You searched for:"Fernanda Garanhani Surita"
We found (38) results for your search.Summary
Rev Bras Ginecol Obstet. 2018;40(4):209-224
To review the existing recommendations on the prenatal care of women with systemic lupus erythematosus (SLE), based on currently available scientific evidence.
An integrative review was performed by two independent researchers, based on the literature available in the MEDLINE (via PubMed), EMBASE and The Cochrane Library databases, using the medical subject headings (MeSH) terms “systemic lupus erythematosus” AND “high-risk pregnancy” OR “prenatal care.” Studies published in English between 2007 and 2017 were included; experimental studies and case reports were excluded. In cases of disagreement regarding the inclusion of studies, a third senior researcher was consulted. Forty titles were initially identified; four duplicates were excluded. After reading the abstracts, 7 were further excluded and 29 were selected for a full-text evaluation.
Systemic lupus erythematosus flares, preeclampsia, gestation loss, preterm birth, fetal growth restriction and neonatal lupus syndromes (mainly congenital heartblock) were the major complications described. The multidisciplinary team should adopt a specific monitoring, with particular therapeutic protocols. There are safe and effective drug options that should be prescribed for a good control of SLE activity.
Pregnant women with SLE present an increased risk for maternal complications, pregnancy loss and other adverse outcomes. The disease activity may worsen and, thereby, increase the risk of other maternal-fetal complications. Thus, maintaining an adequate control of disease activity and treating flares quickly should be a central goal during prenatal care.
Summary
Rev Bras Ginecol Obstet. 2018;40(4):209-224
To review the existing recommendations on the prenatal care of women with systemic lupus erythematosus (SLE), based on currently available scientific evidence.
An integrative review was performed by two independent researchers, based on the literature available in the MEDLINE (via PubMed), EMBASE and The Cochrane Library databases, using the medical subject headings (MeSH) terms “systemic lupus erythematosus” AND “high-risk pregnancy” OR “prenatal care.” Studies published in English between 2007 and 2017 were included; experimental studies and case reports were excluded. In cases of disagreement regarding the inclusion of studies, a third senior researcher was consulted. Forty titles were initially identified; four duplicates were excluded. After reading the abstracts, 7 were further excluded and 29 were selected for a full-text evaluation.
Systemic lupus erythematosus flares, preeclampsia, gestation loss, preterm birth, fetal growth restriction and neonatal lupus syndromes (mainly congenital heartblock) were the major complications described. The multidisciplinary team should adopt a specific monitoring, with particular therapeutic protocols. There are safe and effective drug options that should be prescribed for a good control of SLE activity.
