You searched for:"Julio César Teixeira"
We found (20) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-334
DOI 10.1590/S0100-72032001000500012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-334
DOI 10.1590/S0100-72032001000500012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(6):347-353
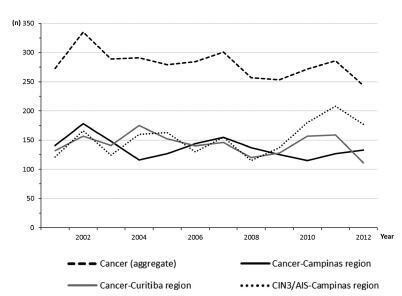
The aim of this study was to assess the time trends and pattern of cervical cancer diagnosed in the period from 2001 to 2012 by means of an opportunistic screening program from two developed regions in Brazil.
An observational study analyzing 3,364 cancer records (n = 1,646 from Campinas and n = 1,718 from Curitiba region) available in hospital-based cancer registries was done. An additional 1,836 records of CIN3/AIS from the region of Campinas was analyzed. The statistical analysis assessed the pooled data and the data by region considering the year of diagnosis, age-group, cancer stage, and histologic type. The Cochran-Armitage trend test was applied and p-values < 0.05 were considered significant.
The total annual cervical cancer registered from2001 to 2012 showed a slight drop (273-244), with an age average of 49.5 y, 13 years over the average for CIN3/AIS (36.8 y). A total of 20.6% of the diagnoses (1.6% under 25 y) were done out of the official screening age-range. The biennial rate of diagnoses by age group for the region of Campinas showed an increase trend for the age groups under 25 y (p = 0.007) and 25 to 44 y (p = 0.003). Stage III was the most recorded for both regions, with an annual average of 43%, without any trend modification. There was an increasing trend for stage I diagnoses in the region of Campinas (p = 0.033). The proportion of glandular histologic types registered had an increased trend over time (p = 0.002), higher for the region of Campinas (21.1% versus 12.5% for the region of Curitiba).
The number, pattern and trends of cervical cancer cases registered had mild and slow modifications and reflect the limited effectivity of the opportunistic screening program, even in developed places.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2018;40(6):347-353
The aim of this study was to assess the time trends and pattern of cervical cancer diagnosed in the period from 2001 to 2012 by means of an opportunistic screening program from two developed regions in Brazil.
An observational study analyzing 3,364 cancer records (n = 1,646 from Campinas and n = 1,718 from Curitiba region) available in hospital-based cancer registries was done. An additional 1,836 records of CIN3/AIS from the region of Campinas was analyzed. The statistical analysis assessed the pooled data and the data by region considering the year of diagnosis, age-group, cancer stage, and histologic type. The Cochran-Armitage trend test was applied and p-values < 0.05 were considered significant.
The total annual cervical cancer registered from2001 to 2012 showed a slight drop (273-244), with an age average of 49.5 y, 13 years over the average for CIN3/AIS (36.8 y). A total of 20.6% of the diagnoses (1.6% under 25 y) were done out of the official screening age-range. The biennial rate of diagnoses by age group for the region of Campinas showed an increase trend for the age groups under 25 y (p = 0.007) and 25 to 44 y (p = 0.003). Stage III was the most recorded for both regions, with an annual average of 43%, without any trend modification. There was an increasing trend for stage I diagnoses in the region of Campinas (p = 0.033). The proportion of glandular histologic types registered had an increased trend over time (p = 0.002), higher for the region of Campinas (21.1% versus 12.5% for the region of Curitiba).
