Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(6):369-370
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(6):369-370
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(4):369-375
To compare the oocyte maturation rate in the treatment of in vitro fertilization (IVF) in terms of the use of human chorionic gonadotropin (hCG), agonist gonadotropin-releasing hormone (GnRH) and dual trigger and to evaluate the associated risk factors for sub-optimal maturation rates.
A retrospective cohort study with 856 women who underwent IVF. They performed oocyte retrieval and were classified into 3 groups (1 - hCG, 2 - GnRHagonist, 3 - dual trigger). The primary outcome was maturation rate per trigger, and the secondary outcomes were the pregnancy rate per oocyte retrieval and the correlations between low maturation rate as well as the clinical and treatment characteristics of women.
The maturation rate was 77% in group 1; 76% in group 2, and 83% in group 3 (p=0.003). Group 2 showed women with better ovarian reserve, greater number of oocytes collected, and more mature oocytes and embryos compared with the other groups (p<0.001). The cumulative clinical pregnancy rate was no different between the groups (p=0.755). Low ovarian reserve and low doses of follicle-stimulating hormone (FSH) administered during the stimulus were associated with a higher chance of null maturation rate.
The oocyte maturation rates and IVF results were similar in all groups. Low ovarian reserve is associated with the worst treatment results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2022;44(4):369-375
To compare the oocyte maturation rate in the treatment of in vitro fertilization (IVF) in terms of the use of human chorionic gonadotropin (hCG), agonist gonadotropin-releasing hormone (GnRH) and dual trigger and to evaluate the associated risk factors for sub-optimal maturation rates.
A retrospective cohort study with 856 women who underwent IVF. They performed oocyte retrieval and were classified into 3 groups (1 - hCG, 2 - GnRHagonist, 3 - dual trigger). The primary outcome was maturation rate per trigger, and the secondary outcomes were the pregnancy rate per oocyte retrieval and the correlations between low maturation rate as well as the clinical and treatment characteristics of women.
The maturation rate was 77% in group 1; 76% in group 2, and 83% in group 3 (p=0.003). Group 2 showed women with better ovarian reserve, greater number of oocytes collected, and more mature oocytes and embryos compared with the other groups (p<0.001). The cumulative clinical pregnancy rate was no different between the groups (p=0.755). Low ovarian reserve and low doses of follicle-stimulating hormone (FSH) administered during the stimulus were associated with a higher chance of null maturation rate.
The oocyte maturation rates and IVF results were similar in all groups. Low ovarian reserve is associated with the worst treatment results.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(7):369-370
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(7):369-370
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(1):37-43
DOI 10.1590/S0100-72032002000100006
Purpose: to determine the factors associated with the detection of a microinvasive carcinoma in the cervical cone of women with a previous colposcopically directed biopsy compatible with cervical intraepithelial neoplasia (CIN) 3 and to evaluate the proportion of involved margins. Patients and methods: we reviewed the medical records of 385 women (mean age: 39 years) submitted to cold conization or conization by high frequency surgery (HFS) with a loop during the period from January 1993 to July 2000. These procedures were indicated on the basis of a biopsy compatible with (CIN) 3. Results: the diagnosis of the cone was compatible with (CIN) 3 in 243 (63%) women and with (CIN) 2 in 13 (3%). Only 10 presented HPV/CIN 1 (3%) and eight had no residual disease in the cone. However, 101 (26%) women presented a microinvasive carcinoma in the cone and 10 (3%) presented a frankly invasive carcinoma. Age, menstrual status and number of deliveries were not related to the severity of the cone lesion. Women with oncologic colpocytology changes suggestive of invasion presented a significantly higher risk of having a microinvasive or invasive carcinoma as determined by final histology (p<0.01), although 52 of the 243 women with CIN 2 or CIN 3 in the cone also showed a suggestion of invasion at colpocytology. Among the women with CIN 2 or 3, the epithelium was white in 44%, dotted in 21%, and mosaic-like in 17%. This proportion was similar for women with a microinvasive or invasive carcinoma, with these images being detected in 37%, 23% and 21% of the cases, respectively. Involvement of the cone margins was significantly higher among women submitted to HFS (49%) than among those submitted to cold conization (29%). Conclusion: the absence of independent clinical and colposcopic factors associated with the detection of a microinvasive carcinoma in women submitted to conization on the basis of a biopsy compatible with (CIN) 3 justifies the conical excision of the squamocolumnar junction in high grade cervical lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(1):37-43
