You searched for:"Marair Gracio Ferreira Sartori"
We found (29) results for your search.Summary
Rev Bras Ginecol Obstet. 1999;21(1):33-37
DOI 10.1590/S0100-72031999000100006
Purpose: to evaluate the agreement between the urodynamic and ultrasonography diagnoses of urinary incontinence, as well as to correlate the variables of both examinations. Methodology: three hundred eighty-one patients with urine loss were selected, from the Sectior of Urogynecology and Vaginal Surgery of the Division of Gynecology, Escola Paulista de Medicina - Federal University of São Paulo. All of them were submitted to urodynamic study, according to the standardization of the International Society of Continence, and to ultrasonography of the bladder neck, with a 6 MHz trasvaginal transducer. We analyzed the maximum closing urethral pressure (MCUP) and the etiological diagnosis of the urine loss. In the ultrasonography, the position of the bladder neck was evaluated in relation to the inferior border of the pubic symphysis, and its mobility as well as the diameter of the urethra and bladder neck. The women were categoriaed according to the urodynamic study in to stress urinary incontinence, detrusor instability and mixed urinary incontinence. Results: 1) the bladder neck, at rest was most frequently above the inferior border of the pubic symphysis and, during effort, below or at the height of the bony reference, in the three groups; 2) the mobility of the bladder neck was similar in the groups; 3) there was no significant correlation between MCUP and the diameter of the urethra and of the bladder neck. Conclusion: we deem that ultrasonography of the bladder neck is always a complement to the clinical evaluation and the urodymanic study.
Summary
Rev Bras Ginecol Obstet. 1999;21(1):33-37
DOI 10.1590/S0100-72031999000100006
Purpose: to evaluate the agreement between the urodynamic and ultrasonography diagnoses of urinary incontinence, as well as to correlate the variables of both examinations. Methodology: three hundred eighty-one patients with urine loss were selected, from the Sectior of Urogynecology and Vaginal Surgery of the Division of Gynecology, Escola Paulista de Medicina - Federal University of São Paulo. All of them were submitted to urodynamic study, according to the standardization of the International Society of Continence, and to ultrasonography of the bladder neck, with a 6 MHz trasvaginal transducer. We analyzed the maximum closing urethral pressure (MCUP) and the etiological diagnosis of the urine loss. In the ultrasonography, the position of the bladder neck was evaluated in relation to the inferior border of the pubic symphysis, and its mobility as well as the diameter of the urethra and bladder neck. The women were categoriaed according to the urodynamic study in to stress urinary incontinence, detrusor instability and mixed urinary incontinence. Results: 1) the bladder neck, at rest was most frequently above the inferior border of the pubic symphysis and, during effort, below or at the height of the bony reference, in the three groups; 2) the mobility of the bladder neck was similar in the groups; 3) there was no significant correlation between MCUP and the diameter of the urethra and of the bladder neck. Conclusion: we deem that ultrasonography of the bladder neck is always a complement to the clinical evaluation and the urodymanic study.
Summary
Rev Bras Ginecol Obstet. 2023;45(6):337-346
To compare the use of mirabegron with anticholinergics drugs for the treatment of overactive bladder (OB).
