You searched for:"Francisco José Candido dos Reis"
We found (23) results for your search.Summary
Rev Bras Ginecol Obstet. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
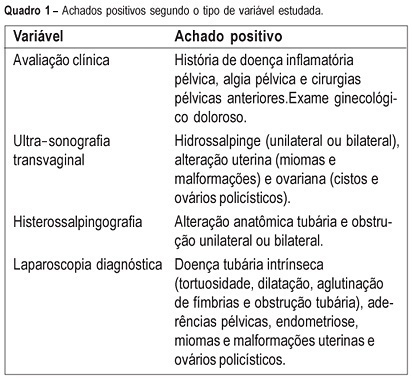
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Rev Bras Ginecol Obstet. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Rev Bras Ginecol Obstet. 2020;42(7):411-414
Summary
Rev Bras Ginecol Obstet. 2020;42(7):411-414
Summary
Rev Bras Ginecol Obstet. 1999;21(7):415-418
DOI 10.1590/S0100-72031999000700008
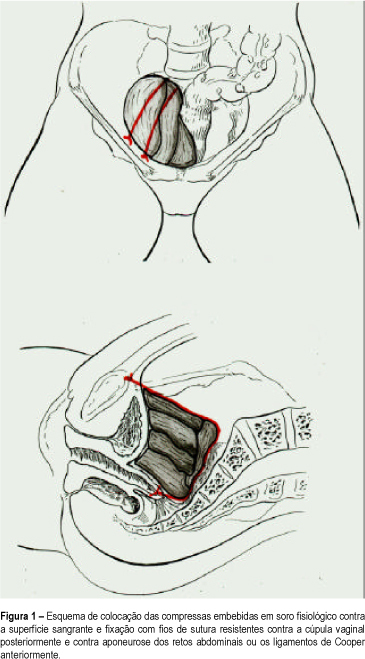
Purpose: to introduce the use of the hemostatic pack, a tampon consisting of compresses tied to the bleeding surface and left in place for 48 to 72 h and which is one of the therapeutic alternatives to be used in this situation. Patients and Methods: we evaluated 3 cases of massive bleeding during surgery, with the exchange, on average, of 1.4 blood volumes (1.2-2.4), in terms of hemostatic effectiveness of the pack and of some patient parameters such as age and amount and type of volume infused. Results: the mean age of the patients was 57 years (51, 56 and 64). Only one had been previously irradiated. The bleeding was of venous origin, from the fossa of the obturator nerve, the iliac plexus and the presacral plexus. The volume expander most often used was 0.9% physiological saline solution, followed by blood derivatives and by Ringer lactate. Two patients were submitted to ligation of the hypogastric vein during surgery, with no improvement. The use of hemostatic synthetic material was inefficient in all three cases. In one of the patients, the use of nonabsorbable sutures to close the bleeding area led to a considerable reduction of bleeding, but did not eliminate it completely. One patient died before 24 h had elapsed, with signs and symptoms of heart failure. The other two patients developed acute renal failure and one of them developed aspirative pneumonia during surgical reexploration. Conclusion: massive bleeding is related to high morbidity and mortality. Among the emergency measures used for hemostasis, the pack seems to be the most adequate.
Summary
Rev Bras Ginecol Obstet. 1999;21(7):415-418
DOI 10.1590/S0100-72031999000700008
Purpose: to introduce the use of the hemostatic pack, a tampon consisting of compresses tied to the bleeding surface and left in place for 48 to 72 h and which is one of the therapeutic alternatives to be used in this situation. Patients and Methods: we evaluated 3 cases of massive bleeding during surgery, with the exchange, on average, of 1.4 blood volumes (1.2-2.4), in terms of hemostatic effectiveness of the pack and of some patient parameters such as age and amount and type of volume infused. Results: the mean age of the patients was 57 years (51, 56 and 64). Only one had been previously irradiated. The bleeding was of venous origin, from the fossa of the obturator nerve, the iliac plexus and the presacral plexus. The volume expander most often used was 0.9% physiological saline solution, followed by blood derivatives and by Ringer lactate. Two patients were submitted to ligation of the hypogastric vein during surgery, with no improvement. The use of hemostatic synthetic material was inefficient in all three cases. In one of the patients, the use of nonabsorbable sutures to close the bleeding area led to a considerable reduction of bleeding, but did not eliminate it completely. One patient died before 24 h had elapsed, with signs and symptoms of heart failure. The other two patients developed acute renal failure and one of them developed aspirative pneumonia during surgical reexploration. Conclusion: massive bleeding is related to high morbidity and mortality. Among the emergency measures used for hemostasis, the pack seems to be the most adequate.
