You searched for:"Francisco Edson de Lucena Feitosa"
We found (18) results for your search.Summary
Rev Bras Ginecol Obstet. 2010;32(8):412-412
Summary
Rev Bras Ginecol Obstet. 2010;32(8):412-412
Summary
Rev Bras Ginecol Obstet. 2006;28(7):431-431
Summary
Rev Bras Ginecol Obstet. 2006;28(7):431-431
Summary
Rev Bras Ginecol Obstet. 2009;31(10):480-484
DOI 10.1590/S0100-72032009001000002
PURPOSE: to evaluate epidemiological aspects in recurrent adolescence pregnancy. METHODS: cohort study including 187 pregnant adolescents attended and followed-up for five years after delivery in an adolescent's attendance service in Ceará state. Age group, being or not at school, living with parents, schooling, marital status and the present partner's condition were analyzed. Data were processed by the EPI-INFO program. Statistical analysis of the independent variables (age, schooling, being at school, having a job, living with parents, marital status and switching partners) was done and compared to the dependent variable (being or not pregnant after five years). The Fisher's exact test was used to evaluate the association among factors which could influence the pregnancy recurrence, the association being present when p<0.05. Risks related to schooling, marital status and multiple partners have been calculated, since these were significant factors for pregnancy recurrence. RESULTS: 61% of the adolescents got pregnant in the five years after the first delivery. Factors such as age, school, work or living with parents were not protective. Nevertheless, when the adolescents had eight or less years of schooling, the risk of getting pregnant has almost duplicated (relative risk (RR)=1.8 (CI95%=1.3-2.6)). New pregnancies were more frequent among the single adolescents without a stable partner (RR=1.3 (CI95%=1.1-1.6) and among the ones who had multiple partners (RR=1.4 (CI95%=1.1-1.7)). CONCLUSIONS: low schooling, multiple partners and non-stable bonds were risk factors for pregnancy recurrence.
Summary
Rev Bras Ginecol Obstet. 2009;31(10):480-484
DOI 10.1590/S0100-72032009001000002
PURPOSE: to evaluate epidemiological aspects in recurrent adolescence pregnancy. METHODS: cohort study including 187 pregnant adolescents attended and followed-up for five years after delivery in an adolescent's attendance service in Ceará state. Age group, being or not at school, living with parents, schooling, marital status and the present partner's condition were analyzed. Data were processed by the EPI-INFO program. Statistical analysis of the independent variables (age, schooling, being at school, having a job, living with parents, marital status and switching partners) was done and compared to the dependent variable (being or not pregnant after five years). The Fisher's exact test was used to evaluate the association among factors which could influence the pregnancy recurrence, the association being present when p<0.05. Risks related to schooling, marital status and multiple partners have been calculated, since these were significant factors for pregnancy recurrence. RESULTS: 61% of the adolescents got pregnant in the five years after the first delivery. Factors such as age, school, work or living with parents were not protective. Nevertheless, when the adolescents had eight or less years of schooling, the risk of getting pregnant has almost duplicated (relative risk (RR)=1.8 (CI95%=1.3-2.6)). New pregnancies were more frequent among the single adolescents without a stable partner (RR=1.3 (CI95%=1.1-1.6) and among the ones who had multiple partners (RR=1.4 (CI95%=1.1-1.7)). CONCLUSIONS: low schooling, multiple partners and non-stable bonds were risk factors for pregnancy recurrence.
Summary
Rev Bras Ginecol Obstet. 1998;20(8):481-484
DOI 10.1590/S0100-72031998000800009
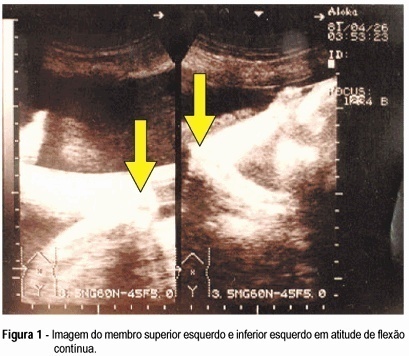
Arthrogryposis multiplex congenita is characterized by multiple joint contractures present at birth. Prenatal diagnosis is difficult. There are few reports in the literature. Fetal akinesia, abnormal limb position, intrauterine growth retardation, and polyhydramnios are the main findings of the ultrasonographic diagnosis. The authors describe a case of arthrogryposis multiplex congenita ultrasonographically diagnosed in the third gestational trimester. The main findings were absence of fetal movements, polyhydramnios, symmetrical and non-symmetrical fetal growth retardation with marked decrease of abdominal and thoracic circumference, low-set ears, micrognathia, continuous flexure contracture of limbs, internal rotation of the femur, and clubfoot on the right.