The number, pattern and trends of cervical cancer cases registered had mild and slow modifications and reflect the limited effectivity of the opportunistic screening program, even in developed places.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(1):37-43
DOI 10.1590/S0100-72032002000100006
Purpose: to determine the factors associated with the detection of a microinvasive carcinoma in the cervical cone of women with a previous colposcopically directed biopsy compatible with cervical intraepithelial neoplasia (CIN) 3 and to evaluate the proportion of involved margins. Patients and methods: we reviewed the medical records of 385 women (mean age: 39 years) submitted to cold conization or conization by high frequency surgery (HFS) with a loop during the period from January 1993 to July 2000. These procedures were indicated on the basis of a biopsy compatible with (CIN) 3. Results: the diagnosis of the cone was compatible with (CIN) 3 in 243 (63%) women and with (CIN) 2 in 13 (3%). Only 10 presented HPV/CIN 1 (3%) and eight had no residual disease in the cone. However, 101 (26%) women presented a microinvasive carcinoma in the cone and 10 (3%) presented a frankly invasive carcinoma. Age, menstrual status and number of deliveries were not related to the severity of the cone lesion. Women with oncologic colpocytology changes suggestive of invasion presented a significantly higher risk of having a microinvasive or invasive carcinoma as determined by final histology (p<0.01), although 52 of the 243 women with CIN 2 or CIN 3 in the cone also showed a suggestion of invasion at colpocytology. Among the women with CIN 2 or 3, the epithelium was white in 44%, dotted in 21%, and mosaic-like in 17%. This proportion was similar for women with a microinvasive or invasive carcinoma, with these images being detected in 37%, 23% and 21% of the cases, respectively. Involvement of the cone margins was significantly higher among women submitted to HFS (49%) than among those submitted to cold conization (29%). Conclusion: the absence of independent clinical and colposcopic factors associated with the detection of a microinvasive carcinoma in women submitted to conization on the basis of a biopsy compatible with (CIN) 3 justifies the conical excision of the squamocolumnar junction in high grade cervical lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(1):37-43
DOI 10.1590/S0100-72032002000100006
Purpose: to determine the factors associated with the detection of a microinvasive carcinoma in the cervical cone of women with a previous colposcopically directed biopsy compatible with cervical intraepithelial neoplasia (CIN) 3 and to evaluate the proportion of involved margins. Patients and methods: we reviewed the medical records of 385 women (mean age: 39 years) submitted to cold conization or conization by high frequency surgery (HFS) with a loop during the period from January 1993 to July 2000. These procedures were indicated on the basis of a biopsy compatible with (CIN) 3. Results: the diagnosis of the cone was compatible with (CIN) 3 in 243 (63%) women and with (CIN) 2 in 13 (3%). Only 10 presented HPV/CIN 1 (3%) and eight had no residual disease in the cone. However, 101 (26%) women presented a microinvasive carcinoma in the cone and 10 (3%) presented a frankly invasive carcinoma. Age, menstrual status and number of deliveries were not related to the severity of the cone lesion. Women with oncologic colpocytology changes suggestive of invasion presented a significantly higher risk of having a microinvasive or invasive carcinoma as determined by final histology (p<0.01), although 52 of the 243 women with CIN 2 or CIN 3 in the cone also showed a suggestion of invasion at colpocytology. Among the women with CIN 2 or 3, the epithelium was white in 44%, dotted in 21%, and mosaic-like in 17%. This proportion was similar for women with a microinvasive or invasive carcinoma, with these images being detected in 37%, 23% and 21% of the cases, respectively. Involvement of the cone margins was significantly higher among women submitted to HFS (49%) than among those submitted to cold conization (29%). Conclusion: the absence of independent clinical and colposcopic factors associated with the detection of a microinvasive carcinoma in women submitted to conization on the basis of a biopsy compatible with (CIN) 3 justifies the conical excision of the squamocolumnar junction in high grade cervical lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):408-414
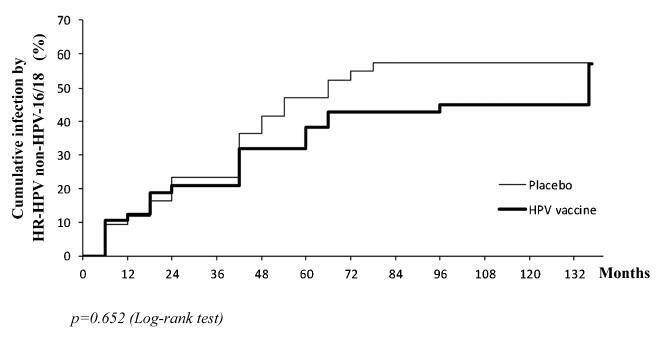
the aim of this study was to evaluate the pattern of human papillomavirus (HPV) detection in an 11.3-year post-vaccination period in a cohort of adolescent and young women vaccinated or not against HPV 16/18.
