You searched for:"José Geraldo Lopes Ramos"
We found (17) results for your search.Summary
Rev Bras Ginecol Obstet. 2003;25(6):431-436
DOI 10.1590/S0100-72032003000600008
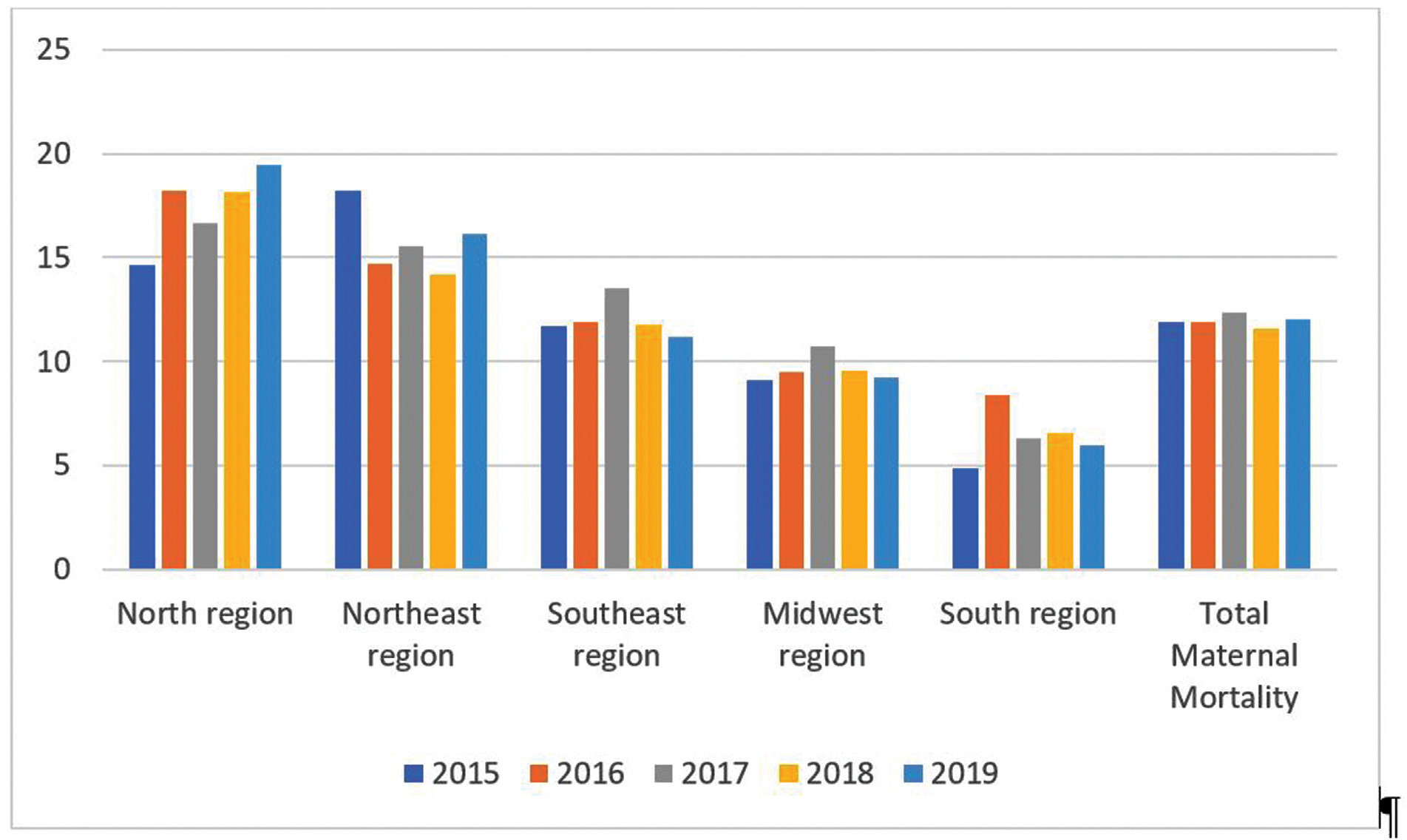
PURPOSE: to analyze maternal death cases that occurred at the "Hospital de Clínicas de Porto Alegre", a reference university hospital for high-risk pregnancies in the state of Rio Grande do Sul, Brazil. METHODS: we carried out a retrospective study of medical records of 10- to 49-year-old women who died at the hospital between 1980 and 1999. Deaths related to pregnancy and puerperium were analyzed independently of the kind and duration of pregnancy. The causes were classified into direct obstetric, indirect obstetric and nonobstetric, according to their association with pregnancy, delivery and puerperium disorders. RESULTS: a total of 81 patients with a mean age of 28.5 years were studied. The maternal mortality rate was 109 per 100,000 live births. Direct obstetric causes made up 61.7% of deaths. Indirect causes made up 23.5% of deaths. Nonobstetric causes made up 15.0% of the total. Among direct obstetric causes, arterial hypertension (18.5%), post-cesarean infection (16%), and septic abortion (12.3%) were the most prevalent. The main maternal mortality events among indirect obstetric causes were cardiopathy (8.6%), acute fatty liver disease (3.5%), and systemic lupus erythematosus (2.5%). Among the nonobstetric causes, malignant neoplasia (7.4%) and AIDS (3.7%) were the most important. CONCLUSIONS: the prevailing causes of maternal death have not changed in the last two decades. The main cause is still hypertension. There is an expressive number of deaths related to cesarean section and infections. The high prevalence of direct obstetric causes shows the low maternal mortality prevention capacity of our health care system.
