You searched for:"Cristina Laguna Benetti-Pinto"
We found (22) results for your search.Summary
Rev Bras Ginecol Obstet. 2023;45(6):312-318
Premature ovarian insufficiency (POI) is characterized by early hypoestrogenism. An increased risk of cardiovascular (CV) disease is a long-term consequence of POI. A challenge of hormone therapy (HT) is to reduce the CV risk.
Cross-sectional study with lipid profile analysis (total cholesterol, LDL-C, HDL-C, VLDL-C and triglycerides), blood glucose levels and arterial blood pressure of women with POI using HT, compared with age and BMI-matched women with normal ovarian function (controls).
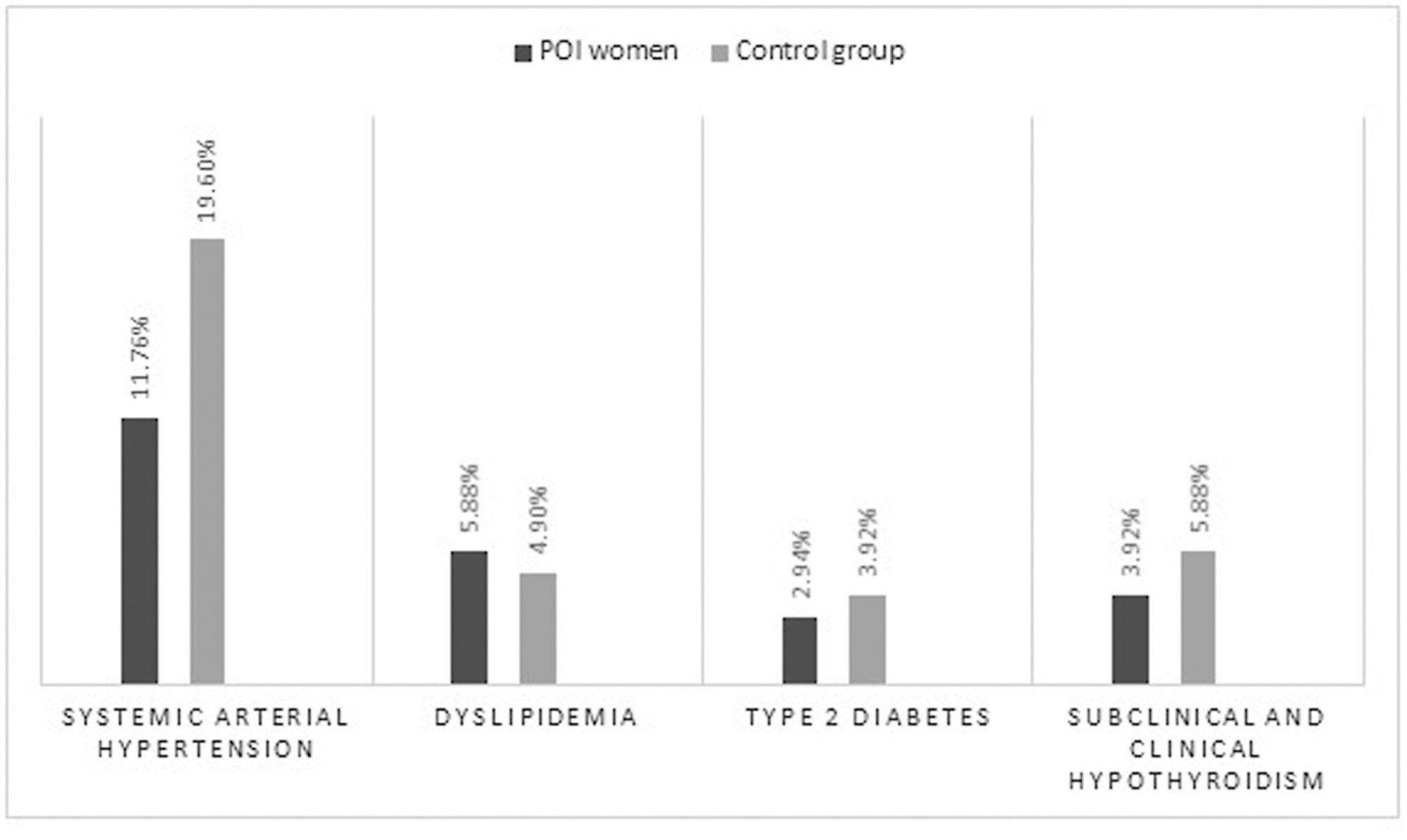
The mean age and BMI of 102 POI patients using HT and 102 controls were 37.2 ± 6.0 and 37.3 ± 5.9 years, respectively; 27.0 ± 5.2 and 27.1 ± 5.4 kg/m2. There wasn't difference between groups in arterial systolic and diastolic blood pressure, blood glucose levels, total cholesterol, LDL-C, VLDL-C and triglycerides. HDL-C levels were significantly higher in the POI group (56.3 ± 14.6 and 52 ± 13.9mg/dL; p = 0.03). Arterial hypertension was the most prevalent chronic disease (12% in the POI group, 19% in the control group, p = ns), followed by dyslipidemia (6 and 5%, in POI and control women).
