You searched for:"Antonio Braga"
We found (19) results for your search.Summary
Rev Bras Ginecol Obstet. 2015;37(6):258-265
DOI 10.1590/SO100-720320150005366
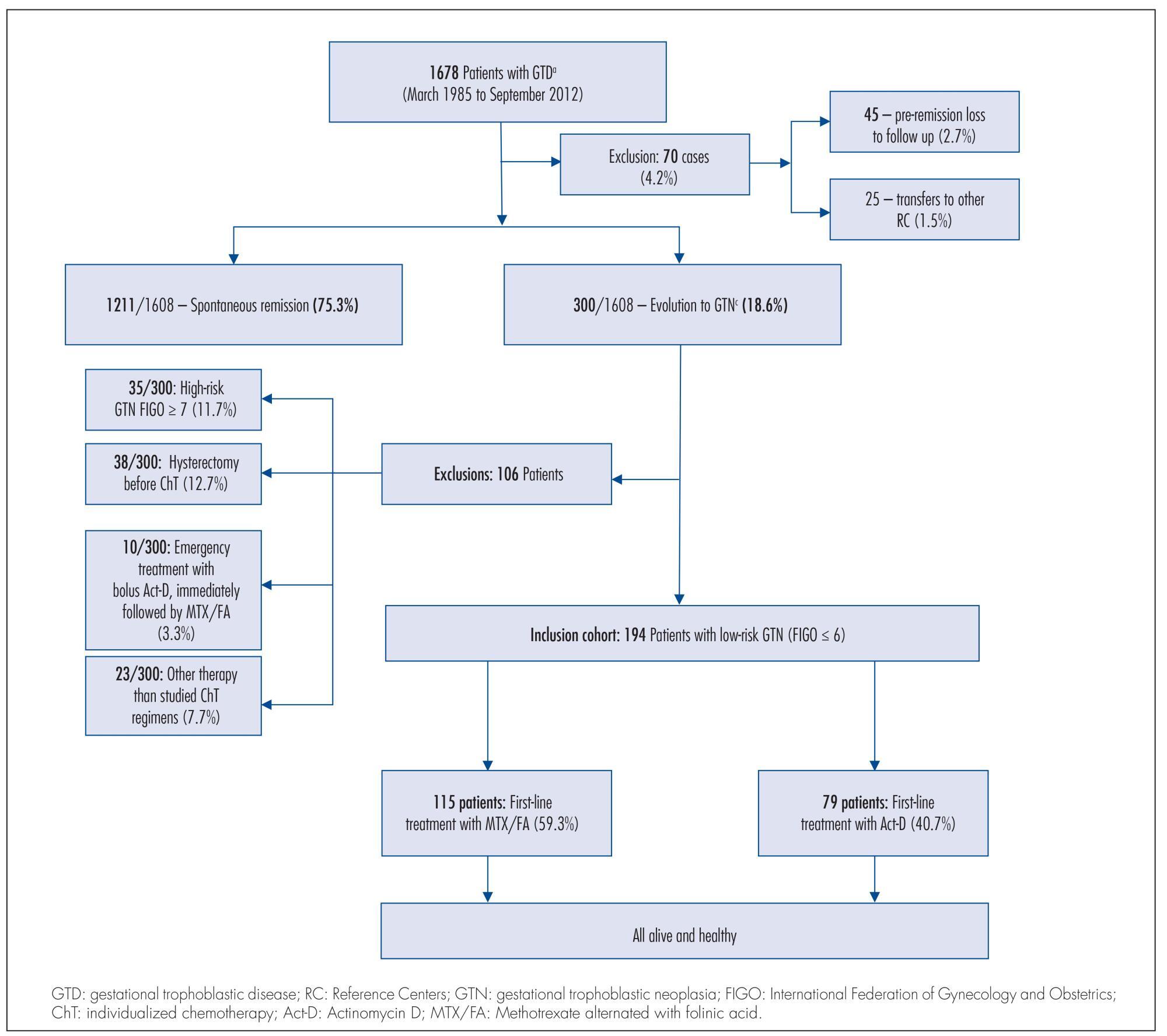
To compare two single-agent chemotherapy (ChT) regimens evaluating, in first-line treatment, response and side effects and, in final single-agent treatment, the outcomes, among Brazilian patients with low-risk gestational trophoblastic neoplasia (GTN), according to International Federation of Gynecology and Obstetrics (FIGO) 2002.
