Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(9):420-424
DOI 10.1590/S0100-72032012000900006
PURPOSE: To evaluate the association between ovarian endometrioma and the presence of deep infiltrating endometriosis (DIE) lesions in a sample of women of the South of Brazil. METHODS: A retrospective study was conducted in all women undergoing surgical treatment of endometriosis from January 2010 to June 2012. Patients were divided into 2 groups according to the presence or not of ovarian endometrioma. Patients presenting an ovarian endometrioma were subsequently divided into 2 groups according to the diameter of the endometrioma (<40 and >40 mm). The following parameters were compared between the groups: cancer antigen (CA) 125 level, size of the endometrioma, presence and number of deep lesions. The statistical analysis was performed with Statistica version 8.0 using Fisher's exact test, Student's t-test and Mann-Whitney test, when needed. The p values of <0.05 were considered statistically significant. RESULTS: During the study period, a total of 201 women underwent laparoscopic surgical treatment of endometriosis. Fifty-five patients (27.9%) presented ovarian endometrioma and 180 patients (89.5%) presented DIE confirmed by pathologic examination. Women presenting an ovarian endometrioma had higher CA 125 levels (39.5 versus 24.1 U/mL; p<0.01) and stronger association with the presence of DIE lesions (98.2 versus 86.2%; p=0.01) and intestinal DIE (57.1 versus 37.9%; p=0.01). There was no difference between the groups with endometriomas <40 and >40 mm. CONCLUSIONS: Ovarian endometrioma is a marker for the presence of DIE lesions, including intestinal DIE.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2012;34(9):420-424
DOI 10.1590/S0100-72032012000900006
PURPOSE: To evaluate the association between ovarian endometrioma and the presence of deep infiltrating endometriosis (DIE) lesions in a sample of women of the South of Brazil. METHODS: A retrospective study was conducted in all women undergoing surgical treatment of endometriosis from January 2010 to June 2012. Patients were divided into 2 groups according to the presence or not of ovarian endometrioma. Patients presenting an ovarian endometrioma were subsequently divided into 2 groups according to the diameter of the endometrioma (<40 and >40 mm). The following parameters were compared between the groups: cancer antigen (CA) 125 level, size of the endometrioma, presence and number of deep lesions. The statistical analysis was performed with Statistica version 8.0 using Fisher's exact test, Student's t-test and Mann-Whitney test, when needed. The p values of <0.05 were considered statistically significant. RESULTS: During the study period, a total of 201 women underwent laparoscopic surgical treatment of endometriosis. Fifty-five patients (27.9%) presented ovarian endometrioma and 180 patients (89.5%) presented DIE confirmed by pathologic examination. Women presenting an ovarian endometrioma had higher CA 125 levels (39.5 versus 24.1 U/mL; p<0.01) and stronger association with the presence of DIE lesions (98.2 versus 86.2%; p=0.01) and intestinal DIE (57.1 versus 37.9%; p=0.01). There was no difference between the groups with endometriomas <40 and >40 mm. CONCLUSIONS: Ovarian endometrioma is a marker for the presence of DIE lesions, including intestinal DIE.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):420-420
DOI 10.1590/S0100-72032002000600014
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):420-420
DOI 10.1590/S0100-72032002000600014
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):420-421
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):420-421
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(9):420-425
DOI 10.1590/S0100-72032010000900002
PURPOSE: to compare the patterns of fetal heart rate (FHR) in the second and third trimesters of pregnancy. METHODS: a prospective and comparative study performed between January 2008 and July 2009. The inclusion criteria were: singleton pregnancy, live fetus, pregnant women without clinical or obstetrical complications, no fetal malformation, gestational age between 24 and 27 weeks (2nd trimester - 2T) or between 36 and 40 weeks (3rd trimester - 3T). Computerized cardiotocography (System 8002 - Sonicaid) was performed for 30 minutes and the fetal biophysical profile was obtained. System 8002 analyzes the FHR tracings for periods of 3.75 seconds (1/16 minutes). During each period, the mean duration of the time intervals between successive fetal heart beats is determined in milliseconds (ms); the mean FHR and also the