Women with POI using HT have blood pressure levels, lipid and glycemic profile and prevalence of hypertension and dyslipidemia similar to women of the same age and BMI with preserved gonadal function, in addition to better HDL levels.
Summary
Rev Bras Ginecol Obstet. 2023;45(6):312-318
Premature ovarian insufficiency (POI) is characterized by early hypoestrogenism. An increased risk of cardiovascular (CV) disease is a long-term consequence of POI. A challenge of hormone therapy (HT) is to reduce the CV risk.
Cross-sectional study with lipid profile analysis (total cholesterol, LDL-C, HDL-C, VLDL-C and triglycerides), blood glucose levels and arterial blood pressure of women with POI using HT, compared with age and BMI-matched women with normal ovarian function (controls).
The mean age and BMI of 102 POI patients using HT and 102 controls were 37.2 ± 6.0 and 37.3 ± 5.9 years, respectively; 27.0 ± 5.2 and 27.1 ± 5.4 kg/m2. There wasn't difference between groups in arterial systolic and diastolic blood pressure, blood glucose levels, total cholesterol, LDL-C, VLDL-C and triglycerides. HDL-C levels were significantly higher in the POI group (56.3 ± 14.6 and 52 ± 13.9mg/dL; p = 0.03). Arterial hypertension was the most prevalent chronic disease (12% in the POI group, 19% in the control group, p = ns), followed by dyslipidemia (6 and 5%, in POI and control women).
Women with POI using HT have blood pressure levels, lipid and glycemic profile and prevalence of hypertension and dyslipidemia similar to women of the same age and BMI with preserved gonadal function, in addition to better HDL levels.
Summary
Rev Bras Ginecol Obstet. 2017;39(7):358-368
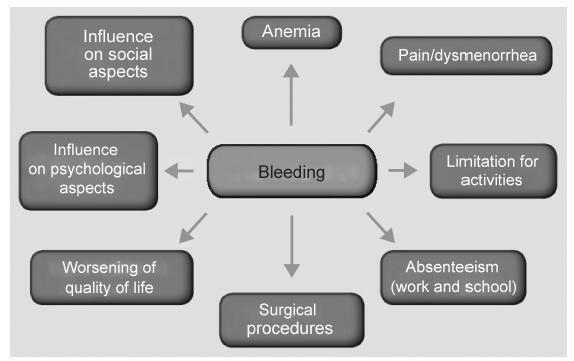
Abnormal uterine bleeding is a frequent condition in Gynecology. It may impact physical, emotional sexual and professional aspects of the lives of women, impairing their quality of life. In cases of acute and severe bleeding, women may need urgent treatment with volumetric replacement and prescription of hemostatic substances. In some specific cases with more intense and prolonged bleeding, surgical treatment may be necessary. The objective of this chapter is to describe the main evidence on the treatment of women with abnormaluterinebleeding, both acuteand chronic.Didactically,thetreatmentoptions were based on the current International Federation of Gynecology and Obstetrics (FIGO) classification system (PALM-COEIN). The etiologies of PALM-COEIN are: uterine Polyp (P), Adenomyosis (A), Leiomyoma (L), precursor and Malignant lesions of the uterine body (M), Coagulopathies (C), Ovulatory dysfunction (O), Endometrial dysfunction (E), Iatrogenic (I), and Not yet classified (N). The articles were selected according to the recommendation grades of the PubMed, Cochrane and Embase databases, and those in which the main objective was the reduction of uterine menstrual bleeding were included. Only studies written in English were included. All editorial or complete papers that were not consistent with abnormal uterine bleeding, or studies in animal models, were excluded. The main objective of the treatment is the reduction of menstrual flow and morbidity and the improvement of quality of life. It is important to emphasize that the treatment in the acute phase aims to hemodynamically stabilize the patient and stop excessive bleeding, while the treatment in the chronic phase is based on correcting menstrual dysfunction according to its etiology and clinical manifestations. The treatment may be surgical or pharmacological, and thelatterisbasedmainlyonhormonaltherapy,anti-inflammatorydrugsandantifibrinolytics.