Summary
Rev Bras Ginecol Obstet. 2009;31(9):425-426
Summary
Rev Bras Ginecol Obstet. 2009;31(9):425-426
Summary
Rev Bras Ginecol Obstet. 1999;21(1):47-54
DOI 10.1590/S0100-72031999000100008
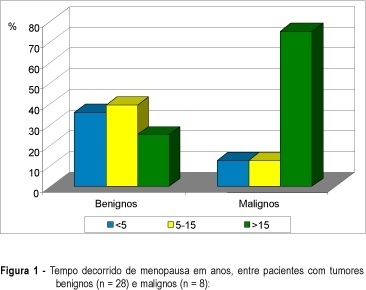
Purpose: to evaluate clinical and ultrasonic findings in patients with pelvic tumors at postmenopause and to correlate them with the final diagnosis. Patients and Methods: thirty-six postmenopausal women with pelvic tumor diagnosis were prospectively evaluated through clinical examination and endovaginal ultrasonography. Clinical follow-up with no surgical procedures was indicated for anechoic cystic tumors with or without thin unique septation and volume under 50 cm³. Needle aspiration was indicated for tumors with the same aspect, and volume of 50 to 100 cm³, whereas exploratory laparotomy was performed in the remaining patients. Diagnosis defined two groups of patients: benign (28) and malignant (8) pathologies. Results: anechoic cystic tumor with or without a thin septum indicates benignity (p = 0.0091). Tumors with solid areas indicate malignancy (p = 0.0024). Ascites correlates with malignancy (p = 0.0278). Heterogeneity, thick capsule, thick septa, and papillary projections predominated in malignancies but without no statistical significance (p > 0,05). Tumor volume indicates malignancy, with a median of 85.2 cm³ in benign tumors and 452.5 cm³ in malignancies (p = 0.0048), with a cutoff at 295 cm³ (sensitivity = 83.3% and specificity = 85.2%). Following this protocol, all malignancies were submitted to surgery and 11 benign tumor patients were treated with a conservative protocol (39.3% of all benign patients). Conclusion: conservative management is an adequate protocol for women with anechoic pelvic tumors with low volume, with or without single thin septum and without ascites. Differentiation between benign and malignant of complex and/or high volume tumors requires complementary investigation.
Summary
Rev Bras Ginecol Obstet. 1999;21(1):47-54
DOI 10.1590/S0100-72031999000100008
Purpose: to evaluate clinical and ultrasonic findings in patients with pelvic tumors at postmenopause and to correlate them with the final diagnosis. Patients and Methods: thirty-six postmenopausal women with pelvic tumor diagnosis were prospectively evaluated through clinical examination and endovaginal ultrasonography. Clinical follow-up with no surgical procedures was indicated for anechoic cystic tumors with or without thin unique septation and volume under 50 cm³. Needle aspiration was indicated for tumors with the same aspect, and volume of 50 to 100 cm³, whereas exploratory laparotomy was performed in the remaining patients. Diagnosis defined two groups of patients: benign (28) and malignant (8) pathologies. Results: anechoic cystic tumor with or without a thin septum indicates benignity (p = 0.0091). Tumors with solid areas indicate malignancy (p = 0.0024). Ascites correlates with malignancy (p = 0.0278). Heterogeneity, thick capsule, thick septa, and papillary projections predominated in malignancies but without no statistical significance (p > 0,05). Tumor volume indicates malignancy, with a median of 85.2 cm³ in benign tumors and 452.5 cm³ in malignancies (p = 0.0048), with a cutoff at 295 cm³ (sensitivity = 83.3% and specificity = 85.2%). Following this protocol, all malignancies were submitted to surgery and 11 benign tumor patients were treated with a conservative protocol (39.3% of all benign patients). Conclusion: conservative management is an adequate protocol for women with anechoic pelvic tumors with low volume, with or without single thin septum and without ascites. Differentiation between benign and malignant of complex and/or high volume tumors requires complementary investigation.