Retrospective analysis of two concurrent cohorts with 194 low-risk GTN patients: from 1992 to 2012, as first-line treatment, 115 patients received 4 intramuscular doses of methotrexate alternated with 4 oral doses of folinic acid (MTX/FA) repetead every 14 days and, since 1996, 79 patients received an endovenous bolus-dose of actinomycin D (Act-D), biweekly. At GTN diagnosis, patient opinion was taken into consideration when defining the initial single-agent ChT regimen, and when there was resistance or toxicity to one regimen, the other drug was used preferentially. This study was approved by the Irmandade da Santa Casa de Misericórdia de Porto Alegre Ethical Committee.
Both groups were clinically similar (p>0.05). In first-line treatments, frequency of complete response was similar (75.7% with MTX/FA and 67.1% with bolus Act-D); the number of ChT courses -median 3 (range: 1-10) with MTX/FA and 2 (range: 1-6) with bolus Act-D - and the time to remission -median 9 weeks (range: 2-16) with MTX/FA and 10 weeks (range: 2-16) with bolus Act-D) - were not different between the groups. In both groups, first-line side effects frequency were high but intensity was low; stomatitis was higher with MTX/FA (p<0.01) and nausea and vomit with Act-D (p<0.01). Final single-agent ChT responses were high in both groups (94.8% with MTX/FA and 83.5% with bolus Act-D; p<0.01) and 13% higher in the group initially treated with MTX/FA. Rates of hysterectomy and of GTN recurrence were low and similar. No patient died due to GTN.
The two regimens had similar first-line ChT response. Final single-agent response rates were high and similar in both groups but the final single-agent remission rate was higher in the MTX/FA group.
Summary
Rev Bras Ginecol Obstet. 2015;37(6):258-265
DOI 10.1590/SO100-720320150005366
To compare two single-agent chemotherapy (ChT) regimens evaluating, in first-line treatment, response and side effects and, in final single-agent treatment, the outcomes, among Brazilian patients with low-risk gestational trophoblastic neoplasia (GTN), according to International Federation of Gynecology and Obstetrics (FIGO) 2002.
Retrospective analysis of two concurrent cohorts with 194 low-risk GTN patients: from 1992 to 2012, as first-line treatment, 115 patients received 4 intramuscular doses of methotrexate alternated with 4 oral doses of folinic acid (MTX/FA) repetead every 14 days and, since 1996, 79 patients received an endovenous bolus-dose of actinomycin D (Act-D), biweekly. At GTN diagnosis, patient opinion was taken into consideration when defining the initial single-agent ChT regimen, and when there was resistance or toxicity to one regimen, the other drug was used preferentially. This study was approved by the Irmandade da Santa Casa de Misericórdia de Porto Alegre Ethical Committee.
Both groups were clinically similar (p>0.05). In first-line treatments, frequency of complete response was similar (75.7% with MTX/FA and 67.1% with bolus Act-D); the number of ChT courses -median 3 (range: 1-10) with MTX/FA and 2 (range: 1-6) with bolus Act-D - and the time to remission -median 9 weeks (range: 2-16) with MTX/FA and 10 weeks (range: 2-16) with bolus Act-D) - were not different between the groups. In both groups, first-line side effects frequency were high but intensity was low; stomatitis was higher with MTX/FA (p<0.01) and nausea and vomit with Act-D (p<0.01). Final single-agent ChT responses were high in both groups (94.8% with MTX/FA and 83.5% with bolus Act-D; p<0.01) and 13% higher in the group initially treated with MTX/FA. Rates of hysterectomy and of GTN recurrence were low and similar. No patient died due to GTN.