Summary
Rev Bras Ginecol Obstet. 2017;39(7):358-368
Abnormal uterine bleeding is a frequent condition in Gynecology. It may impact physical, emotional sexual and professional aspects of the lives of women, impairing their quality of life. In cases of acute and severe bleeding, women may need urgent treatment with volumetric replacement and prescription of hemostatic substances. In some specific cases with more intense and prolonged bleeding, surgical treatment may be necessary. The objective of this chapter is to describe the main evidence on the treatment of women with abnormaluterinebleeding, both acuteand chronic.Didactically,thetreatmentoptions were based on the current International Federation of Gynecology and Obstetrics (FIGO) classification system (PALM-COEIN). The etiologies of PALM-COEIN are: uterine Polyp (P), Adenomyosis (A), Leiomyoma (L), precursor and Malignant lesions of the uterine body (M), Coagulopathies (C), Ovulatory dysfunction (O), Endometrial dysfunction (E), Iatrogenic (I), and Not yet classified (N). The articles were selected according to the recommendation grades of the PubMed, Cochrane and Embase databases, and those in which the main objective was the reduction of uterine menstrual bleeding were included. Only studies written in English were included. All editorial or complete papers that were not consistent with abnormal uterine bleeding, or studies in animal models, were excluded. The main objective of the treatment is the reduction of menstrual flow and morbidity and the improvement of quality of life. It is important to emphasize that the treatment in the acute phase aims to hemodynamically stabilize the patient and stop excessive bleeding, while the treatment in the chronic phase is based on correcting menstrual dysfunction according to its etiology and clinical manifestations. The treatment may be surgical or pharmacological, and thelatterisbasedmainlyonhormonaltherapy,anti-inflammatorydrugsandantifibrinolytics.
Summary
Rev Bras Ginecol Obstet. 2022;44(4):369-375
To compare the oocyte maturation rate in the treatment of in vitro fertilization (IVF) in terms of the use of human chorionic gonadotropin (hCG), agonist gonadotropin-releasing hormone (GnRH) and dual trigger and to evaluate the associated risk factors for sub-optimal maturation rates.
A retrospective cohort study with 856 women who underwent IVF. They performed oocyte retrieval and were classified into 3 groups (1 - hCG, 2 - GnRHagonist, 3 - dual trigger). The primary outcome was maturation rate per trigger, and the secondary outcomes were the pregnancy rate per oocyte retrieval and the correlations between low maturation rate as well as the clinical and treatment characteristics of women.
The maturation rate was 77% in group 1; 76% in group 2, and 83% in group 3 (p=0.003). Group 2 showed women with better ovarian reserve, greater number of oocytes collected, and more mature oocytes and embryos compared with the other groups (p<0.001). The cumulative clinical pregnancy rate was no different between the groups (p=0.755). Low ovarian reserve and low doses of follicle-stimulating hormone (FSH) administered during the stimulus were associated with a higher chance of null maturation rate.
The oocyte maturation rates and IVF results were similar in all groups. Low ovarian reserve is associated with the worst treatment results.
Summary
Rev Bras Ginecol Obstet. 2022;44(4):369-375
To compare the oocyte maturation rate in the treatment of in vitro fertilization (IVF) in terms of the use of human chorionic gonadotropin (hCG), agonist gonadotropin-releasing hormone (GnRH) and dual trigger and to evaluate the associated risk factors for sub-optimal maturation rates.