Summary
Rev Bras Ginecol Obstet. 2003;25(6):431-436
DOI 10.1590/S0100-72032003000600008
PURPOSE: to analyze maternal death cases that occurred at the "Hospital de Clínicas de Porto Alegre", a reference university hospital for high-risk pregnancies in the state of Rio Grande do Sul, Brazil. METHODS: we carried out a retrospective study of medical records of 10- to 49-year-old women who died at the hospital between 1980 and 1999. Deaths related to pregnancy and puerperium were analyzed independently of the kind and duration of pregnancy. The causes were classified into direct obstetric, indirect obstetric and nonobstetric, according to their association with pregnancy, delivery and puerperium disorders. RESULTS: a total of 81 patients with a mean age of 28.5 years were studied. The maternal mortality rate was 109 per 100,000 live births. Direct obstetric causes made up 61.7% of deaths. Indirect causes made up 23.5% of deaths. Nonobstetric causes made up 15.0% of the total. Among direct obstetric causes, arterial hypertension (18.5%), post-cesarean infection (16%), and septic abortion (12.3%) were the most prevalent. The main maternal mortality events among indirect obstetric causes were cardiopathy (8.6%), acute fatty liver disease (3.5%), and systemic lupus erythematosus (2.5%). Among the nonobstetric causes, malignant neoplasia (7.4%) and AIDS (3.7%) were the most important. CONCLUSIONS: the prevailing causes of maternal death have not changed in the last two decades. The main cause is still hypertension. There is an expressive number of deaths related to cesarean section and infections. The high prevalence of direct obstetric causes shows the low maternal mortality prevention capacity of our health care system.
Summary
Rev Bras Ginecol Obstet. 2016;38(9):450-455
To demonstrate the initial experience of robotic hysterectomy to treat benign uterine disease at a university hospital in Brazil.
A cross-sectional study was conducted to review data from the first twenty patients undergoing robotic hysterectomy at our hospital. The surgeries were performed from November 2013 to August 2014, all of them by the same surgeon. The patients were reviewed for preoperative characteristics, including age, body mass index (BMI), indications for the hysterectomy and previous surgeries. Data of operative times, complications, postoperative pain and length of hospital stay were also collected.
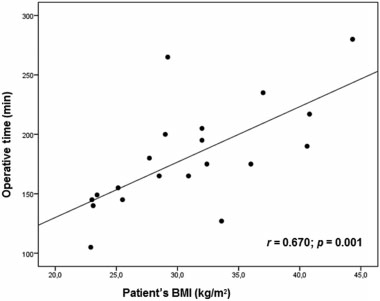
The total operating room time was 252.9 minutes, while the operative time was 180.7 minutes and the console time was 136.6 minutes. Docking time was 4.2 minutes, and the average undocking time was 1.9 minutes. There was a strong correlation between the operative time and the patient's BMI (r = 0.670 ; p = 0.001). The console time had significant correlation with the uterine weight and the patient's BMI (r = 0.468; p = 0.037). A learning curve was observed during docking and undocking times.
Despite its high cost, the robotic surgery is gaining more space in gynecological surgery. By the results obtained in our hospital, this surgical proposal proved to be feasible and safe. Our initial experience demonstrated a learning curve in some ways.
Summary
Rev Bras Ginecol Obstet. 2016;38(9):450-455
To demonstrate the initial experience of robotic hysterectomy to treat benign uterine disease at a university hospital in Brazil.