Summary
Rev Bras Ginecol Obstet. 2016;38(1):47-52
Patient autonomy has great importance for a valid informed consent in clinical practice. Our objectives were to quantify thedomains of patient autonomy and to evaluate the variables that can affect patient autonomy in women with chronic pelvic pain.
This study is a cross sectional survey performed in a tertiary care University Hospital. Fifty-two consecutive women scheduled for laparoscopic management of chronic pelvic were included. Three major components of autonomy (competence, information or freedom) were evaluated using a Likert scale with 24 validated affirmatives.
Competence scores (0.85 vs 0.92; p = 0.006) and information scores (0.90 vs 0.93; p = 0.02) were low for women with less than eight years of school attendance. Information scores were low in the presence of anxiety (0.91 vs 0.93; p = 0.05) or depression (0.90 vs 0.93; p = 0.01).
Our data show that systematic evaluation of patient autonomy can provide clinical relevant information in gynecology. Low educational level, anxiety and depression might reduce the patient autonomy in women with chronic pelvic pain.
Summary
Rev Bras Ginecol Obstet. 2016;38(1):47-52
Patient autonomy has great importance for a valid informed consent in clinical practice. Our objectives were to quantify thedomains of patient autonomy and to evaluate the variables that can affect patient autonomy in women with chronic pelvic pain.
This study is a cross sectional survey performed in a tertiary care University Hospital. Fifty-two consecutive women scheduled for laparoscopic management of chronic pelvic were included. Three major components of autonomy (competence, information or freedom) were evaluated using a Likert scale with 24 validated affirmatives.
Competence scores (0.85 vs 0.92; p = 0.006) and information scores (0.90 vs 0.93; p = 0.02) were low for women with less than eight years of school attendance. Information scores were low in the presence of anxiety (0.91 vs 0.93; p = 0.05) or depression (0.90 vs 0.93; p = 0.01).
Our data show that systematic evaluation of patient autonomy can provide clinical relevant information in gynecology. Low educational level, anxiety and depression might reduce the patient autonomy in women with chronic pelvic pain.
Summary
Rev Bras Ginecol Obstet. 2020;42(8):486-492
To determine the average body composition (percentage of body fat), the anthropometric markers, and the intensity of clinical pain in women with a clinical diagnosis of chronic pelvic pain (CPP) secondary to endometriosis.
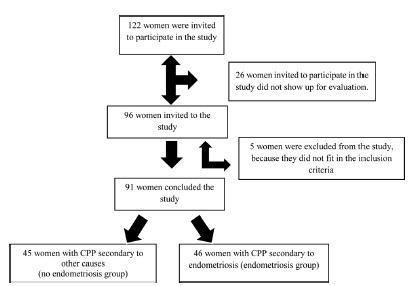
A case-control study performed with 91 women, 46 of whom with CPP secondary to endometriosis and 45 of whom with CPP secondary to other causes. They underwent an evaluation of the anthropometric parameters by means of the body mass index (BMI), the perimeters (waist, abdomen, hip), and the percentage of body fat (%BF), which were assessed on a body composition monitor by bioimpedance; the intensity of the clinical pain was evaluated using the visual analog scale (VAS), and the symptoms of anxiety and depression, using the hospital’s anxiety and depression scale (HAD).