DOI 10.1590/S0100-72032002000100006
Purpose: to determine the factors associated with the detection of a microinvasive carcinoma in the cervical cone of women with a previous colposcopically directed biopsy compatible with cervical intraepithelial neoplasia (CIN) 3 and to evaluate the proportion of involved margins. Patients and methods: we reviewed the medical records of 385 women (mean age: 39 years) submitted to cold conization or conization by high frequency surgery (HFS) with a loop during the period from January 1993 to July 2000. These procedures were indicated on the basis of a biopsy compatible with (CIN) 3. Results: the diagnosis of the cone was compatible with (CIN) 3 in 243 (63%) women and with (CIN) 2 in 13 (3%). Only 10 presented HPV/CIN 1 (3%) and eight had no residual disease in the cone. However, 101 (26%) women presented a microinvasive carcinoma in the cone and 10 (3%) presented a frankly invasive carcinoma. Age, menstrual status and number of deliveries were not related to the severity of the cone lesion. Women with oncologic colpocytology changes suggestive of invasion presented a significantly higher risk of having a microinvasive or invasive carcinoma as determined by final histology (p<0.01), although 52 of the 243 women with CIN 2 or CIN 3 in the cone also showed a suggestion of invasion at colpocytology. Among the women with CIN 2 or 3, the epithelium was white in 44%, dotted in 21%, and mosaic-like in 17%. This proportion was similar for women with a microinvasive or invasive carcinoma, with these images being detected in 37%, 23% and 21% of the cases, respectively. Involvement of the cone margins was significantly higher among women submitted to HFS (49%) than among those submitted to cold conization (29%). Conclusion: the absence of independent clinical and colposcopic factors associated with the detection of a microinvasive carcinoma in women submitted to conization on the basis of a biopsy compatible with (CIN) 3 justifies the conical excision of the squamocolumnar junction in high grade cervical lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(1):37-42
DOI 10.1590/S0100-72032011000100006
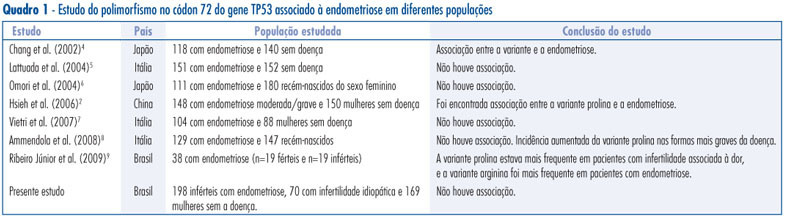
PURPOSE: to evaluate the frequency of TP53 codon 72 polymorphism in infertile women with endometriosis, women with idiopathic infertility, controls and its relation to the disease. METHODS: a case-control study that included 198 infertile women with endometriosis, 70 women with idiopathic infertility and 169 fertile women without endometriosis as control. Detection of TP53 codon 72 gene polymorphism (rs1042522, Arg/C:Pro/G), that promotes a C/G exchange in the coding region of the gene, was performed by real time Polymerase Chain Reaction (PCR), using the TaqMan system of primers, that flank the implicated region and probes labeled with different fluorescent dyes, one for allele C and other for allele G. When two dyes were observed, the patient was considered to be heterozygous CG. In the presence of only one dye, the individual was considered to be homozygous CC or GG. The χ2 test was used to compare allele and genotype frequencies between groups. All p-values were two-tailed and a p-value <0.05 was considered to be statistically significant. RESULTS: we found no statistically significant difference in the distribution of TP53 codon 72 polymorphism genotypes CC, CG or GG (p=0.7) and alleles C or G (p=0.4) between infertile patients with endometriosis and controls (p=0.4), regardless of the stage of the disease. In relation to infertility, no statistically significant difference in the genotype or allele distribution (p=1.0 and p=0.9, respectively) was observed between idiopathic infertile women and controls. Considering the dominant inheritance model, again, no statistically significant difference was found even in the endometriosis (p=0.5) or the idiopathic infertility group (p=0.9) when compared to controls. Regarding the recessive inheritance model no statistically significant difference was found, with p=0.6 and p=1.0, respectively, for the endometriosis and idiopathic infertility groups. CONCLUSION: the results suggest that the TP53 codon 72 polymorphism does not confer genetic susceptibility to endometriosis and/or infertility in the Brazilian population, not even the severe form of the disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(1):37-42