A cross-sectional study was conducted to review data from the first twenty patients undergoing robotic hysterectomy at our hospital. The surgeries were performed from November 2013 to August 2014, all of them by the same surgeon. The patients were reviewed for preoperative characteristics, including age, body mass index (BMI), indications for the hysterectomy and previous surgeries. Data of operative times, complications, postoperative pain and length of hospital stay were also collected.
The total operating room time was 252.9 minutes, while the operative time was 180.7 minutes and the console time was 136.6 minutes. Docking time was 4.2 minutes, and the average undocking time was 1.9 minutes. There was a strong correlation between the operative time and the patient's BMI (r = 0.670 ; p = 0.001). The console time had significant correlation with the uterine weight and the patient's BMI (r = 0.468; p = 0.037). A learning curve was observed during docking and undocking times.
Despite its high cost, the robotic surgery is gaining more space in gynecological surgery. By the results obtained in our hospital, this surgical proposal proved to be feasible and safe. Our initial experience demonstrated a learning curve in some ways.
Summary
Rev Bras Ginecol Obstet. 2017;39(9):496-512
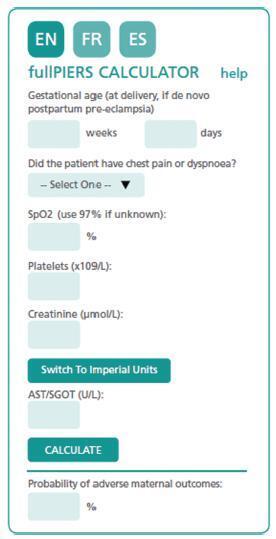
The authors review hypertensive disease during pregnancy with an academic and practical view, and using the best evidence available. This disease, which is the most important clinical disease in Brazilian pregnant women, may have its incidence reduced with prevention through the use of calcium and aspirin in pregnant women at risk. Previously, it was a disease that presented with hypertension with proteinuria, but it has now been classified with new clinical parameters besides proteinuria. Morbidity and mortality should be reduced in a continental country such as Brazil using protocols for the early treatment of complications by calculating severe outcomes in preeclampsia. The early treatment of acute hypertension, use of magnesium sulfate and early hospitalization in cases of preeclampsia are concepts to pursue the reduction of our pregnant women’s mortality.
Summary
Rev Bras Ginecol Obstet. 2017;39(9):496-512
The authors review hypertensive disease during pregnancy with an academic and practical view, and using the best evidence available. This disease, which is the most important clinical disease in Brazilian pregnant women, may have its incidence reduced with prevention through the use of calcium and aspirin in pregnant women at risk. Previously, it was a disease that presented with hypertension with proteinuria, but it has now been classified with new clinical parameters besides proteinuria. Morbidity and mortality should be reduced in a continental country such as Brazil using protocols for the early treatment of complications by calculating severe outcomes in preeclampsia. The early treatment of acute hypertension, use of magnesium sulfate and early hospitalization in cases of preeclampsia are concepts to pursue the reduction of our pregnant women’s mortality.
Summary
Rev Bras Ginecol Obstet. 2006;28(9):513-522
DOI 10.1590/S0100-72032006000900003
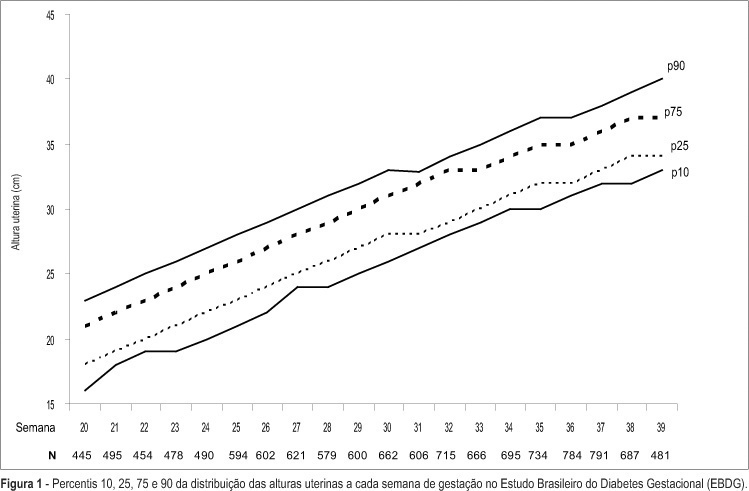
PURPOSE: to describe, in participants of the Brazilian Study of Gestational Diabetes (EBDG), the percentile distribution of uterine height by gestational age and to validate the use of percentiles of the chart derived by the "Centro Latino-Americano de Perinatologia" (CLAP), used as reference in predicting abnormal fetal growth. METHODS: the EBDG is a cohort study of 5564 pregnant women older than 19 years, followed through and after delivery. Interviews and standardized anthropometry were performed at baseline between 20-28 weeks. Medical records covering prenatal and delivery periods were then reviewed following a standardized approach. Analyses pertain to 3539 women with gestational age confirmed by ultrasound. Diagnostic properties of the 10th and the 90th percentiles of both charts (EBDG and CLAP) as predictors of abnormal neonatal weight were determined. RESULTS: uterine height was higher in EBDG than in the CLAP chart at every gestational week, being 1-4 and 2-6 cm greater, at the 10th and 90th percentiles respectively. The CLAP 10th percentile classified as small the uterine heights of only 0.3 to 1.7% of Brazilian women, while the 90th percentile classified as large the uterine heights of 42 to 57% of the sample. The sensitivity of CLAP percentile 10 in the prediction of small for gestational age varied from 0.8 to 6% and the specificity of CLAP percentile 90 in the prediction of large for gestational age, from 46 to 61%. CONCLUSIONS: the CLAP uterine height reference chart does not reflect the current uterine growth pattern of pregnant Brazilians, limiting its clinical applicability in the detection of abnormal fetal growth, especially intrauterine growth restriction.