Pregnant women with SLE present an increased risk for maternal complications, pregnancy loss and other adverse outcomes. The disease activity may worsen and, thereby, increase the risk of other maternal-fetal complications. Thus, maintaining an adequate control of disease activity and treating flares quickly should be a central goal during prenatal care.
Summary
Rev Bras Ginecol Obstet. 2022;44(3):211-213
Summary
Rev Bras Ginecol Obstet. 2022;44(3):211-213
Summary
Rev Bras Ginecol Obstet. 2023;45(5):221-224
Summary
Rev Bras Ginecol Obstet. 2023;45(5):221-224
Summary
Rev Bras Ginecol Obstet. 2021;43(4):247-249
Summary
Rev Bras Ginecol Obstet. 2021;43(4):247-249
Summary
Rev Bras Ginecol Obstet. 2020;42(5):248-254
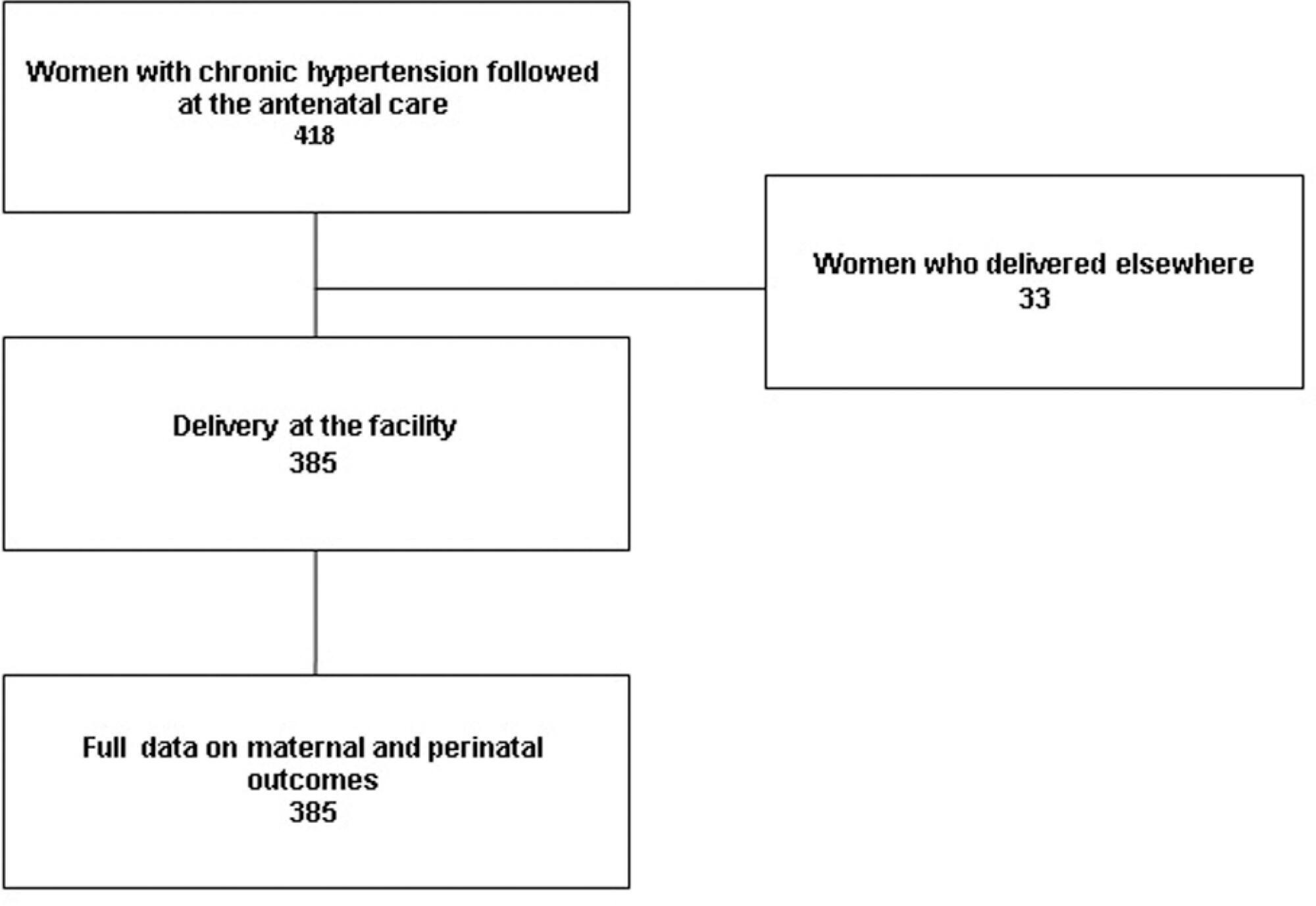
To assess maternal and perinatal outcomes of pregnancies in women with chronic hypertension (CH). Methods Retrospective cohort of women with CH followed at a referral center for a 5 year period (2012-2017). Data were obtained from medical charts review and described as means and frequencies, and a Poisson regression was performed to identify factors independently associated to the occurrence of superimposed preeclampsia (sPE).
A total of 385 women were included in the present study; the majority were > than 30 years old, multiparous, mostly white and obese before pregnancy. One third had pre-eclampsia (PE) in a previous pregnancy and 17% of them had organ damage associated with hypertension, mainly kidney dysfunction. A total of 85% of the patients used aspirin and calcium carbonate for pre-eclampsia prophylaxis and our frequency of sPE was 40%, with an early onset (32.98 ± 6.14 weeks). Of those, 40% had severe features of PE, including 5 cases of HELLP syndrome; however, no cases of eclampsia or maternal death were reported. C-section incidence was high, gestational age at birth was 36 weeks, and nearly a third (115 cases) of newborns had complications at birth One third of the women remained using antihypertensive drugs after pregnancy.
Chronic hypertension is related with the high occurrence of PE, C-sections, prematurity and neonatal complications. Close surveillance and multidisciplinary care are important for early diagnosis of complications.
Summary
Rev Bras Ginecol Obstet. 2020;42(5):248-254
To assess maternal and perinatal outcomes of pregnancies in women with chronic hypertension (CH). Methods Retrospective cohort of women with CH followed at a referral center for a 5 year period (2012-2017). Data were obtained from medical charts review and described as means and frequencies, and a Poisson regression was performed to identify factors independently associated to the occurrence of superimposed preeclampsia (sPE).