differences between adjacent periods are calculated for each period. The parameters included: basal FHR, FHR accelerations, duration of high variation episodes, duration of low variation episodes and short-term variation. The dataset was analyzed by the Student t test, chi-square test and Fisher's exact test. Statistical significance was set at p<0.05. RESULTS: eighteen pregnancies on the second trimester were compared to 25 pregnancies on the third trimester. There was a significant difference in the FHR parameters evaluated by computerized cardiotocography between the 2T and 3T groups, regarding the following results: mean basal FHR (mean, 143.8 bpm versus 134.0 bpm, p=0.009), mean number of transitory FHR accelerations > 10 bpm (3.7 bpm versus 8.4 bpm, p <0.001) and >15 bpm (mean, 0.9 bpm versus 5.4 bpm, p <0.001), mean duration of high variation episodes (8.4 min versus 15.4 min, p=0.008) and mean short - term variation (8.0 ms versus 10.9 ms, p=0.01). The fetal biophysical profile showed normal results in all pregnancies. CONCLUSION: the present study shows significant differences in the FHR characteristics when the 2nd and 3rd trimesters of pregnancy are compared and confirms the influence of autonomic nervous system maturation on FHR regulation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(9):420-425
DOI 10.1590/S0100-72032010000900002
PURPOSE: to compare the patterns of fetal heart rate (FHR) in the second and third trimesters of pregnancy. METHODS: a prospective and comparative study performed between January 2008 and July 2009. The inclusion criteria were: singleton pregnancy, live fetus, pregnant women without clinical or obstetrical complications, no fetal malformation, gestational age between 24 and 27 weeks (2nd trimester - 2T) or between 36 and 40 weeks (3rd trimester - 3T). Computerized cardiotocography (System 8002 - Sonicaid) was performed for 30 minutes and the fetal biophysical profile was obtained. System 8002 analyzes the FHR tracings for periods of 3.75 seconds (1/16 minutes). During each period, the mean duration of the time intervals between successive fetal heart beats is determined in milliseconds (ms); the mean FHR and also the differences between adjacent periods are calculated for each period. The parameters included: basal FHR, FHR accelerations, duration of high variation episodes, duration of low variation episodes and short-term variation. The dataset was analyzed by the Student t test, chi-square test and Fisher's exact test. Statistical significance was set at p<0.05. RESULTS: eighteen pregnancies on the second trimester were compared to 25 pregnancies on the third trimester. There was a significant difference in the FHR parameters evaluated by computerized cardiotocography between the 2T and 3T groups, regarding the following results: mean basal FHR (mean, 143.8 bpm versus 134.0 bpm, p=0.009), mean number of transitory FHR accelerations > 10 bpm (3.7 bpm versus 8.4 bpm, p <0.001) and >15 bpm (mean, 0.9 bpm versus 5.4 bpm, p <0.001), mean duration of high variation episodes (8.4 min versus 15.4 min, p=0.008) and mean short - term variation (8.0 ms versus 10.9 ms, p=0.01). The fetal biophysical profile showed normal results in all pregnancies. CONCLUSION: the present study shows significant differences in the FHR characteristics when the 2nd and 3rd trimesters of pregnancy are compared and confirms the influence of autonomic nervous system maturation on FHR regulation.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):420-426
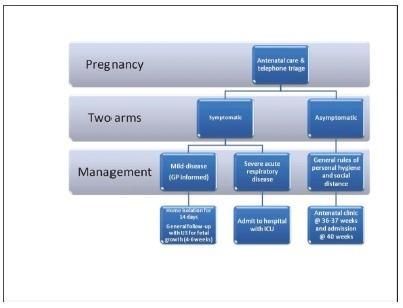
Since the World Health Organization (WHO) declared coronavirus infection (COVID-19) a Public Health Emergency of International Concern in January 2020, there have been many concerns about pregnant women and the possible effects of this emergency with catastrophic outcomes inmany countries. Information on COVID-19 and pregnancy are scarce and spread throughout a fewcase series, with no more than 50 cases in total. The present review provides a brief analysis of COVID-19, pregnancy in the COVID-19 era, and the effects of COVID-19 on pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(7):420-426
Since the World Health Organization (WHO) declared coronavirus infection (COVID-19) a Public Health Emergency of International Concern in January 2020, there have been many concerns about pregnant women and the possible effects of this emergency with catastrophic outcomes inmany countries. Information on COVID-19 and pregnancy are scarce and spread throughout a fewcase series, with no more than 50 cases in total. The present review provides a brief analysis of COVID-19, pregnancy in the COVID-19 era, and the effects of COVID-19 on pregnancy.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):421-421