a subset of 91 women from a single center participating in a randomized clinical trial (2001-2010, NCT00689741/00120848/00518336) with HPV 16/18 AS04- adjuvanted vaccine was evaluated. All women received three doses of the HPV vaccine (n = 48) or a placebo (n = 43), and cervical samples were collected at 6-month intervals. Only in this center, one additional evaluation was performed in 2012. Up to 1,492 cervical samples were tested for HPV-DNA and genotyped with polymerase chain reaction (PCR). The vaccine group characteristics were compared by Chi-square or Fisher exact or Mann-Whitney test. The high-risk (HR)-HPV 6-month-persistent infection rate was calculated. The cumulative infection by HPV group was evaluated by the Kaplan-Meier method and the log-rank test.
the cumulative infection with any type of HPV in an 11.3-year period was 67% in the HPV vaccine group and 72% in the placebo group (p = 0.408). The longitudinal analysis showed an increase of 4% per year at risk for detection of HR-HPV (non-HPV 16/ 18) over time (p = 0.015), unrelated to vaccination. The cumulative infection with HPV 16/18 was 4% for the HPV vaccine group and 29% for the placebo group (p = 0.003). There were 43 episodes of HR-HPV 6-month persistent infection, unrelated to vaccination.
this study showed themaintenance of viral detection rate accumulating HR-HPV (non-HPV-16-18) positive tests during a long period post-vaccination, regardless of prior vaccination. This signalizes that the high number of HPV-positive testsmay be maintained after vaccination.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(8):408-414
the aim of this study was to evaluate the pattern of human papillomavirus (HPV) detection in an 11.3-year post-vaccination period in a cohort of adolescent and young women vaccinated or not against HPV 16/18.
a subset of 91 women from a single center participating in a randomized clinical trial (2001-2010, NCT00689741/00120848/00518336) with HPV 16/18 AS04- adjuvanted vaccine was evaluated. All women received three doses of the HPV vaccine (n = 48) or a placebo (n = 43), and cervical samples were collected at 6-month intervals. Only in this center, one additional evaluation was performed in 2012. Up to 1,492 cervical samples were tested for HPV-DNA and genotyped with polymerase chain reaction (PCR). The vaccine group characteristics were compared by Chi-square or Fisher exact or Mann-Whitney test. The high-risk (HR)-HPV 6-month-persistent infection rate was calculated. The cumulative infection by HPV group was evaluated by the Kaplan-Meier method and the log-rank test.
the cumulative infection with any type of HPV in an 11.3-year period was 67% in the HPV vaccine group and 72% in the placebo group (p = 0.408). The longitudinal analysis showed an increase of 4% per year at risk for detection of HR-HPV (non-HPV 16/ 18) over time (p = 0.015), unrelated to vaccination. The cumulative infection with HPV 16/18 was 4% for the HPV vaccine group and 29% for the placebo group (p = 0.003). There were 43 episodes of HR-HPV 6-month persistent infection, unrelated to vaccination.