A total of 385 women were included in the present study; the majority were > than 30 years old, multiparous, mostly white and obese before pregnancy. One third had pre-eclampsia (PE) in a previous pregnancy and 17% of them had organ damage associated with hypertension, mainly kidney dysfunction. A total of 85% of the patients used aspirin and calcium carbonate for pre-eclampsia prophylaxis and our frequency of sPE was 40%, with an early onset (32.98 ± 6.14 weeks). Of those, 40% had severe features of PE, including 5 cases of HELLP syndrome; however, no cases of eclampsia or maternal death were reported. C-section incidence was high, gestational age at birth was 36 weeks, and nearly a third (115 cases) of newborns had complications at birth One third of the women remained using antihypertensive drugs after pregnancy.
Chronic hypertension is related with the high occurrence of PE, C-sections, prematurity and neonatal complications. Close surveillance and multidisciplinary care are important for early diagnosis of complications.
Summary
Rev Bras Ginecol Obstet. 2023;45(5):253-260
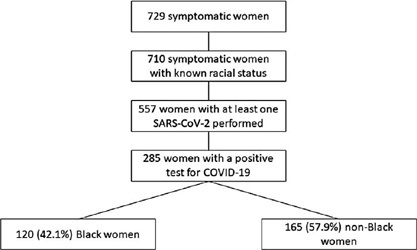
To evaluate the impact of the race (Black versus non-Black) on maternal and perinatal outcomes of pregnant women with COVID-19 in Brazil. Methods This is a subanalysis of REBRACO, a Brazilian multicenter cohort study designed to evaluate the impact of COVID-19 on pregnant women. From February2020 until February 2021, 15 maternity hospitals in Brazil collected data on women with respiratory symptoms. We selected all women with a positive test for COVID-19; then, we divided them into two groups: Black and non-Black women. Finally, we compared, between groups, sociodemographic, maternal, and perinatal outcomes. We obtained the frequency of events in each group and compared them using X2 test; p-values < 0.05 were considered significant. We also estimated the odds ratio (OR) and confidence intervals (CI).
729 symptomatic women were included in the study; of those, 285 were positive for COVID-19, 120 (42.1%) were Black, and 165 (57.9%) were non-Black. Black women had worse education (p = 0.037). The timing of access to the health system was similar between both groups, with 26.3% being included with seven or more days of symptoms. Severe acute respiratory syndrome (OR 2.22 CI 1.17–4.21), intensive care unit admission (OR 2.00 CI 1.07–3.74), and desaturation at admission (OR 3.72 CI 1.41–9.84) were more likely to occur among Black women. Maternal death was higher among Black women (7.8% vs. 2.6%, p = 0.048). Perinatal outcomes were similar between both groups.
Brazilian Black women were more likely to die due to the consequences of COVID-19.
Summary
Rev Bras Ginecol Obstet. 2023;45(5):253-260
To evaluate the impact of the race (Black versus non-Black) on maternal and perinatal outcomes of pregnant women with COVID-19 in Brazil. Methods This is a subanalysis of REBRACO, a Brazilian multicenter cohort study designed to evaluate the impact of COVID-19 on pregnant women. From February2020 until February 2021, 15 maternity hospitals in Brazil collected data on women with respiratory symptoms. We selected all women with a positive test for COVID-19; then, we divided them into two groups: Black and non-Black women. Finally, we compared, between groups, sociodemographic, maternal, and perinatal outcomes. We obtained the frequency of events in each group and compared them using X2 test; p-values < 0.05 were considered significant. We also estimated the odds ratio (OR) and confidence intervals (CI).
729 symptomatic women were included in the study; of those, 285 were positive for COVID-19, 120 (42.1%) were Black, and 165 (57.9%) were non-Black. Black women had worse education (p = 0.037). The timing of access to the health system was similar between both groups, with 26.3% being included with seven or more days of symptoms. Severe acute respiratory syndrome (OR 2.22 CI 1.17–4.21), intensive care unit admission (OR 2.00 CI 1.07–3.74), and desaturation at admission (OR 3.72 CI 1.41–9.84) were more likely to occur among Black women. Maternal death was higher among Black women (7.8% vs. 2.6%, p = 0.048). Perinatal outcomes were similar between both groups.
Brazilian Black women were more likely to die due to the consequences of COVID-19.