DOI 10.1590/S0100-72032002000600016
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(6):421-421
DOI 10.1590/S0100-72032002000600016
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):421-428
DOI 10.1590/S0100-72032000000700004
Purpose: to evaluate 24 cases of gastroschisis, in relation to the prognostic factors that interfered with postnatal outcome. Patients and Method: twenty-four pregnancies with fetal prenatal ultrasound diagnosis of gastroschisis, during an 8-year period, were analyzed. Gastroschisis was classified into isolated, when there were no other structural abnormalities, or associated, when other abnormalities were present. For both groups the following parameters were examined: ultrasound bowel dilatation (>18 mm), obstetric complications and postnatal outcome. Nonparametric Mann-Whitney and exact Fisher's tests were used for statistical analyses. Results: in 9 cases (37.5%) gastroschisis was associated with other abnormalities, and in 15 cases it was isolated (62.5%). All cases of associated gastroschisis had a letal prognosis, therefore the overall mortality rate was 60.8%. In the group of isolated gastroschisis, all were born alive and were submitted to surgery, but the survival rate after surgical correction was 60%. The median gestational age at birth was 35 weeks and birth weight 2,365 grams. Premature delivery was observed in 10 cases, mainly as a consequence of obstetric complication. Two newborns were small for gestational age, and only 3 had birth weight >2,500 grams. Oligohydramnios was found in 46.6% and it was more frequent in the group of postnatal death (66.7%). Ultrasound assessment of bowel showed bowel dilatation in 86.6%, however, without relation to the prognosis and postnatal bowel findings. There was no significant difference between gestational age at birth and birth weight comparing the survivor and postnatal death groups. Conclusions: isolated gastroschisis had a better prognosis when compared to associated, therefore this prenatal differentiation is important. Isolated gastroschisis was often associated with prematurity, small birth weight and obstetric complications. Prenatal diagnosis allows better monitoring of fetal and obstetric conditions. Delivery should be at term, unless presenting with obstetric complications.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(7):421-428
DOI 10.1590/S0100-72032000000700004
Purpose: to evaluate 24 cases of gastroschisis, in relation to the prognostic factors that interfered with postnatal outcome. Patients and Method: twenty-four pregnancies with fetal prenatal ultrasound diagnosis of gastroschisis, during an 8-year period, were analyzed. Gastroschisis was classified into isolated, when there were no other structural abnormalities, or associated, when other abnormalities were present. For both groups the following parameters were examined: ultrasound bowel dilatation (>18 mm), obstetric complications and postnatal outcome. Nonparametric Mann-Whitney and exact Fisher's tests were used for statistical analyses. Results: in 9 cases (37.5%) gastroschisis was associated with other abnormalities, and in 15 cases it was isolated (62.5%). All cases of associated gastroschisis had a letal prognosis, therefore the overall mortality rate was 60.8%. In the group of isolated gastroschisis, all were born alive and were submitted to surgery, but the survival rate after surgical correction was 60%. The median gestational age at birth was 35 weeks and birth weight 2,365 grams. Premature delivery was observed in 10 cases, mainly as a consequence of obstetric complication. Two newborns were small for gestational age, and only 3 had birth weight >2,500 grams. Oligohydramnios was found in 46.6% and it was more frequent in the group of postnatal death (66.7%). Ultrasound assessment of bowel showed bowel dilatation in 86.6%, however, without relation to the prognosis and postnatal bowel findings. There was no significant difference between gestational age at birth and birth weight comparing the survivor and postnatal death groups. Conclusions: isolated gastroschisis had a better prognosis when compared to associated, therefore this prenatal differentiation is important. Isolated gastroschisis was often associated with prematurity, small birth weight and obstetric complications. Prenatal diagnosis allows better monitoring of fetal and obstetric conditions. Delivery should be at term, unless presenting with obstetric complications.