DOI 10.1590/S0100-72032011000100006
PURPOSE: to evaluate the frequency of TP53 codon 72 polymorphism in infertile women with endometriosis, women with idiopathic infertility, controls and its relation to the disease. METHODS: a case-control study that included 198 infertile women with endometriosis, 70 women with idiopathic infertility and 169 fertile women without endometriosis as control. Detection of TP53 codon 72 gene polymorphism (rs1042522, Arg/C:Pro/G), that promotes a C/G exchange in the coding region of the gene, was performed by real time Polymerase Chain Reaction (PCR), using the TaqMan system of primers, that flank the implicated region and probes labeled with different fluorescent dyes, one for allele C and other for allele G. When two dyes were observed, the patient was considered to be heterozygous CG. In the presence of only one dye, the individual was considered to be homozygous CC or GG. The χ2 test was used to compare allele and genotype frequencies between groups. All p-values were two-tailed and a p-value <0.05 was considered to be statistically significant. RESULTS: we found no statistically significant difference in the distribution of TP53 codon 72 polymorphism genotypes CC, CG or GG (p=0.7) and alleles C or G (p=0.4) between infertile patients with endometriosis and controls (p=0.4), regardless of the stage of the disease. In relation to infertility, no statistically significant difference in the genotype or allele distribution (p=1.0 and p=0.9, respectively) was observed between idiopathic infertile women and controls. Considering the dominant inheritance model, again, no statistically significant difference was found even in the endometriosis (p=0.5) or the idiopathic infertility group (p=0.9) when compared to controls. Regarding the recessive inheritance model no statistically significant difference was found, with p=0.6 and p=1.0, respectively, for the endometriosis and idiopathic infertility groups. CONCLUSION: the results suggest that the TP53 codon 72 polymorphism does not confer genetic susceptibility to endometriosis and/or infertility in the Brazilian population, not even the severe form of the disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):37-43
DOI 10.1590/S0100-72032005000100008
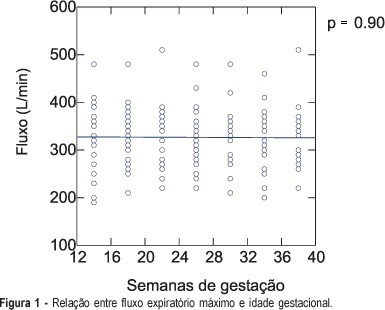
PURPOSE: to investigate the normal peak expiratory flow values in healthy pregnant women employing a portable expiratory apparatus (Mini-Wright Peak Flow Meter), and to relate the obtained measurements to each patient's height, body mass index (BMI) and age, along gestation. METHODS: a longitudinal prospective study including 26 pregnant women followed up from the first trimester to the 36th week of gestation and examined every four weeks. On the occasion of seven visits, the pregnant women performed forced exhaling into a portable expiratory apparatus three times, with the highest value being considered the peak expiratory flow. All measurements were made under the same investigator's supervision in order to reduce the margin of error. Pearson coefficient was used to calculate the correlation between flow and BMI, between flow and patient's height, and between flow and patient's age. RESULTS: the variation in flow values during pregnancy can be determined by flow = 328.32 -0.07 x week, with a Pearson coefficient equal to zero. To determine whether there was a difference in the correlation coefficients between BMI and flow, we compared the lowest coefficient (0.47 for week 30, flow = 123.49 + 7.64 x BMI) with the highest coefficient (0.59 for week 34, flow = 87.77 + 9.05 x BMI) of each studied time interval and obtained a value of 0.22, indicating a good correlation between the flow and BMI variables. There was a positive correlation between height and flow (Pearson = 0.61), with flow = -477.47 + 497.38 x height. The correlation coefficient between flow and age was 0.24, with the equation obtained in this case being non-linear. CONCLUSIONS: peak expiratory flow values did not change along gestation. Higher flows were observed in taller women. Pregnant women with a higher BMI before gestation presented higher flows. There was no correlation between flow and maternal age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2005;27(1):37-43
DOI 10.1590/S0100-72032005000100008