A retrospective cohort study with 856 women who underwent IVF. They performed oocyte retrieval and were classified into 3 groups (1 - hCG, 2 - GnRHagonist, 3 - dual trigger). The primary outcome was maturation rate per trigger, and the secondary outcomes were the pregnancy rate per oocyte retrieval and the correlations between low maturation rate as well as the clinical and treatment characteristics of women.
The maturation rate was 77% in group 1; 76% in group 2, and 83% in group 3 (p=0.003). Group 2 showed women with better ovarian reserve, greater number of oocytes collected, and more mature oocytes and embryos compared with the other groups (p<0.001). The cumulative clinical pregnancy rate was no different between the groups (p=0.755). Low ovarian reserve and low doses of follicle-stimulating hormone (FSH) administered during the stimulus were associated with a higher chance of null maturation rate.
The oocyte maturation rates and IVF results were similar in all groups. Low ovarian reserve is associated with the worst treatment results.
Summary
Rev Bras Ginecol Obstet. 2017;39(8):403-407
To determine the clinical and epidemiological characteristics of abdominal wall endometriosis (AWE), as well as the rate and recurrence factors for the disease.
A retrospective study of 52 women with AWE was performed at Universidade Estadual de Campinas from 2004 to 2014. Of the 231 surgeries performed for the diagnosis of endometriosis, 52 women were found to have abdominal wall endometriosis (AWE). The frequencies, means and standard deviations of the clinical characteristics of these women were calculated, as well as the recurrence rate of AWE. To determine the risk factors for disease recurrence, Fisher’s exact test was used.
The mean age of the patients was 30.71 ± 5.91 years. The main clinical manifestations were pain (98%) and sensation of a mass (36.5%).We observed that 94% of these women had undergone at least 1 cesarean section, and 73% had used medication for the postoperative control of endometriosis. The lesion was most commonly located in the cesarean section scar (65%). The recurrence rate of the disease was of 26.9%. All 14 women who had relapsed had surgical margins compromised in the previous surgery. There was no correlation between recurrent AWE and a previous cesarean section (p = 0.18), previous laparotomy (p = 0.11), previous laparoscopy (p = 0.12) and postoperative hormone therapy (p = 0.51).
Women with previous cesarean sections with local pain or lumps should be investigated for AWE. The recurrence of AWE is high, especially when the first surgery is not appropriate and leaves compromised surgical margins.
Summary
Rev Bras Ginecol Obstet. 2017;39(8):403-407
To determine the clinical and epidemiological characteristics of abdominal wall endometriosis (AWE), as well as the rate and recurrence factors for the disease.
A retrospective study of 52 women with AWE was performed at Universidade Estadual de Campinas from 2004 to 2014. Of the 231 surgeries performed for the diagnosis of endometriosis, 52 women were found to have abdominal wall endometriosis (AWE). The frequencies, means and standard deviations of the clinical characteristics of these women were calculated, as well as the recurrence rate of AWE. To determine the risk factors for disease recurrence, Fisher’s exact test was used.
The mean age of the patients was 30.71 ± 5.91 years. The main clinical manifestations were pain (98%) and sensation of a mass (36.5%).We observed that 94% of these women had undergone at least 1 cesarean section, and 73% had used medication for the postoperative control of endometriosis. The lesion was most commonly located in the cesarean section scar (65%). The recurrence rate of the disease was of 26.9%. All 14 women who had relapsed had surgical margins compromised in the previous surgery. There was no correlation between recurrent AWE and a previous cesarean section (p = 0.18), previous laparotomy (p = 0.11), previous laparoscopy (p = 0.12) and postoperative hormone therapy (p = 0.51).
Women with previous cesarean sections with local pain or lumps should be investigated for AWE. The recurrence of AWE is high, especially when the first surgery is not appropriate and leaves compromised surgical margins.
Summary
Rev Bras Ginecol Obstet. 2022;44(5):503-510
To evaluate the impact of surgical treatment of deep infiltrative endometriosis (DIE) on pelvic floor dysfunction (urinary incontinence [UI], pelvic organ prolapse [POP], fecal incontinence [FI)] or constipation, and sexual function [dyspareunia]).
The present systematic review was performed in the PubMed database. For the selection of studies, articles should be published by January 5, 2021, without language restriction.
