleeding, bladder perforation (intraoperative) or gluteal pain, and urinary infection (postoperative), among others, without differences between the groups.
High cure rates in all compartments were observed according to the anatomical criterion (stage I), without differences in P-QoL scores and complications either with USLS or SSLF for the surgical treatment of accentuated POP.
Summary
Rev Bras Ginecol Obstet. 2023;45(10):584-593
To evaluate the efficacy and outcomes of the surgical treatment for pelvic organ prolapse (POP) in stages III and IV by sacrospinous ligament fixation (SSLF) or uterosacral ligament suspension (USLS) by comparing anatomical and subjective cure rates and quality-of-life parameters (through the version validated for the Portuguese language of the Prolapse Quality of Life [P-QoL] questionnaire) under two definitions: genital prolapse Ba, Bp, and C< −1 (stage I) and Ba, Bp, and C ≤ 0 (stage II).
After we obtained approval from the Ethics Committee (under CAAE 0833/06) and registered the study in ClinicalTrials.gov (NCT 01347021), 51 patients were randomized into two groups: the USLS group (N = 26) and the SSLF group (N = 25), with follow-up 6 and 12 months after the procedures.
There was a significant improvement in the P-QoL score and anatomical measurements of all compartments in both groups after 12 months (p< 0.001). The anatomical cure rates in the USLS and SSLF groups, considering stage 1, were of 34.6% and 40% (anterior) respectively; of 100% both for groups (apical); and of 73.1% and 92% (posterior) respectively. The rates of adverse outcomes were of 42% (N = 11) and 36% (N = 11) for the USLS and SSLF groups respectively (p = 0.654), and those outcomes were excessive bleeding, bladder perforation (intraoperative) or gluteal pain, and urinary infection (postoperative), among others, without differences between the groups.
High cure rates in all compartments were observed according to the anatomical criterion (stage I), without differences in P-QoL scores and complications either with USLS or SSLF for the surgical treatment of accentuated POP.