PURPOSE: to investigate the normal peak expiratory flow values in healthy pregnant women employing a portable expiratory apparatus (Mini-Wright Peak Flow Meter), and to relate the obtained measurements to each patient's height, body mass index (BMI) and age, along gestation. METHODS: a longitudinal prospective study including 26 pregnant women followed up from the first trimester to the 36th week of gestation and examined every four weeks. On the occasion of seven visits, the pregnant women performed forced exhaling into a portable expiratory apparatus three times, with the highest value being considered the peak expiratory flow. All measurements were made under the same investigator's supervision in order to reduce the margin of error. Pearson coefficient was used to calculate the correlation between flow and BMI, between flow and patient's height, and between flow and patient's age. RESULTS: the variation in flow values during pregnancy can be determined by flow = 328.32 -0.07 x week, with a Pearson coefficient equal to zero. To determine whether there was a difference in the correlation coefficients between BMI and flow, we compared the lowest coefficient (0.47 for week 30, flow = 123.49 + 7.64 x BMI) with the highest coefficient (0.59 for week 34, flow = 87.77 + 9.05 x BMI) of each studied time interval and obtained a value of 0.22, indicating a good correlation between the flow and BMI variables. There was a positive correlation between height and flow (Pearson = 0.61), with flow = -477.47 + 497.38 x height. The correlation coefficient between flow and age was 0.24, with the equation obtained in this case being non-linear. CONCLUSIONS: peak expiratory flow values did not change along gestation. Higher flows were observed in taller women. Pregnant women with a higher BMI before gestation presented higher flows. There was no correlation between flow and maternal age.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(1):37-42
DOI 10.1590/S0100-72032004000100006
PURPOSE: to evaluate the accuracy of directional vacuum-assisted biopsy (mammotomy), guided by ultrasonography, in the diagnosis of nonpalpable breast lesion, as compared with excision biopsy, and to evaluate the therapeutic value of mammotomy in nonpalpable benign lesions. METHODS: 114 patients, who presented nonpalpable breast lesion, visible on ultrasonography, were included. The patients were referred to complementary ultrasonographic evaluation due to mastalgia or earlier found mammographic alteration. All were submitted to mammotomy guided by ultrasonography using Mammotome® (Biopsys, Irvine, Califórnia), with a 11 gauge needle. The excision biopsy was performed with previous puncture of those patients who presented residual lesion after the mammotomy, that is, 88 patients. To evaluate comparatively the mammotomy results with those of excision biopsy, the sensitivity and specificity rates, positive and negative predictive values, and the agreement proportion were calculated. Not only the sensibilities, but also the specificities and the agreement proportions of both examinations were compared through Wald statistics, using a model for classified data. RESULTS: of 114 patients, 88 were submitted to excision biopsy. The remaining 26 did not show post-mammotomy lesions visible on ultrasonography, and for one year they were without alterations on the bi-annual mammographic and ultrasonographic examinations. The diameter of those lesions was less than 1.5 cm. Among the 88 patients that underwent excision biopsy, 69 (78,4%) showed benign and 19 (21,6%), malignant lesions. Mammotomy diagnosed 16 of the malignant lesions, with three false-negative and no false-positive results. The false results occurred in the first cases, showing the existence of a learning curve of the method, or due to technical difficulty such as the blurring of ultrasonographic image by bleeding. The sensitivity and specificity were 84,2% and 100%, respectively, with 100% positive predictive and 95,8% predictive negative values. The mammotomy accuracy was 96,6%. Complications were rare: two cases of hematomas, none of them needing surgical drainage; a case of vasovagal reflex not allowing the conclusion of the examination. The cosmetic results were very favorable due to small incisions (3 mm) and to the smaller amount of excised tissue. CONCLUSION: mammotomy guided by ultrasonography showed to be a diagnostic method with high accuracy, and it may be used as therapy for benign, smaller than 1.5 cm lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2004;26(1):37-42
DOI 10.1590/S0100-72032004000100006