Six randomized controlled studies that evaluated surgical treatment for DIE and the comparison of different surgical techniques were included.
The studies were selected independently by title and abstract by two authors. Disagreements were resolved by a third author. All included studies were also evaluated according to the Cochrane risk of bias tool and the quality of the evidence was analyzed using the GRADE criteria. Subgroup analysis by different treatments and follow-up periods was also performed.
Six studies were included in the quantitative analysis. The risk of bias between studies showed an uncertain risk of bias for most studies, with concealment of allocation being the least reported category. The quality of the evidence was considered low. High heterogeneity was found between the studies. No study has evaluated UI or POP comparatively before and after surgery.
Dyspareunia and FI have improved after the surgical procedure, but it was not possible to demonstratewhich surgical technique was related to these outcomes as there was surgical heterogeneity. This diversity was found across data, with the recommendation of future prospective studies addressing pelvic floor disorders withDIE.
Summary
Rev Bras Ginecol Obstet. 2022;44(5):503-510
To evaluate the impact of surgical treatment of deep infiltrative endometriosis (DIE) on pelvic floor dysfunction (urinary incontinence [UI], pelvic organ prolapse [POP], fecal incontinence [FI)] or constipation, and sexual function [dyspareunia]).
The present systematic review was performed in the PubMed database. For the selection of studies, articles should be published by January 5, 2021, without language restriction.
Six randomized controlled studies that evaluated surgical treatment for DIE and the comparison of different surgical techniques were included.
The studies were selected independently by title and abstract by two authors. Disagreements were resolved by a third author. All included studies were also evaluated according to the Cochrane risk of bias tool and the quality of the evidence was analyzed using the GRADE criteria. Subgroup analysis by different treatments and follow-up periods was also performed.
Six studies were included in the quantitative analysis. The risk of bias between studies showed an uncertain risk of bias for most studies, with concealment of allocation being the least reported category. The quality of the evidence was considered low. High heterogeneity was found between the studies. No study has evaluated UI or POP comparatively before and after surgery.
Dyspareunia and FI have improved after the surgical procedure, but it was not possible to demonstratewhich surgical technique was related to these outcomes as there was surgical heterogeneity. This diversity was found across data, with the recommendation of future prospective studies addressing pelvic floor disorders withDIE.
Summary
Rev Bras Ginecol Obstet. 2020;42(8):511-518
Summary
Rev Bras Ginecol Obstet. 2020;42(8):511-518
Summary
Rev Bras Ginecol Obstet. 2019;41(9):564-574
To assess the efficacy of non-surgical treatment for adenomyosis.
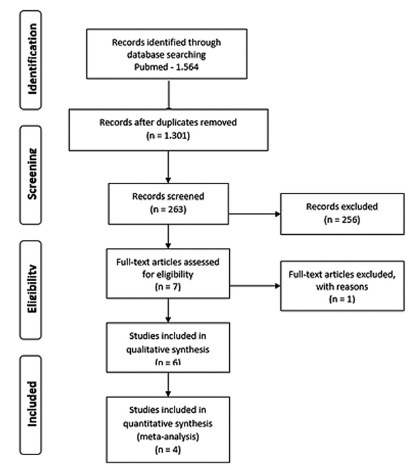
A search was performed by two authors in the Pubmed, Scopus, and Scielo databases and in the grey literature from inception to March 2018, with no language restriction.
We have included prospective randomized studies for treating symptomaticwomen with adenomyosis (abnormal uterine bleeding and/or pelvic pain) diagnosed by ultrasound or magnetic resonance imaging.
Studies were primarily selected by title and abstract. The articles that were eligible for inclusion were evaluated in their entirety, and their data was extracted for further processing and analysis.