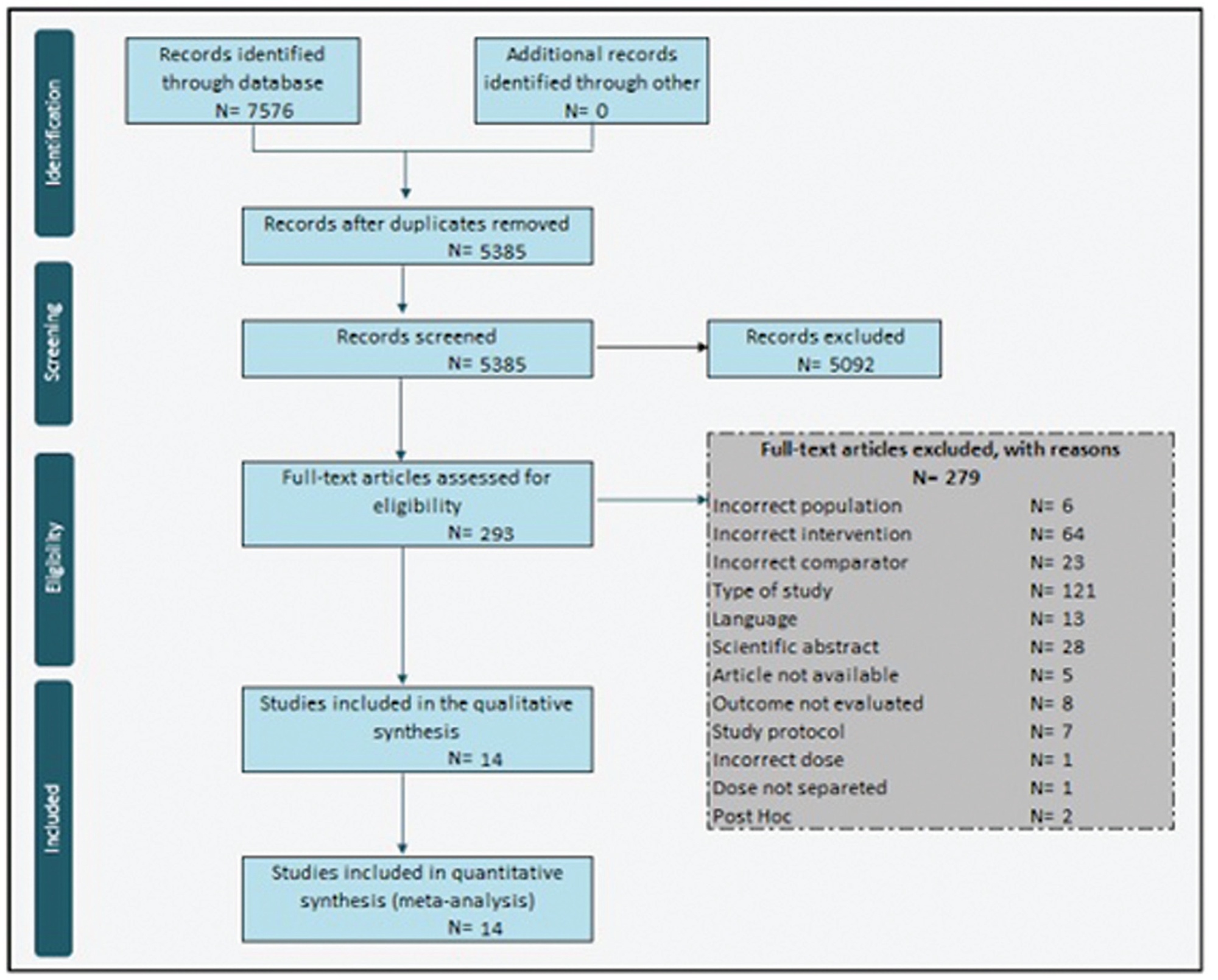
Systematic searches were conducted in EMBASE, PUBMED, Cochrane, and LILACS databases from inception to September 2021. We included RCTs, women with clinically proven OB symptoms, studies that compared mirabegron to antimuscarinic drugs, and that evaluated the efficacy, safety or adherence.
RevMan 5.4 was used to combine results across studies. We derived risk ratios (RRs) and mean differences with 95% CIs using a random-effects meta-analytic model. Cochrane Collaboration Tool and GRADE was applied for risk of bias and quality of the evidence.
We included 14 studies with a total of 10,774 patients. Fewer total adverse events was reported in mirabegron group than in antimuscarinics group [RR 0.93 (0.89–0.98)]. The risk of gastrointestinal tract disorders and dry mouth were lower with mirabegron [RR 0,58 (0.48–0.68); 9375 patients; RR 0.44 (0.35–0.56), 9375 patients, respectively]. No difference was reported between mirabegron and antimuscarinics drugs for efficacy. The adherence to treatment was 87.7% in both groups [RR 0.99 (0.98–1.00)].
Mirabegron and antimuscarinics have comparable efficacy and adherence rates; however, mirabegron showed fewer total and isolated adverse events.
Summary
Rev Bras Ginecol Obstet. 2023;45(6):337-346
To compare the use of mirabegron with anticholinergics drugs for the treatment of overactive bladder (OB).
Systematic searches were conducted in EMBASE, PUBMED, Cochrane, and LILACS databases from inception to September 2021. We included RCTs, women with clinically proven OB symptoms, studies that compared mirabegron to antimuscarinic drugs, and that evaluated the efficacy, safety or adherence.
RevMan 5.4 was used to combine results across studies. We derived risk ratios (RRs) and mean differences with 95% CIs using a random-effects meta-analytic model. Cochrane Collaboration Tool and GRADE was applied for risk of bias and quality of the evidence.