The two regimens had similar first-line ChT response. Final single-agent response rates were high and similar in both groups but the final single-agent remission rate was higher in the MTX/FA group.
Summary
Rev Bras Ginecol Obstet. 2018;40(5):294-299
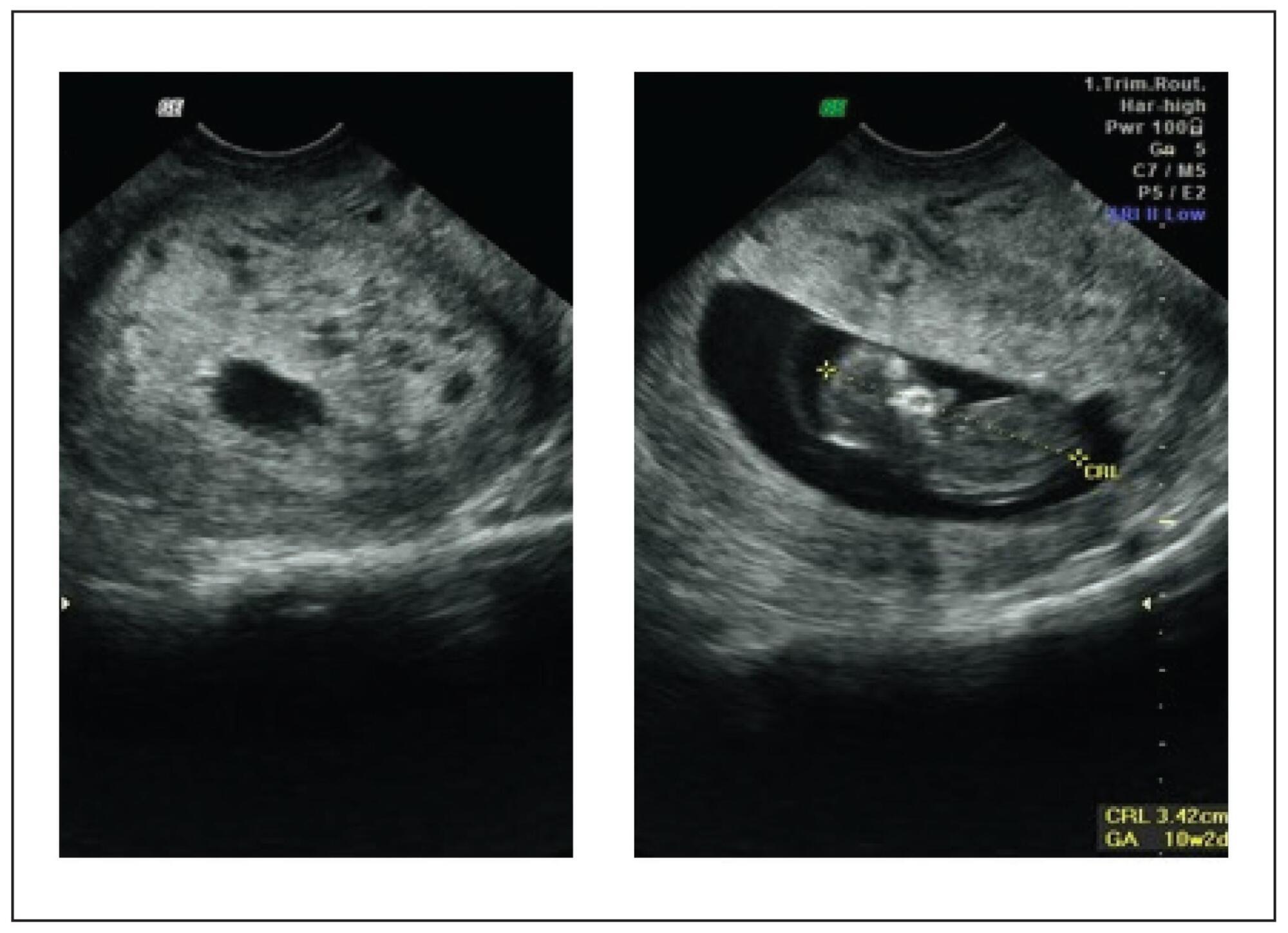
This report presents the case of a patient with gestational trophoblastic neoplasia after a partial hydatidiform mole formed in the Fallopian tube. Ectopic molar pregnancy is a rare condition, with an estimated incidence of 1 in every 20,000 to 100,000 pregnancies; less than 300 cases of it have been reported in the Western literature. The present report is important because it presents current diagnostic criteria for this rare condition, which has been incorrectly diagnosed in the past, not only morphologically but also immunohistochemically. It also draws the attention of obstetricians to the occurrence of ectopic molar pregnancy, which tends to progress to Fallopian tube rupture more often than in cases of ectopic non-molar pregnancy. Progression to gestational trophoblastic neoplasia ensures that patients with ectopic molar pregnancy must undergo postmolar monitoring, which must be just as thorough as that of patients with intrauterine hydatidiform moles, even if chemotherapy results in high cure rates.
Summary
Rev Bras Ginecol Obstet. 2018;40(5):294-299
This report presents the case of a patient with gestational trophoblastic neoplasia after a partial hydatidiform mole formed in the Fallopian tube. Ectopic molar pregnancy is a rare condition, with an estimated incidence of 1 in every 20,000 to 100,000 pregnancies; less than 300 cases of it have been reported in the Western literature. The present report is important because it presents current diagnostic criteria for this rare condition, which has been incorrectly diagnosed in the past, not only morphologically but also immunohistochemically. It also draws the attention of obstetricians to the occurrence of ectopic molar pregnancy, which tends to progress to Fallopian tube rupture more often than in cases of ectopic non-molar pregnancy. Progression to gestational trophoblastic neoplasia ensures that patients with ectopic molar pregnancy must undergo postmolar monitoring, which must be just as thorough as that of patients with intrauterine hydatidiform moles, even if chemotherapy results in high cure rates.
Summary