Summary
Rev Bras Ginecol Obstet. 2017;39(6):258-264
In the pregnancy-puerperal cycle, women may develop complications that require admission to the Intensive Care Unit (ICU). Thus, special attention to pharmacotherapy is necessary, particularly to potential drug interactions (PDIs) and to the effect of the drugs on the fetus and newborn.
The aim of this study was to determine the profile of PDIs and the potential risk of drugs used during pregnancy and breastfeeding among patients admitted to the ICU.
We conducted an observational, cross-sectional and prospective study, including pregnant and breastfeeding women admitted to the ICU at the Women’s Hospital of a university in the city of Campinas, Brazil, for one year. Online databases were used to identify and classify the PDIs and the potential risk of the drugs used during pregnancy and breastfeeding.
We evaluated 305 prescriptions of 58 women, 31 pregnant and 27 breastfeeding, and 284 (91%) prescriptions presented PDIs. A total of 175 different combinations of PDIs were identified in the prescriptions, and adverse effects caused by the simultaneous use of drugs were not actually observed in the clinical practice. A total of 26 (1.4%) PDIs were classified as contraindicated. We identified 15 (13.8%) drugs prescribed with risk D, and 2 (1.8%) with risk X for pregnant women, as well as 4 (4.9%) drugs prescribed with high risk for breastfeeding women.
This study demonstrates that there is a high incidence of PDIs in prescriptions. Most drugs used by pregnant and breastfeeding women at the ICU did not present serious risks to their fetus and newborns, but sometimes drugs with risk D or X are necessary in the course of the treatment.
Summary
Rev Bras Ginecol Obstet. 2017;39(6):258-264
In the pregnancy-puerperal cycle, women may develop complications that require admission to the Intensive Care Unit (ICU). Thus, special attention to pharmacotherapy is necessary, particularly to potential drug interactions (PDIs) and to the effect of the drugs on the fetus and newborn.
The aim of this study was to determine the profile of PDIs and the potential risk of drugs used during pregnancy and breastfeeding among patients admitted to the ICU.
We conducted an observational, cross-sectional and prospective study, including pregnant and breastfeeding women admitted to the ICU at the Women’s Hospital of a university in the city of Campinas, Brazil, for one year. Online databases were used to identify and classify the PDIs and the potential risk of the drugs used during pregnancy and breastfeeding.
We evaluated 305 prescriptions of 58 women, 31 pregnant and 27 breastfeeding, and 284 (91%) prescriptions presented PDIs. A total of 175 different combinations of PDIs were identified in the prescriptions, and adverse effects caused by the simultaneous use of drugs were not actually observed in the clinical practice. A total of 26 (1.4%) PDIs were classified as contraindicated. We identified 15 (13.8%) drugs prescribed with risk D, and 2 (1.8%) with risk X for pregnant women, as well as 4 (4.9%) drugs prescribed with high risk for breastfeeding women.