We included 14 studies with a total of 10,774 patients. Fewer total adverse events was reported in mirabegron group than in antimuscarinics group [RR 0.93 (0.89–0.98)]. The risk of gastrointestinal tract disorders and dry mouth were lower with mirabegron [RR 0,58 (0.48–0.68); 9375 patients; RR 0.44 (0.35–0.56), 9375 patients, respectively]. No difference was reported between mirabegron and antimuscarinics drugs for efficacy. The adherence to treatment was 87.7% in both groups [RR 0.99 (0.98–1.00)].
Mirabegron and antimuscarinics have comparable efficacy and adherence rates; however, mirabegron showed fewer total and isolated adverse events.
Summary
Rev Bras Ginecol Obstet. 2003;25(5):353-358
DOI 10.1590/S0100-72032003000500008
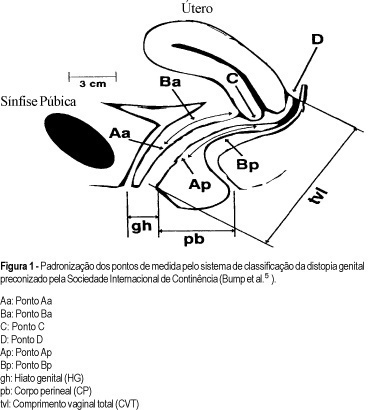
PURPOSE: to determine interobserver reliability of site-specific measurements and stages according to the proposed International Continence Society prolapse terminology document. METHODS: we analyzed 51 women during urogynecological investigation performed at the Urogynecology and Vaginal Surgery Sector of UNIFESP / EPM. We recorded the locations of point-specific measures proposed by the International Continence Society (ICS). They are: two in the anterior vaginal wall, two in the superior vagina, two in the posterior vaginal wall, genital hiatus, perineal body and total vaginal length. Then we recorded the stage of genital prolapse. Women underwent pelvic examinations by two investigators, each blinded to the results of the other's examination. The reproducibility of the nine site-specific measurements and the summary stage were analyzed using Pearson's correlation coefficient and the median measurements were compared by the paired-t test. RESULTS: there were substantial and highly significant correlations for each of the nine measurements. Correlation coefficient for point Aa was 0.89 (p<0.0001), point Ba 0.90 (p<0.0001), point C 0.97 (p<0.0001), point Ap de 0.72 (p<0.0001), point Bp 0.84 (p<0.0001), point D 0.91 (p<0.0001), genital hiatus 0.65 (p<0.0001), perineal body 0.66 (p<0.0001) e total vaginal length 0.73 (p<0.0001). We also did not note differences between the means of measurements by the two examiners. Staging was highly reproducible (r=0.81, p<0.0001). ln no subject did the stage vary by more than one; in 86,2%, stages were identical. CONCLUSIONS: there is a good reproducibility of measures using the system proposed by the International Continence Society prolapse terminology document.
Summary
Rev Bras Ginecol Obstet. 2003;25(5):353-358
DOI 10.1590/S0100-72032003000500008
PURPOSE: to determine interobserver reliability of site-specific measurements and stages according to the proposed International Continence Society prolapse terminology document. METHODS: we analyzed 51 women during urogynecological investigation performed at the Urogynecology and Vaginal Surgery Sector of UNIFESP / EPM. We recorded the locations of point-specific measures proposed by the International Continence Society (ICS). They are: two in the anterior vaginal wall, two in the superior vagina, two in the posterior vaginal wall, genital hiatus, perineal body and total vaginal length. Then we recorded the stage of genital prolapse. Women underwent pelvic examinations by two investigators, each blinded to the results of the other's examination. The reproducibility of the nine site-specific measurements and the summary stage were analyzed using Pearson's correlation coefficient and the median measurements were compared by the paired-t test. RESULTS: there were substantial and highly significant correlations for each of the nine measurements. Correlation coefficient for point Aa was 0.89 (p<0.0001), point Ba 0.90 (p<0.0001), point C 0.97 (p<0.0001), point Ap de 0.72 (p<0.0001), point Bp 0.84 (p<0.0001), point D 0.91 (p<0.0001), genital hiatus 0.65 (p<0.0001), perineal body 0.66 (p<0.0001) e total vaginal length 0.73 (p<0.0001). We also did not note differences between the means of measurements by the two examiners. Staging was highly reproducible (r=0.81, p<0.0001). ln no subject did the stage vary by more than one; in 86,2%, stages were identical. CONCLUSIONS: there is a good reproducibility of measures using the system proposed by the International Continence Society prolapse terminology document.