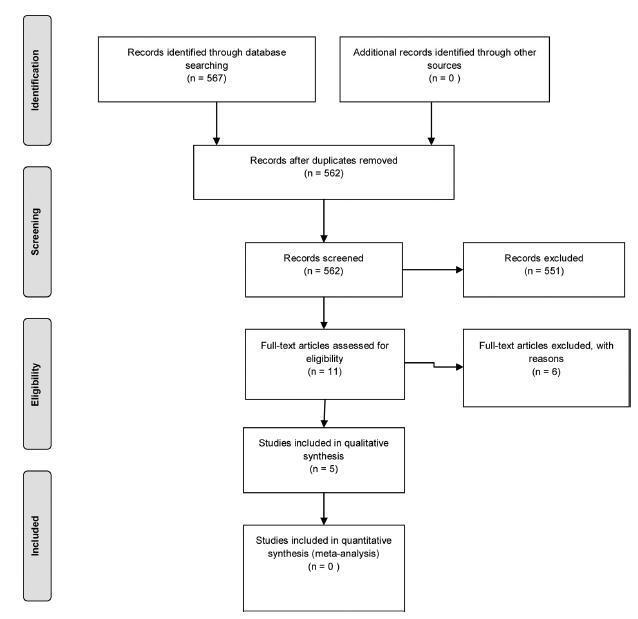
From567retrieved records only 5 remained for analysis. The intervention groups were: levonorgestrel intrauterine system (LNG-IUS)(n= 2), dienogest (n= 2), and letrozole (n= 1). Levonorgestrel intrauterine system was effective to control bleeding when compared to hysterectomy or combined oral contraceptives (COCs). One study assessed chronic pelvic pain and reported that LNG-IUS was superior to COC to reduce symptoms. Regarding dienogest, it was efficient to reduce pelvic pain when compared to placebo or goserelin, but less effective to control bleeding than gonadotropin-releasing hormone (GnRH) analog. Letrozolewas as efficient asGnRHanalog to relieve dysmenorrhea and dyspareunia, but not for chronic pelvic pain. Reduction of uterine volumewas seen with aromatase inhibitors, GnRH analog, and LGN-IUD.
Levonorgestrel intrauterine system and dienogest have significantly improved the control of bleeding and pelvic pain, respectively, in women with adenomyosis. However, there is insufficient data from the retrieved studies to endorse eachmedication for this disease. Further randomized control tests (RCTs) are needed to address pharmacological treatment of adenomyosis.
Summary
Rev Bras Ginecol Obstet. 2019;41(9):564-574
To assess the efficacy of non-surgical treatment for adenomyosis.
A search was performed by two authors in the Pubmed, Scopus, and Scielo databases and in the grey literature from inception to March 2018, with no language restriction.
We have included prospective randomized studies for treating symptomaticwomen with adenomyosis (abnormal uterine bleeding and/or pelvic pain) diagnosed by ultrasound or magnetic resonance imaging.
Studies were primarily selected by title and abstract. The articles that were eligible for inclusion were evaluated in their entirety, and their data was extracted for further processing and analysis.
From567retrieved records only 5 remained for analysis. The intervention groups were: levonorgestrel intrauterine system (LNG-IUS)(n= 2), dienogest (n= 2), and letrozole (n= 1). Levonorgestrel intrauterine system was effective to control bleeding when compared to hysterectomy or combined oral contraceptives (COCs). One study assessed chronic pelvic pain and reported that LNG-IUS was superior to COC to reduce symptoms. Regarding dienogest, it was efficient to reduce pelvic pain when compared to placebo or goserelin, but less effective to control bleeding than gonadotropin-releasing hormone (GnRH) analog. Letrozolewas as efficient asGnRHanalog to relieve dysmenorrhea and dyspareunia, but not for chronic pelvic pain. Reduction of uterine volumewas seen with aromatase inhibitors, GnRH analog, and LGN-IUD.
Levonorgestrel intrauterine system and dienogest have significantly improved the control of bleeding and pelvic pain, respectively, in women with adenomyosis. However, there is insufficient data from the retrieved studies to endorse eachmedication for this disease. Further randomized control tests (RCTs) are needed to address pharmacological treatment of adenomyosis.