Rev Bras Ginecol Obstet. 2021;43(4):323-328
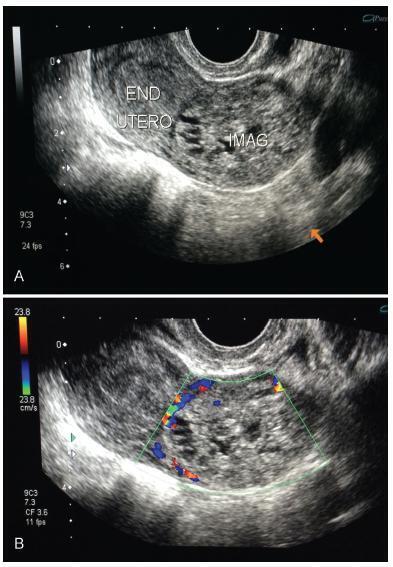
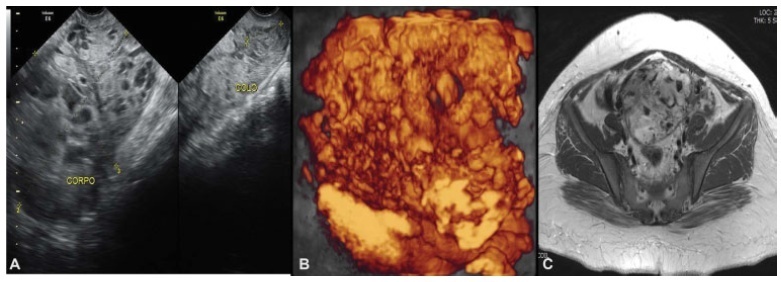
Complete hydatidiform mole (CHM) is a rare type of pregnancy, in which 15 to 20% of the cases may develop into gestational trophoblastic neoplasia (GTN). The diagnostic of GTN must be done as early as possible through weekly surveillance of serum hCG after uterine evacuation.We report the case of 23-year-old primigravida, with CHM but without surveillance of hCG after uterine evacuation. Two months later, the patient presented to the emergency with vaginal bleeding and was referred to the Centro de Doenças Trofoblásticas do Hospital São Paulo. She was diagnosed with high risk GTN stage/score III:7 as per The International Federation of Gynecology and Obstetrics/World Health Organization (FIGO/WHO). The sonographic examination revealed enlarged uterus with a heterogeneous mass constituted of multiple large vessels invading and causing disarrangement of the myometrium. The patient evolved with progressive worsening of vaginal bleeding after chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine (EMA-CO) regimen. She underwent blood transfusion and embolization of uterine arteries due to severe vaginal hemorrhage episodes, with complete control of bleeding. The hCG reached a negative value after the third cycle, and there was a complete regression of the anomalous vascularization of the uterus as well as full recovery of the uterine anatomy. The treatment in a reference center was essential for the appropriate management, especially regarding the uterine arteries embolization trough percutaneous femoral
Summary
Rev Bras Ginecol Obstet. 2021;43(4):323-328
Complete hydatidiform mole (CHM) is a rare type of pregnancy, in which 15 to 20% of the cases may develop into gestational trophoblastic neoplasia (GTN). The diagnostic of GTN must be done as early as possible through weekly surveillance of serum hCG after uterine evacuation.We report the case of 23-year-old primigravida, with CHM but without surveillance of hCG after uterine evacuation. Two months later, the patient presented to the emergency with vaginal bleeding and was referred to the Centro de Doenças Trofoblásticas do Hospital São Paulo. She was diagnosed with high risk GTN stage/score III:7 as per The International Federation of Gynecology and Obstetrics/World Health Organization (FIGO/WHO). The sonographic examination revealed enlarged uterus with a heterogeneous mass constituted of multiple large vessels invading and causing disarrangement of the myometrium. The patient evolved with progressive worsening of vaginal bleeding after chemotherapy with etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine (EMA-CO) regimen. She underwent blood transfusion and embolization of uterine arteries due to severe vaginal hemorrhage episodes, with complete control of bleeding. The hCG reached a negative value after the third cycle, and there was a complete regression of the anomalous vascularization of the uterus as well as full recovery of the uterine anatomy. The treatment in a reference center was essential for the appropriate management, especially regarding the uterine arteries embolization trough percutaneous femoral
Summary
Rev Bras Ginecol Obstet. 2015;37(7):339-343
DOI 10.1590/S0100-720320150005318
We report here a case of gestational trophoblastic neoplasia after spontaneous normalization of human chorionic gonadotropin in a patient with a partial hydatidiform mole. This is the second occurrence of this event to be reported and the first one with proven immunohistochemical evidence. Besides showing the treatment for this pregnancy complication, this case report discusses the possibility of reducing the duration of post-molar follow-up, as well as strategies for early recognition of gestational trophoblastic neoplasia after spontaneous remission of molar pregnancy.
Summary
Rev Bras Ginecol Obstet. 2015;37(7):339-343
DOI 10.1590/S0100-720320150005318
We report here a case of gestational trophoblastic neoplasia after spontaneous normalization of human chorionic gonadotropin in a patient with a partial hydatidiform mole. This is the second occurrence of this event to be reported and the first one with proven immunohistochemical evidence. Besides showing the treatment for this pregnancy complication, this case report discusses the possibility of reducing the duration of post-molar follow-up, as well as strategies for early recognition of gestational trophoblastic neoplasia after spontaneous remission of molar pregnancy.
Summary
Rev Bras Ginecol Obstet. 2022;44(4):343-351
To evaluate the emotional and clinical aspects observed in women with gestational trophoblastic disease (GTD) followed-up in a reference center (RC) by a multidisciplinary team.