Summary
Rev Bras Ginecol Obstet. 1998;20(8):481-484
DOI 10.1590/S0100-72031998000800009
Arthrogryposis multiplex congenita is characterized by multiple joint contractures present at birth. Prenatal diagnosis is difficult. There are few reports in the literature. Fetal akinesia, abnormal limb position, intrauterine growth retardation, and polyhydramnios are the main findings of the ultrasonographic diagnosis. The authors describe a case of arthrogryposis multiplex congenita ultrasonographically diagnosed in the third gestational trimester. The main findings were absence of fetal movements, polyhydramnios, symmetrical and non-symmetrical fetal growth retardation with marked decrease of abdominal and thoracic circumference, low-set ears, micrognathia, continuous flexure contracture of limbs, internal rotation of the femur, and clubfoot on the right.
Summary
Rev Bras Ginecol Obstet. 2003;25(7):491-499
DOI 10.1590/S0100-72032003000700005
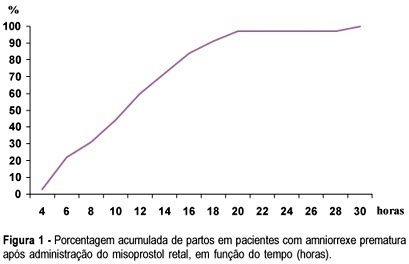
PURPOSE: to investigate whether rectally administered misoprostol is an effective method for induction of labor in patients with premature ruptured membranes at term. METHODS: a pilot trial was conducted, enrolling 32 women with alive, singleton, cephalic fetus and ruptured membranes between 36 and 41 weeks of pregnancy, with Bishop score <6 and without evidence of labor. They received rectal misoprostol (tablets of 50 mg) every 4 h until active labor was diagnosed. Patients with ruptured membranes for >18 h received antibiotics (crystalline penicillin) for prophylaxis of streptococcal infeccion. Outcomes included time from induction to labor and induction to delivery, incidence of tachysystole, mode of delivery, incidence of chorioamnionitis and neonatal outcome. Statistical analysis was performed using the public domain software Epi-Info 2002. Means and standard deviations were calculated, as well as frequency distributions. Survival analysis was performed to determine percent of deliveries according to time (hours) since the administration of the first tablet. RESULTS: the mean (±SD) induction-to-labor and induction-to-delivery intervals were 299.8±199.9 and 681±340.5 min, respectively. The frequency of tachysystole was 9.4%. About 72% of patients achieved vaginal delivery. Chorioamnionitis was diagnosed in 12.5% of the patients. Median Apgar scores at 1st and 5th min were 8 and 9, respectively. There was no case of Apgar <7 at the 5th min. Neonatal sepsis occurred in 12.5% of the neonates. CONCLUSION: induction of labor with rectal misoprostol in the setting of premature rupture of membranes was effective, with 72% of vaginal deliveries and a low rate of chorioamnionitis. These findings must be confirmed by large randomized controlled trials.
Summary
Rev Bras Ginecol Obstet. 2003;25(7):491-499
DOI 10.1590/S0100-72032003000700005
PURPOSE: to investigate whether rectally administered misoprostol is an effective method for induction of labor in patients with premature ruptured membranes at term. METHODS: a pilot trial was conducted, enrolling 32 women with alive, singleton, cephalic fetus and ruptured membranes between 36 and 41 weeks of pregnancy, with Bishop score <6 and without evidence of labor. They received rectal misoprostol (tablets of 50 mg) every 4 h until active labor was diagnosed. Patients with ruptured membranes for >18 h received antibiotics (crystalline penicillin) for prophylaxis of streptococcal infeccion. Outcomes included time from induction to labor and induction to delivery, incidence of tachysystole, mode of delivery, incidence of chorioamnionitis and neonatal outcome. Statistical analysis was performed using the public domain software Epi-Info 2002. Means and standard deviations were calculated, as well as frequency distributions. Survival analysis was performed to determine percent of deliveries according to time (hours) since the administration of the first tablet. RESULTS: the mean (±SD) induction-to-labor and induction-to-delivery intervals were 299.8±199.9 and 681±340.5 min, respectively. The frequency of tachysystole was 9.4%. About 72% of patients achieved vaginal delivery. Chorioamnionitis was diagnosed in 12.5% of the patients. Median Apgar scores at 1st and 5th min were 8 and 9, respectively. There was no case of Apgar <7 at the 5th min. Neonatal sepsis occurred in 12.5% of the neonates. CONCLUSION: induction of labor with rectal misoprostol in the setting of premature rupture of membranes was effective, with 72% of vaginal deliveries and a low rate of chorioamnionitis. These findings must be confirmed by large randomized controlled trials.