Summary
Rev Bras Ginecol Obstet. 2002;24(6):365-370
DOI 10.1590/S0100-72032002000600002
Purpose: to study the relationship between pelvic floor function and bladder neck mobility in women with and without stress urinary incontinence (SUI), in menacme and postmenopausal. Methods: sixty-one SUI patients were evaluated; 31 of them were in menacme and of these 17 had SUI and 14 did not have any complaint; 30 were postmenopausal and of these, 15 with SUI and 15 without SUI. Simple cystometry and empty supine stress test were performed in those who had urinary incontinence complaint. Bladder neck mobility was studied by ultrasound and by the Q-tip test. To study pelvic floor function, vaginal cones and digital palpation were used. Results: the bladder neck position in the incontinent women (Groups A and C), determined by ultrasound or the Q tip-test, was --11.8 cm in Group A and --12.5 cm in Group C, lower than the continent women, in whom the bladder neck was at +4.4 cm in Group B and +2.3 cm in Group D. There were no differences in bladder neck mobility among the continent menacme (9.1 cm) and postmenopausal (9.5 cm) groups. Also there were no differences among the incontinent groups (17.1 cm for Group A and 16.6 cm for Group C). The bladder neck mobility was greater in the incontinent women (A and C). Continent women had better results on evaluation of pelvic floor muscles than the incontinent ones, even using vaginal cones or digital palpation, and these results were not dependent on the hormonal status. Conclusion: a positive correlation was found between the Q-tip tests and ultrasound, and between test with vaginal cones and digital palpation. No significant correlation was found between pelvic floor function and bladder neck mobility.
Summary
Rev Bras Ginecol Obstet. 2002;24(6):365-370
DOI 10.1590/S0100-72032002000600002
Purpose: to study the relationship between pelvic floor function and bladder neck mobility in women with and without stress urinary incontinence (SUI), in menacme and postmenopausal. Methods: sixty-one SUI patients were evaluated; 31 of them were in menacme and of these 17 had SUI and 14 did not have any complaint; 30 were postmenopausal and of these, 15 with SUI and 15 without SUI. Simple cystometry and empty supine stress test were performed in those who had urinary incontinence complaint. Bladder neck mobility was studied by ultrasound and by the Q-tip test. To study pelvic floor function, vaginal cones and digital palpation were used. Results: the bladder neck position in the incontinent women (Groups A and C), determined by ultrasound or the Q tip-test, was --11.8 cm in Group A and --12.5 cm in Group C, lower than the continent women, in whom the bladder neck was at +4.4 cm in Group B and +2.3 cm in Group D. There were no differences in bladder neck mobility among the continent menacme (9.1 cm) and postmenopausal (9.5 cm) groups. Also there were no differences among the incontinent groups (17.1 cm for Group A and 16.6 cm for Group C). The bladder neck mobility was greater in the incontinent women (A and C). Continent women had better results on evaluation of pelvic floor muscles than the incontinent ones, even using vaginal cones or digital palpation, and these results were not dependent on the hormonal status. Conclusion: a positive correlation was found between the Q-tip tests and ultrasound, and between test with vaginal cones and digital palpation. No significant correlation was found between pelvic floor function and bladder neck mobility.
Summary
Rev Bras Ginecol Obstet. 2002;24(7):433-438
DOI 10.1590/S0100-72032002000700002
Purpose: to analyze the correlation between Valsalva leak point pressure and maximum urethral closure pressure and clinical symptoms in women with stress urinary incontinence. Methods: we analyzed retrospectively 164 patients with urodynamic diagnosis of stress and mixed urinary incontinence established by the Urogynecology and Vaginal Surgery Sector of UNIFESP/EPM. All patients were submmited to medical interview, physical examination and urodynamic study. Patients were divided into groups according to the subjective degree of stress urinary incontinence. Valsalva leak point pressure (VLPP) was measured with a vesical volume of 200 mL. Urethral profile was determined using a flow catheter number 8 with measurement of maximum urethral closure pressure (MUCP). Data were compared by chi², ANOVA and Tukey tests. Results: mean age was 51.2 years (19-82), 76 women (47.2%) were in menacme and 85 (52.8%) in postmenopausal status. Mean parity was 3.9 (0-18). The exact test for trend demonstrated a statistically significant (p<0.0001) correlation between the number of patients with VLPP of 60 cmH2O or less and clinical complaints. The group with severe leakage had mean VLPP of 69.1 cmH2O. The group with moderated leakage had mean VLPP of 84.6 cmH2O and the group with mild leakage had mean VLPP of 90.6 cmH2O. Conclusions: VLPP correlated with the subjective degree of stress urinary incontinence. Higher grades of stress urinary incontinence had a higher likelyhood of a low VLPP. MUCP did not correlate with clinical complaints.