Summary
Rev Bras Ginecol Obstet. 2006;28(9):513-522
DOI 10.1590/S0100-72032006000900003
PURPOSE: to describe, in participants of the Brazilian Study of Gestational Diabetes (EBDG), the percentile distribution of uterine height by gestational age and to validate the use of percentiles of the chart derived by the "Centro Latino-Americano de Perinatologia" (CLAP), used as reference in predicting abnormal fetal growth. METHODS: the EBDG is a cohort study of 5564 pregnant women older than 19 years, followed through and after delivery. Interviews and standardized anthropometry were performed at baseline between 20-28 weeks. Medical records covering prenatal and delivery periods were then reviewed following a standardized approach. Analyses pertain to 3539 women with gestational age confirmed by ultrasound. Diagnostic properties of the 10th and the 90th percentiles of both charts (EBDG and CLAP) as predictors of abnormal neonatal weight were determined. RESULTS: uterine height was higher in EBDG than in the CLAP chart at every gestational week, being 1-4 and 2-6 cm greater, at the 10th and 90th percentiles respectively. The CLAP 10th percentile classified as small the uterine heights of only 0.3 to 1.7% of Brazilian women, while the 90th percentile classified as large the uterine heights of 42 to 57% of the sample. The sensitivity of CLAP percentile 10 in the prediction of small for gestational age varied from 0.8 to 6% and the specificity of CLAP percentile 90 in the prediction of large for gestational age, from 46 to 61%. CONCLUSIONS: the CLAP uterine height reference chart does not reflect the current uterine growth pattern of pregnant Brazilians, limiting its clinical applicability in the detection of abnormal fetal growth, especially intrauterine growth restriction.
Summary
Rev Bras Ginecol Obstet. 2002;24(8):555-559
DOI 10.1590/S0100-72032002000800009
The hemolytic - uremic syndrome (HUS) presents with a triad of acute renal failure, microangiopathic hemolytic anemia and thrombocytopenia associated with high morbidity and mortality. On the differential diagnosis, other entities must be considered like preeclampsia, HELLP syndrome, acute fatty liver of pregnancy and thrombotic thrombocytopenic purpura. We report a case of HUS occurring in the immediate postpartum period in a patient initially diagnosed as having preeclampsia. The differential diagnosis was based on abrupt renal failure, blood pressure increase and clinical and laboratorial evidence of hemolysis. Attention is directed to investigation, clinical management and prognosis based on review of the literature.
Summary
Rev Bras Ginecol Obstet. 2002;24(8):555-559
DOI 10.1590/S0100-72032002000800009
The hemolytic - uremic syndrome (HUS) presents with a triad of acute renal failure, microangiopathic hemolytic anemia and thrombocytopenia associated with high morbidity and mortality. On the differential diagnosis, other entities must be considered like preeclampsia, HELLP syndrome, acute fatty liver of pregnancy and thrombotic thrombocytopenic purpura. We report a case of HUS occurring in the immediate postpartum period in a patient initially diagnosed as having preeclampsia. The differential diagnosis was based on abrupt renal failure, blood pressure increase and clinical and laboratorial evidence of hemolysis. Attention is directed to investigation, clinical management and prognosis based on review of the literature.
Summary
Rev Bras Ginecol Obstet. 2022;44(7):637-639
Summary
Rev Bras Ginecol Obstet. 2022;44(7):637-639