Summary
Rev Bras Ginecol Obstet. 2005;27(8):493-500
DOI 10.1590/S0100-72032005000800010
The interest of modern obstetrics in labor induction can be demonstrated by the huge amount of scientific articles published during the last few years. The advances of medicine in general and particularly of obstetrics allowed that more risky pregnancies reach term or near term, with a maternal or fetal indication for pregnancy interruption before the spontaneous onset of labor and delivery. This leads the obstetrician to the situation of choosing between cesarean section and labor induction. With the aim of helping the obstetrician to make the choice for labor induction and thus collaborate with the reduction in cesarean section rates, it is necessary that an accessible, cheap, safe, effective, easy to be used method with good acceptability is available. Although several methods of labor induction reported in medical literature do exist, it is known that there is no ideal method. However, among them, two are highlighted. The first is oxytocin, which has the advantages of promoting physiologic uterine contractions of labor and reverting uterine hypercontractility when suspended. The other method is misoprostol, nowadays the most used, which ripens the uterine cervix and induces uterine contractions of labor. However, there are still some controversies regarding its ideal dose, route and safety.
Summary
Rev Bras Ginecol Obstet. 2005;27(8):493-500
DOI 10.1590/S0100-72032005000800010
The interest of modern obstetrics in labor induction can be demonstrated by the huge amount of scientific articles published during the last few years. The advances of medicine in general and particularly of obstetrics allowed that more risky pregnancies reach term or near term, with a maternal or fetal indication for pregnancy interruption before the spontaneous onset of labor and delivery. This leads the obstetrician to the situation of choosing between cesarean section and labor induction. With the aim of helping the obstetrician to make the choice for labor induction and thus collaborate with the reduction in cesarean section rates, it is necessary that an accessible, cheap, safe, effective, easy to be used method with good acceptability is available. Although several methods of labor induction reported in medical literature do exist, it is known that there is no ideal method. However, among them, two are highlighted. The first is oxytocin, which has the advantages of promoting physiologic uterine contractions of labor and reverting uterine hypercontractility when suspended. The other method is misoprostol, nowadays the most used, which ripens the uterine cervix and induces uterine contractions of labor. However, there are still some controversies regarding its ideal dose, route and safety.
Summary
Rev Bras Ginecol Obstet. 2017;39(2):53-59
To evaluate blood loss during misoprostol-induced vaginal births and during cesarean sections after attempted misoprostol induction.
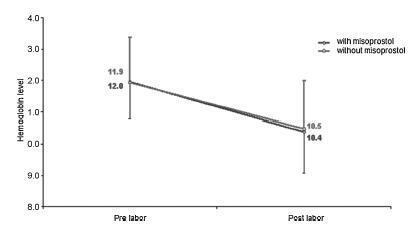
We conducted a prospective observational study in 101 pregnant women indicated for labor induction; pre- and postpartum hemoglobin levels were measured to estimate blood loss during delivery. Labor was induced by administering 25 μg vaginal misoprostol every 6 hours (with a maximum of 6 doses). The control group included 30 patients who spontaneously entered labor, and 30 patients who underwent elective cesarean section. Pre- and postpartum hemoglobin levels were evaluated using the analysis of variance for repeated measurements, showing the effects of time (pre- and postpartum) and of the group (with and withoutmisoprostol administration).
Therewere significant differences between pre- and postpartum hemoglobin levels (p < 0.0001) with regard to misoprostol-induced vaginal deliveries (1.6 ± 1.4 mg/dL), non-induced vaginal deliveries (1.4 ± 1.0 mg/dL), cesarean sections after attempted misoprostol induction (1.5 ± 1.0 mg/dL), and elective cesarean deliveries (1.8 ± 1.1 mg/dL). However, the differences were proportional between the groups with and without misoprostol administration, for both cesarean (p = 0.6845) and vaginal deliveries (p = 0.2694).
Labor induction using misoprostol did not affect blood loss during delivery.
Summary
Rev Bras Ginecol Obstet. 2017;39(2):53-59
To evaluate blood loss during misoprostol-induced vaginal births and during cesarean sections after attempted misoprostol induction.
We conducted a prospective observational study in 101 pregnant women indicated for labor induction; pre- and postpartum hemoglobin levels were measured to estimate blood loss during delivery. Labor was induced by administering 25 μg vaginal misoprostol every 6 hours (with a maximum of 6 doses). The control group included 30 patients who spontaneously entered labor, and 30 patients who underwent elective cesarean section. Pre- and postpartum hemoglobin levels were evaluated using the analysis of variance for repeated measurements, showing the effects of time (pre- and postpartum) and of the group (with and withoutmisoprostol administration).
Therewere significant differences between pre- and postpartum hemoglobin levels (p < 0.0001) with regard to misoprostol-induced vaginal deliveries (1.6 ± 1.4 mg/dL), non-induced vaginal deliveries (1.4 ± 1.0 mg/dL), cesarean sections after attempted misoprostol induction (1.5 ± 1.0 mg/dL), and elective cesarean deliveries (1.8 ± 1.1 mg/dL). However, the differences were proportional between the groups with and without misoprostol administration, for both cesarean (p = 0.6845) and vaginal deliveries (p = 0.2694).
Labor induction using misoprostol did not affect blood loss during delivery.
Summary
Rev Bras Ginecol Obstet. 2006;28(9):566-566
Summary
Rev Bras Ginecol Obstet. 2006;28(9):566-566