Retrospective cohort study of the clinical records of 186 women with GTD and of the emotional aspects (EA) observed in these women by a teamof psychologists and reported by the 389 support groups conducted from 2014 to 2018.
The women were young (mean age: 31.2 years), 47% had no living child, 60% had planned the pregnancy, and 50% participated in two or more SG. Most women (n=137; 73.6%) reached spontaneous remission ofmolar gestation in a median time of 10 weeks and had a total follow-up time of seven months. In the group of 49 women (26.3%) who progressed to gestational trophoblastic neoplasia (GTN), time to remission after chemotherapy was 18 weeks, and total follow-up time was 36 months. EA included different levels of anxiety and depression,more evident in 9.1% of the women; these symptoms tended to occur more frequently in women older than 40 years (p=0.067), less educated (p=0.054), and whose disease progressed to GTN (p=0.018), as well as in those who had to undergo multi-agent chemotherapy (p=0.028) or hysterectomy (p=0.001) adjuvant to clinical treatment.
This study found several EA in association with all types of GTD. It also highlights the importance of specialized care only found in a RC, essential to support the recovery of the mental health of these women.
Summary
Rev Bras Ginecol Obstet. 2022;44(4):343-351
To evaluate the emotional and clinical aspects observed in women with gestational trophoblastic disease (GTD) followed-up in a reference center (RC) by a multidisciplinary team.
Retrospective cohort study of the clinical records of 186 women with GTD and of the emotional aspects (EA) observed in these women by a teamof psychologists and reported by the 389 support groups conducted from 2014 to 2018.
The women were young (mean age: 31.2 years), 47% had no living child, 60% had planned the pregnancy, and 50% participated in two or more SG. Most women (n=137; 73.6%) reached spontaneous remission ofmolar gestation in a median time of 10 weeks and had a total follow-up time of seven months. In the group of 49 women (26.3%) who progressed to gestational trophoblastic neoplasia (GTN), time to remission after chemotherapy was 18 weeks, and total follow-up time was 36 months. EA included different levels of anxiety and depression,more evident in 9.1% of the women; these symptoms tended to occur more frequently in women older than 40 years (p=0.067), less educated (p=0.054), and whose disease progressed to GTN (p=0.018), as well as in those who had to undergo multi-agent chemotherapy (p=0.028) or hysterectomy (p=0.001) adjuvant to clinical treatment.