Summary
Rev Bras Ginecol Obstet. 2002;24(7):433-438
DOI 10.1590/S0100-72032002000700002
Purpose: to analyze the correlation between Valsalva leak point pressure and maximum urethral closure pressure and clinical symptoms in women with stress urinary incontinence. Methods: we analyzed retrospectively 164 patients with urodynamic diagnosis of stress and mixed urinary incontinence established by the Urogynecology and Vaginal Surgery Sector of UNIFESP/EPM. All patients were submmited to medical interview, physical examination and urodynamic study. Patients were divided into groups according to the subjective degree of stress urinary incontinence. Valsalva leak point pressure (VLPP) was measured with a vesical volume of 200 mL. Urethral profile was determined using a flow catheter number 8 with measurement of maximum urethral closure pressure (MUCP). Data were compared by chi², ANOVA and Tukey tests. Results: mean age was 51.2 years (19-82), 76 women (47.2%) were in menacme and 85 (52.8%) in postmenopausal status. Mean parity was 3.9 (0-18). The exact test for trend demonstrated a statistically significant (p<0.0001) correlation between the number of patients with VLPP of 60 cmH2O or less and clinical complaints. The group with severe leakage had mean VLPP of 69.1 cmH2O. The group with moderated leakage had mean VLPP of 84.6 cmH2O and the group with mild leakage had mean VLPP of 90.6 cmH2O. Conclusions: VLPP correlated with the subjective degree of stress urinary incontinence. Higher grades of stress urinary incontinence had a higher likelyhood of a low VLPP. MUCP did not correlate with clinical complaints.
Summary
Rev Bras Ginecol Obstet. 2017;39(9):441-442
Summary
Rev Bras Ginecol Obstet. 2017;39(9):441-442
Summary
Rev Bras Ginecol Obstet. 2004;26(6):441-447
DOI 10.1590/S0100-72032004000600004
OBJECTIVE: to compare Baden and Walker's (BW) classification system to the International Continence Society (ICS) standardization of terminology of female pelvic organ prolapse. METHODS: information about urogynecological investigation on 101 women, performed by the Urogynecology and Vaginal Surgery Sector of UNIFESP/EPM, was retrospectively analyzed. Only patients who had undergone the standard ICS exam which quantifies the pelvic prolapse were selected. According to ICS, the prolapse is analyzed through a standard reference system relating the hymen to the anatomic position of six vaginal points: two in the anterior vaginal wall, two in the vaginal apex and other two in the posterior vaginal wall. The maximum amount of pelvic organ prolapse was viewed and recorded during a Valsalva's maneuver. The measurement of the most distal point of the prolapse was performed and it was compared to the BW classification system. The data were analyzed by kappa statistics, to assess the concordance between the two terminologies. RESULTS: There was total correspondence only for the posterior vaginal prolapse stage IV (one patient) and for the uterus prolapse stage 0 (29 patients) with severe rectocele and absence of prolapse, respectively, according to BW. In the three types of prolapses evaluated, the values of kappa statistics were below 0.4, indicating a weak concordance between the two terminologies. There is an extensive variation in the measurement of the most distal point of prolapse when the BW classification is perfomed. CONCLUSIONS: there is a weak concordance between the BW classification system and the ICS standardization of terminology of female pelvic organ prolapse.