The groups did not differ in terms of mean age, BMI, %BF or regarding the available waist-to-hip ratio (WHR). The mean intensity of the clinical pain by the VAS was of 7.2 ± 2.06 in the group with CPP secondary to endometriosis, and of 5.93 ± 2.64 in the group with CPP secondary to other causes (p = 0.03), revealing significant differences between the groups.
We concluded that, despite the difference in the pain score assessed between the two groups, there was no difference regarding body composition and anthropometry.
Summary
Rev Bras Ginecol Obstet. 2020;42(8):486-492
To determine the average body composition (percentage of body fat), the anthropometric markers, and the intensity of clinical pain in women with a clinical diagnosis of chronic pelvic pain (CPP) secondary to endometriosis.
A case-control study performed with 91 women, 46 of whom with CPP secondary to endometriosis and 45 of whom with CPP secondary to other causes. They underwent an evaluation of the anthropometric parameters by means of the body mass index (BMI), the perimeters (waist, abdomen, hip), and the percentage of body fat (%BF), which were assessed on a body composition monitor by bioimpedance; the intensity of the clinical pain was evaluated using the visual analog scale (VAS), and the symptoms of anxiety and depression, using the hospital’s anxiety and depression scale (HAD).
The groups did not differ in terms of mean age, BMI, %BF or regarding the available waist-to-hip ratio (WHR). The mean intensity of the clinical pain by the VAS was of 7.2 ± 2.06 in the group with CPP secondary to endometriosis, and of 5.93 ± 2.64 in the group with CPP secondary to other causes (p = 0.03), revealing significant differences between the groups.
We concluded that, despite the difference in the pain score assessed between the two groups, there was no difference regarding body composition and anthropometry.
Summary
Rev Bras Ginecol Obstet. 1999;21(9):549-552
DOI 10.1590/S0100-72031999000900008
Purpose: to evaluate the correlation between clinical and surgical staging of patients with vulvar carcinoma, according to the "Federação Internacional de Ginecologia e Obstetrícia" (FIGO 95). Methods: the authors studied 66 consecutive cases of vulvar carcinoma from 1977 to 1997. All patients were clinically staged to verify size and localization of the lesion as well as inguinal lymph node involvement and invasion of other organs. Forty-four patients were submitted to surgical treatment and 34 could be staged according to FIGO 95. Results: among the 34 patients staged through surgery, 17 (50%) showed agreement between clinical and surgical staging. Thus, in 17 patients the staging was different and in these the surgical staging was higher than the clinical in 13 cases and lower in 4 cases. We found in the clinical staging I, 2 cases that were surgical stage II and 1 case that was surgical stage III. Conclusion: the surgical staging could detect lymph node metastasis in patients with clinically negative nodes, as well as exclude false-positive cases. The clinical staging was not accurate for patients with vulvar carcinoma.
Summary
Rev Bras Ginecol Obstet. 1999;21(9):549-552
DOI 10.1590/S0100-72031999000900008
Purpose: to evaluate the correlation between clinical and surgical staging of patients with vulvar carcinoma, according to the "Federação Internacional de Ginecologia e Obstetrícia" (FIGO 95). Methods: the authors studied 66 consecutive cases of vulvar carcinoma from 1977 to 1997. All patients were clinically staged to verify size and localization of the lesion as well as inguinal lymph node involvement and invasion of other organs. Forty-four patients were submitted to surgical treatment and 34 could be staged according to FIGO 95. Results: among the 34 patients staged through surgery, 17 (50%) showed agreement between clinical and surgical staging. Thus, in 17 patients the staging was different and in these the surgical staging was higher than the clinical in 13 cases and lower in 4 cases. We found in the clinical staging I, 2 cases that were surgical stage II and 1 case that was surgical stage III. Conclusion: the surgical staging could detect lymph node metastasis in patients with clinically negative nodes, as well as exclude false-positive cases. The clinical staging was not accurate for patients with vulvar carcinoma.