this study showed themaintenance of viral detection rate accumulating HR-HPV (non-HPV-16-18) positive tests during a long period post-vaccination, regardless of prior vaccination. This signalizes that the high number of HPV-positive testsmay be maintained after vaccination.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(7):417-418
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2019;41(7):417-418
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(8):431-437
DOI 10.1590/S0100-72031999000800002
Purpose: to evaluate risk factors and papillomavirus (HPV) associated lesions in male partners of women with genital intraepithelial neoplasia. Patients and Methods: three hundred and thirty-seven men were evaluated by urethral cytology, peniscopy, and biopsy, if necessary. We analyzed the results and the relations to age, educational level, smoking, contact time with the present partner, age at first intercourse, number of partners, previous sexually transmitted diseases (STD), circumcision, peniscopic findings, and female lesion grade. Results: peniscopy was positive in 144 (42,7%) and HPV infection was diagnosed in 105 (31,2%). Smoking, contact time with the present partner up to 6 months, and more than one previous sexual partner were associated with HPV lesions (p<0,05). The urethral cytology was suspect in 4,2% and smoking, positive peniscopy or biopsy and partners of women with high-grade lesion (p<0,05) were associated with the diagnosis. 72.1% of 229 biopsies were positive, independently of the peniscopic findings and women's lesion grade. Conclusions: HPV infection was diagnosed in 31.2% and was associated with smoking, contact time with the present partner up to 6 months and more than one previous sexual partner, but not with the female lesion grade, educationa level, previous STD, circumcision and peniscopic findings.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1999;21(8):431-437
DOI 10.1590/S0100-72031999000800002
Purpose: to evaluate risk factors and papillomavirus (HPV) associated lesions in male partners of women with genital intraepithelial neoplasia. Patients and Methods: three hundred and thirty-seven men were evaluated by urethral cytology, peniscopy, and biopsy, if necessary. We analyzed the results and the relations to age, educational level, smoking, contact time with the present partner, age at first intercourse, number of partners, previous sexually transmitted diseases (STD), circumcision, peniscopic findings, and female lesion grade. Results: peniscopy was positive in 144 (42,7%) and HPV infection was diagnosed in 105 (31,2%). Smoking, contact time with the present partner up to 6 months, and more than one previous sexual partner were associated with HPV lesions (p<0,05). The urethral cytology was suspect in 4,2% and smoking, positive peniscopy or biopsy and partners of women with high-grade lesion (p<0,05) were associated with the diagnosis. 72.1% of 229 biopsies were positive, independently of the peniscopic findings and women's lesion grade. Conclusions: HPV infection was diagnosed in 31.2% and was associated with smoking, contact time with the present partner up to 6 months and more than one previous sexual partner, but not with the female lesion grade, educationa level, previous STD, circumcision and peniscopic findings.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):567-572
To compare death rates by COVID-19 between pregnant or postpartum and nonpregnant women during the first and second waves of the Brazilian pandemic.
In the present population-based evaluation data from the Sistema de Informação da Vigilância Epidemiológica da Gripe (SIVEP-Gripe, in the Portuguese acronym), we included women with c (ARDS) by COVID-19: 47,768 in 2020 (4,853 obstetric versus 42,915 nonobstetric) and 66,689 in 2021 (5,208 obstetric versus 61,481 nonobstetric) and estimated the frequency of in-hospital death.
We identified 377 maternal deaths in 2020 (first wave) and 804 in 2021 (second wave). The death rate increased 2.0-fold for the obstetric (7.7 to 15.4%) and 1.6-fold for the nonobstetric groups (13.9 to 22.9%) from 2020 to 2021 (odds ratio [OR]: 0.52; 95% confidence interval [CI]: 0.47–0.58 in 2020 and OR: 0.61; 95%CI: 0.56– 0.66 in 2021; p < 0.05). In women with comorbidities, the death rate increased 1.7-fold (13.3 to 23.3%) and 1.4-fold (22.8 to 31.4%) in the obstetric and nonobstetric groups, respectively (OR: 0.52; 95%CI: 0.44–0.61 in 2020 to OR: 0.66; 95%CI: 0.59–0.73 in 2021; p <0.05). In women without comorbidities, the mortality rate was higher for nonobstetric (2.4 times; 6.6 to 15.7%) than for obstetric women (1.8 times; 5.5 to 10.1%; OR: 0.81; 95%CI: 0.69–0.95 in 2020 and OR: 0.60; 95%CI: 0.58–0.68 in 2021; p <0.05).
There was an increase in maternal deaths from COVID-19 in 2021 compared with 2020, especially in patients with comorbidities. Death rates were even higher in nonpregnant women, with or without comorbidities.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):631-635
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(6):631-635