Summary
Rev Bras Ginecol Obstet. 2004;26(6):441-447
DOI 10.1590/S0100-72032004000600004
OBJECTIVE: to compare Baden and Walker's (BW) classification system to the International Continence Society (ICS) standardization of terminology of female pelvic organ prolapse. METHODS: information about urogynecological investigation on 101 women, performed by the Urogynecology and Vaginal Surgery Sector of UNIFESP/EPM, was retrospectively analyzed. Only patients who had undergone the standard ICS exam which quantifies the pelvic prolapse were selected. According to ICS, the prolapse is analyzed through a standard reference system relating the hymen to the anatomic position of six vaginal points: two in the anterior vaginal wall, two in the vaginal apex and other two in the posterior vaginal wall. The maximum amount of pelvic organ prolapse was viewed and recorded during a Valsalva's maneuver. The measurement of the most distal point of the prolapse was performed and it was compared to the BW classification system. The data were analyzed by kappa statistics, to assess the concordance between the two terminologies. RESULTS: There was total correspondence only for the posterior vaginal prolapse stage IV (one patient) and for the uterus prolapse stage 0 (29 patients) with severe rectocele and absence of prolapse, respectively, according to BW. In the three types of prolapses evaluated, the values of kappa statistics were below 0.4, indicating a weak concordance between the two terminologies. There is an extensive variation in the measurement of the most distal point of prolapse when the BW classification is perfomed. CONCLUSIONS: there is a weak concordance between the BW classification system and the ICS standardization of terminology of female pelvic organ prolapse.
Summary
Rev Bras Ginecol Obstet. 2009;31(9):447-452
DOI 10.1590/S0100-72032009000900005
PURPOSE: to compare the effects of functional electrostimulation of the pelvic floor and therapy with cones in women with stress urinary incontinence (SUI). METHODS: randomized clinical study for which 45 patients with SUI were selected. The effects of functional electrostimulation of the pelvic floor were evaluated in the SUI treatment of 24 women, with the use of clinical data (micturition diary, pad test and a questionnaire about quality of life - I-QoL). The patients were submitted to two 20' weekly sessions for four consecutive months, under the supervision of a physiotherapist. The electrode used had 10 cm length and 3.5 cm width with a double metallic ring and a cylindrical shape, positioned in the medium third of the vagina. The electric parameters used were: intensity varying from 10 to 100 mA and 50 Hz of fixed frequency, with pulse duration of 1 ms. Also, we evaluated 21 patients who were submitted to vaginal cone treatment. The cone therapy was done with two 45 minute sessions per week. The cones' weight varied from 20 to 100 gr. RESULTS: there was no difference between the outcomes of electrostimulation of the pelvic floor and the vaginal cones for the treatment of SUI (p>0.05). After four months, there was a significant improvement in the I-QoL index of the patients treated both with electrostimulation (40.3 versus 82.9) or with the cones (47.7 versus 84.1). There was a significant decrease in pad weight in both groups, measured before and after the treatment (28.5 and 32 g versus 2.0 and 3.0 g for the electrostimulation and cone group, respectively). Finally, there was a significant decrease in the number of urinary leakage evaluated by the micturition diary in both groups (p<0.0001). CONCLUSIONS: both electrostimulation and vaginal cones were effective in the treatment of women with SUI.
Summary
Rev Bras Ginecol Obstet. 2009;31(9):447-452
DOI 10.1590/S0100-72032009000900005
PURPOSE: to compare the effects of functional electrostimulation of the pelvic floor and therapy with cones in women with stress urinary incontinence (SUI). METHODS: randomized clinical study for which 45 patients with SUI were selected. The effects of functional electrostimulation of the pelvic floor were evaluated in the SUI treatment of 24 women, with the use of clinical data (micturition diary, pad test and a questionnaire about quality of life - I-QoL). The patients were submitted to two 20' weekly sessions for four consecutive months, under the supervision of a physiotherapist. The electrode used had 10 cm length and 3.5 cm width with a double metallic ring and a cylindrical shape, positioned in the medium third of the vagina. The electric parameters used were: intensity varying from 10 to 100 mA and 50 Hz of fixed frequency, with pulse duration of 1 ms. Also, we evaluated 21 patients who were submitted to vaginal cone treatment. The cone therapy was done with two 45 minute sessions per week. The cones' weight varied from 20 to 100 gr. RESULTS: there was no difference between the outcomes of electrostimulation of the pelvic floor and the vaginal cones for the treatment of SUI (p>0.05). After four months, there was a significant improvement in the I-QoL index of the patients treated both with electrostimulation (40.3 versus 82.9) or with the cones (47.7 versus 84.1). There was a significant decrease in pad weight in both groups, measured before and after the treatment (28.5 and 32 g versus 2.0 and 3.0 g for the electrostimulation and cone group, respectively). Finally, there was a significant decrease in the number of urinary leakage evaluated by the micturition diary in both groups (p<0.0001). CONCLUSIONS: both electrostimulation and vaginal cones were effective in the treatment of women with SUI.