This study found several EA in association with all types of GTD. It also highlights the importance of specialized care only found in a RC, essential to support the recovery of the mental health of these women.
Summary
Rev Bras Ginecol Obstet. 2023;45(6):356-367
Summary
Rev Bras Ginecol Obstet. 2023;45(6):356-367
Summary
Rev Bras Ginecol Obstet. 2023;45(7):384-392
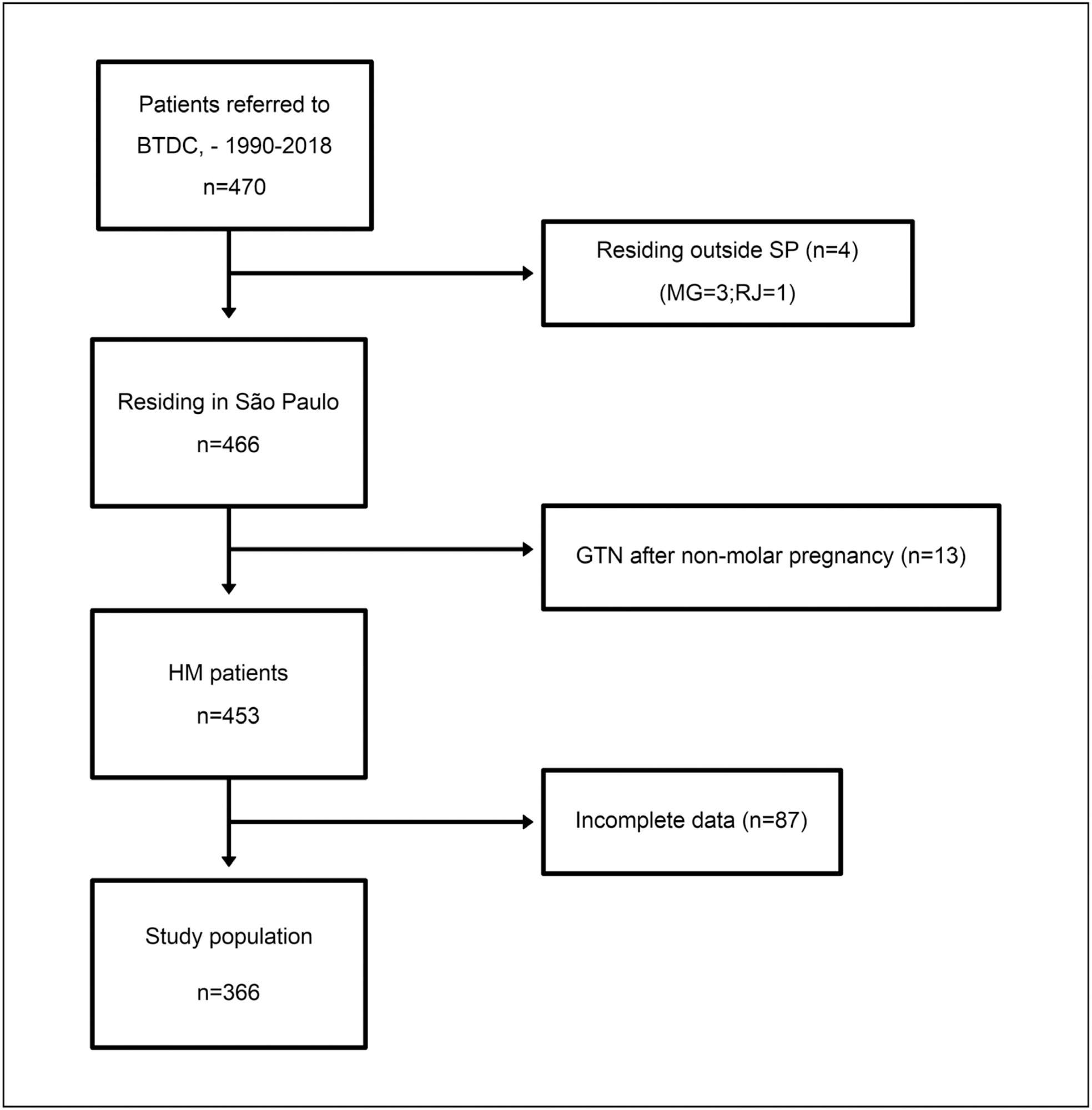
To assess the potential relationship of clinical status upon admission and distance traveled from geographical health district in women with gestational trophoblastic disease (GTD).
This is a cross-sectional study including women with GTD from the 17 health districts from the São Paulo state (I–XVII), Brazil, referred to the Botucatu Trophoblastic Disease Center (specialized center, district VI), between 1990 and 2018. At admission, hydatidiform mole was assessed according to the risk score system of Berkowitz et al. Gestational trophoblastic neoplasia was evaluated using the International Federation of Gynecology and Obstetrics / World Health Organization (FIGO/WHO) staging/risk score. Data on demographics, clinical status and distance traveled were collected. Multiple regression analyses were performed.
This study included 366 women (335 hydatidiform mole, 31 gestational trophoblastic neoplasia). The clinical status at admission and distance traveled significantly differed between the specialized center district and other districts. Patients referred from health districts IX (β = 2.38 [0.87–3.88], p = 0.002) and XVI (β = 0.78 [0.02–1.55], p = 0.045) had higher hydatidiform mole scores than those from the specialized center district. Gestational trophoblastic neoplasia patients from district XVI showed a 3.32 increase in FIGO risk scores compared with those from the specialized center area (β = 3.32, 95% CI = 0.78–5.87, p = 0.010). Distance traveled by patients from districts IX (200km) and XVI (203.5km) was significantly longer than that traveled by patients from the specialized center district (76km).