Summary
Rev Bras Ginecol Obstet. 2008;30(12):609-613
DOI 10.1590/S0100-72032008001200004
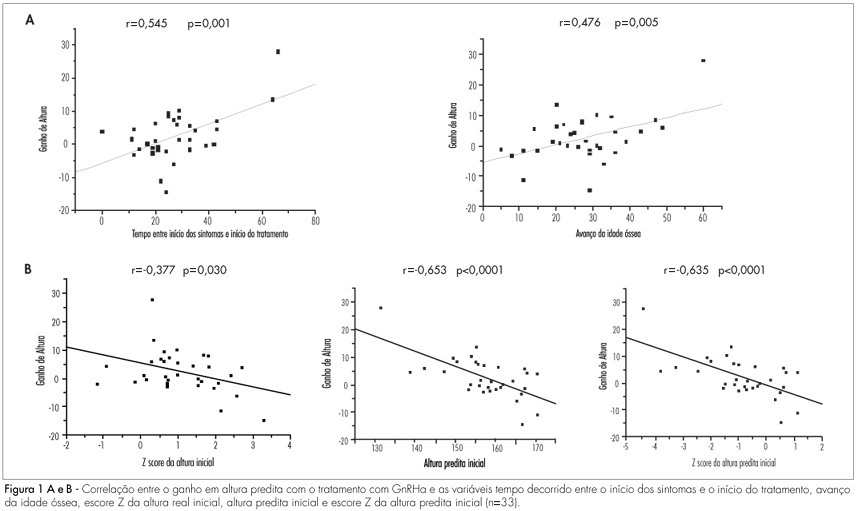
PURPOSE: to evaluate predictive factors of response to GnRHa treatment in girls with idiopathic central precocious puberty. METHODS: a retrospective cohort study was conducted involving 33 girls diagnosed with idiopathic central precocious puberty and treated with GnRHa. The following independent variables were assessed: age at the beginning of therapy and at the onset of symptoms, time elapsed since the appearance of pubertal characteristics and the beginning of treatment, bone age, bone age advance, duration of GnRHa treatment, actual height and Z-score, predicted height and Z-score and hormone measurements of FSH and LH after GnRH stimulation, which were correlated with gain in height as a dependent variable at treatment discontinuation, calculated by the difference between the predicted height at the end and beginning of treatment. For statistical analysis, Pearson's linear correlation was used, in addition to multiple linear regression analysis. RESULTS: the mean age at the beginning of treatment was 7.8±1.3 years, with a mean bone age of 10.1±1.6 years. Bone age advance was 2.3±1.1 years and was controlled during the treatment period. Gain in predicted height was 2.5±1.3cm. It was positively correlated with time elapsed since the beginning of symptoms and the beginning of treatment and with bone age advance, while negatively correlated with the Z-score of height at the beginning of treatment and predicted height at the beginning of treatment, and the latter was the main factor determining gain from treatment. CONCLUSIONS: girls who had the most significant compromise of predicted adult height, as detected by a larger deviation from the population (Z-score) and the most considerable advance in bone age, received benefit from GnRHa therapy, and they must not be excluded from the group to be treated.
Summary
Rev Bras Ginecol Obstet. 2008;30(12):609-613
DOI 10.1590/S0100-72032008001200004
PURPOSE: to evaluate predictive factors of response to GnRHa treatment in girls with idiopathic central precocious puberty. METHODS: a retrospective cohort study was conducted involving 33 girls diagnosed with idiopathic central precocious puberty and treated with GnRHa. The following independent variables were assessed: age at the beginning of therapy and at the onset of symptoms, time elapsed since the appearance of pubertal characteristics and the beginning of treatment, bone age, bone age advance, duration of GnRHa treatment, actual height and Z-score, predicted height and Z-score and hormone measurements of FSH and LH after GnRH stimulation, which were correlated with gain in height as a dependent variable at treatment discontinuation, calculated by the difference between the predicted height at the end and beginning of treatment. For statistical analysis, Pearson's linear correlation was used, in addition to multiple linear regression analysis. RESULTS: the mean age at the beginning of treatment was 7.8±1.3 years, with a mean bone age of 10.1±1.6 years. Bone age advance was 2.3±1.1 years and was controlled during the treatment period. Gain in predicted height was 2.5±1.3cm. It was positively correlated with time elapsed since the beginning of symptoms and the beginning of treatment and with bone age advance, while negatively correlated with the Z-score of height at the beginning of treatment and predicted height at the beginning of treatment, and the latter was the main factor determining gain from treatment. CONCLUSIONS: girls who had the most significant compromise of predicted adult height, as detected by a larger deviation from the population (Z-score) and the most considerable advance in bone age, received benefit from GnRHa therapy, and they must not be excluded from the group to be treated.