This study demonstrates that there is a high incidence of PDIs in prescriptions. Most drugs used by pregnant and breastfeeding women at the ICU did not present serious risks to their fetus and newborns, but sometimes drugs with risk D or X are necessary in the course of the treatment.
Summary
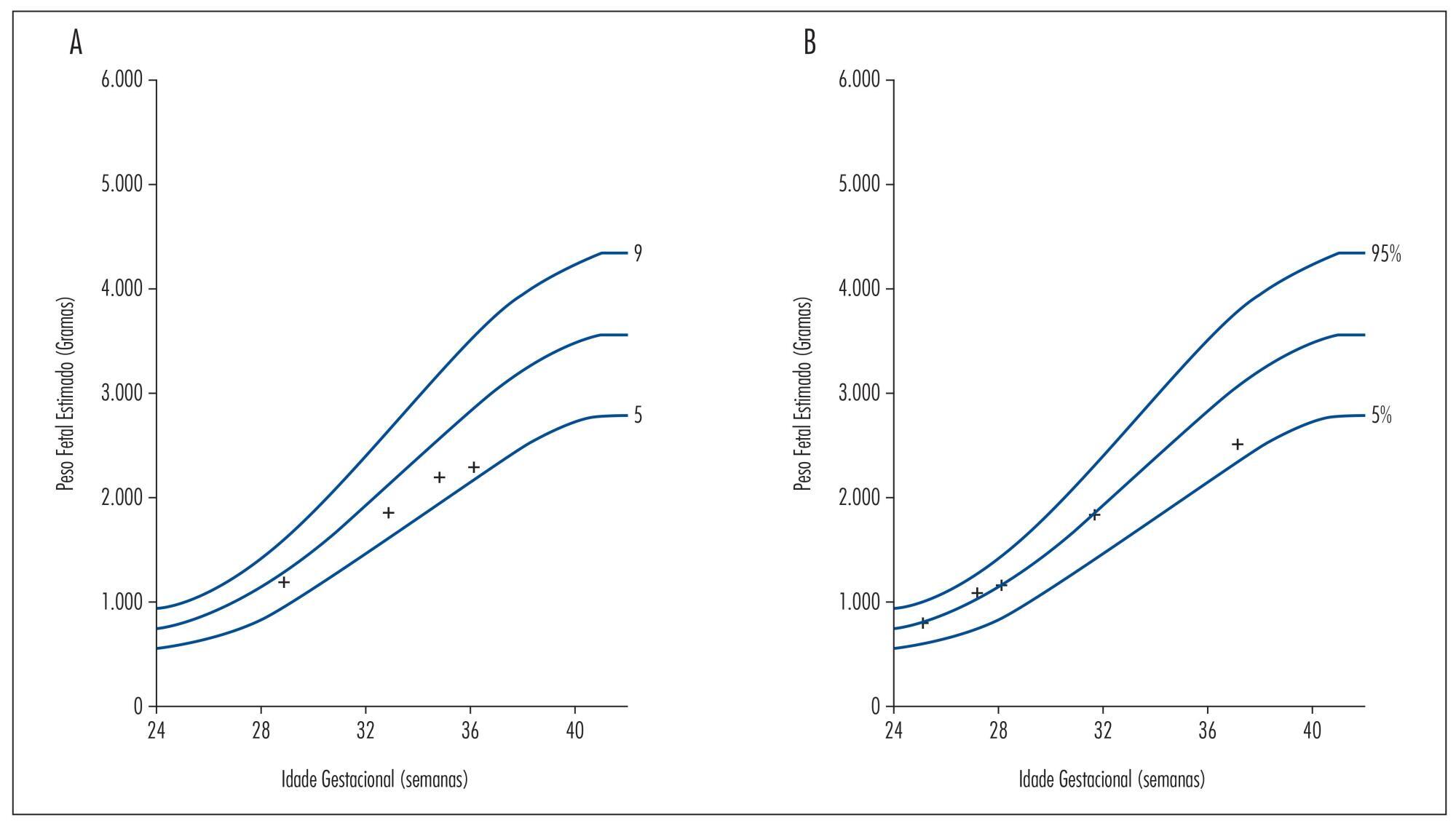
Rev Bras Ginecol Obstet. 2015;37(6):291-296
DOI 10.1590/SO100-720320150005169
Beta thalassemia major is a rare hereditary blood disease in which impaired synthesis
of beta globin chains causes severe anemia. Medical treatment consists of chronic
blood transfusions and iron chelation. We describe two cases of adolescents with beta
thalassemia major with unplanned pregnancies and late onset of prenatal care. One had
worsening of anemia with increased transfusional requirement, fetal growth
restriction, and placental senescence. The other was also diagnosed with
hypothyroidism and low maternal weight, and was admitted twice during pregnancy due
to dengue shock syndrome and influenza H1N1-associated respiratory infection. She
also developed fetal growth restriction and underwent vaginal delivery at term
complicated by uterine hypotonia. Both patients required blood transfusions after
birth and chose medroxyprogesterone as a contraceptive method afterwards. This report
highlights the importance of medical advice on contraceptive methods for these women
and the role of a specialized prenatal follow-up in association with a
hematologist.
Summary
Rev Bras Ginecol Obstet. 2015;37(6):291-296
DOI 10.1590/SO100-720320150005169
Beta thalassemia major is a rare hereditary blood disease in which impaired synthesis
of beta globin chains causes severe anemia. Medical treatment consists of chronic
blood transfusions and iron chelation. We describe two cases of adolescents with beta
thalassemia major with unplanned pregnancies and late onset of prenatal care. One had
worsening of anemia with increased transfusional requirement, fetal growth
restriction, and placental senescence. The other was also diagnosed with
hypothyroidism and low maternal weight, and was admitted twice during pregnancy due
to dengue shock syndrome and influenza H1N1-associated respiratory infection. She
also developed fetal growth restriction and underwent vaginal delivery at term
complicated by uterine hypotonia. Both patients required blood transfusions after
birth and chose medroxyprogesterone as a contraceptive method afterwards. This report
highlights the importance of medical advice on contraceptive methods for these women
and the role of a specialized prenatal follow-up in association with a
hematologist.