Patients from health districts outside the specialized center area had higher risk scores for both hydatidiform mole and gestational trophoblastic neoplasia at admission. Long distances (>80 km) seemed to adversely influence gestational trophoblastic disease clinical status at admission, indicating barriers to accessing specialized centers.
Summary
Rev Bras Ginecol Obstet. 2023;45(7):384-392
To assess the potential relationship of clinical status upon admission and distance traveled from geographical health district in women with gestational trophoblastic disease (GTD).
This is a cross-sectional study including women with GTD from the 17 health districts from the São Paulo state (I–XVII), Brazil, referred to the Botucatu Trophoblastic Disease Center (specialized center, district VI), between 1990 and 2018. At admission, hydatidiform mole was assessed according to the risk score system of Berkowitz et al. Gestational trophoblastic neoplasia was evaluated using the International Federation of Gynecology and Obstetrics / World Health Organization (FIGO/WHO) staging/risk score. Data on demographics, clinical status and distance traveled were collected. Multiple regression analyses were performed.
This study included 366 women (335 hydatidiform mole, 31 gestational trophoblastic neoplasia). The clinical status at admission and distance traveled significantly differed between the specialized center district and other districts. Patients referred from health districts IX (β = 2.38 [0.87–3.88], p = 0.002) and XVI (β = 0.78 [0.02–1.55], p = 0.045) had higher hydatidiform mole scores than those from the specialized center district. Gestational trophoblastic neoplasia patients from district XVI showed a 3.32 increase in FIGO risk scores compared with those from the specialized center area (β = 3.32, 95% CI = 0.78–5.87, p = 0.010). Distance traveled by patients from districts IX (200km) and XVI (203.5km) was significantly longer than that traveled by patients from the specialized center district (76km).
Patients from health districts outside the specialized center area had higher risk scores for both hydatidiform mole and gestational trophoblastic neoplasia at admission. Long distances (>80 km) seemed to adversely influence gestational trophoblastic disease clinical status at admission, indicating barriers to accessing specialized centers.
Summary
Rev Bras Ginecol Obstet. 2015;37(1):42-51
DOI 10.1590/SO100-720320140005198
Gestational trophoblastic neoplasia (GTN) is the term to describe a set of malignant placental diseases, including invasive mole, choriocarcinoma, placental site trophoblastic tumor and epithelioid trophoblastic tumor. Both invasive mole and choriocarcinoma respond well to chemotherapy, and cure rates are greater than 90%. Since the advent of chemotherapy, low-risk GTN has been treated with a single agent, usually methotrexate or actinomycin D. Cases of high-risk GTN, however, should be treated with multiagent chemotherapy, and the regimen usually selected is EMA-CO, which combines etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine. This study reviews the literature about GTN to discuss current knowledge about its diagnosis and treatment.
Summary
Rev Bras Ginecol Obstet. 2015;37(1):42-51
DOI 10.1590/SO100-720320140005198
Gestational trophoblastic neoplasia (GTN) is the term to describe a set of malignant placental diseases, including invasive mole, choriocarcinoma, placental site trophoblastic tumor and epithelioid trophoblastic tumor. Both invasive mole and choriocarcinoma respond well to chemotherapy, and cure rates are greater than 90%. Since the advent of chemotherapy, low-risk GTN has been treated with a single agent, usually methotrexate or actinomycin D. Cases of high-risk GTN, however, should be treated with multiagent chemotherapy, and the regimen usually selected is EMA-CO, which combines etoposide, methotrexate, actinomycin D, cyclophosphamide and vincristine. This study reviews the literature about GTN to discuss current knowledge about its diagnosis and treatment.