PURPOSE: to evaluate the accuracy of directional vacuum-assisted biopsy (mammotomy), guided by ultrasonography, in the diagnosis of nonpalpable breast lesion, as compared with excision biopsy, and to evaluate the therapeutic value of mammotomy in nonpalpable benign lesions. METHODS: 114 patients, who presented nonpalpable breast lesion, visible on ultrasonography, were included. The patients were referred to complementary ultrasonographic evaluation due to mastalgia or earlier found mammographic alteration. All were submitted to mammotomy guided by ultrasonography using Mammotome® (Biopsys, Irvine, Califórnia), with a 11 gauge needle. The excision biopsy was performed with previous puncture of those patients who presented residual lesion after the mammotomy, that is, 88 patients. To evaluate comparatively the mammotomy results with those of excision biopsy, the sensitivity and specificity rates, positive and negative predictive values, and the agreement proportion were calculated. Not only the sensibilities, but also the specificities and the agreement proportions of both examinations were compared through Wald statistics, using a model for classified data. RESULTS: of 114 patients, 88 were submitted to excision biopsy. The remaining 26 did not show post-mammotomy lesions visible on ultrasonography, and for one year they were without alterations on the bi-annual mammographic and ultrasonographic examinations. The diameter of those lesions was less than 1.5 cm. Among the 88 patients that underwent excision biopsy, 69 (78,4%) showed benign and 19 (21,6%), malignant lesions. Mammotomy diagnosed 16 of the malignant lesions, with three false-negative and no false-positive results. The false results occurred in the first cases, showing the existence of a learning curve of the method, or due to technical difficulty such as the blurring of ultrasonographic image by bleeding. The sensitivity and specificity were 84,2% and 100%, respectively, with 100% positive predictive and 95,8% predictive negative values. The mammotomy accuracy was 96,6%. Complications were rare: two cases of hematomas, none of them needing surgical drainage; a case of vasovagal reflex not allowing the conclusion of the examination. The cosmetic results were very favorable due to small incisions (3 mm) and to the smaller amount of excised tissue. CONCLUSION: mammotomy guided by ultrasonography showed to be a diagnostic method with high accuracy, and it may be used as therapy for benign, smaller than 1.5 cm lesions.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(1):37-41
DOI 10.1590/S0100-72032000000100007
Purpose: to evaluate the effects of tibolone on climacteric symptoms and clinical and metabolic variables. Methods: thirty-four postmenopausal women were treated orally with 2.5 mg tibolone daily for 48 weeks and evaluated as to climacteric complaints, clinical aspects such as weight and blood pressure and lipid profile (total cholesterol, HDL-c, LDL-c, VLDL-c and triglycerides). Results: a significant improvement of climacteric complaints was demonstrated by a significant decrease in the Kupperman index (p<0.001) and the mean number of hot flushes (p<0.001) from the first month of treatment onwards. There was a significant decrease in total cholesterol, triglycerides and VLDL-c (p<0.001). The LDL-c levels presented a slight decrease (not significant). The HDL-c levels showed a significant decrease at week 24. However these levels returned to baseline levels at week 48. With regard to the vital signs no change in body weight and blood pressure was measured. The side effects were mild and temporary, vaginal bleeding, nausea and edema being the most common. Conclusion: tibolone may be considered a safe and efficient option to treat climacteric symptoms in postmenopausal women without significant impact on lipid profile.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(1):37-41
DOI 10.1590/S0100-72032000000100007
Purpose: to evaluate the effects of tibolone on climacteric symptoms and clinical and metabolic variables. Methods: thirty-four postmenopausal women were treated orally with 2.5 mg tibolone daily for 48 weeks and evaluated as to climacteric complaints, clinical aspects such as weight and blood pressure and lipid profile (total cholesterol, HDL-c, LDL-c, VLDL-c and triglycerides). Results: a significant improvement of climacteric complaints was demonstrated by a significant decrease in the Kupperman index (p<0.001) and the mean number of hot flushes (p<0.001) from the first month of treatment onwards. There was a significant decrease in total cholesterol, triglycerides and VLDL-c (p<0.001). The LDL-c levels presented a slight decrease (not significant). The HDL-c levels showed a significant decrease at week 24. However these levels returned to baseline levels at week 48. With regard to the vital signs no change in body weight and blood pressure was measured. The side effects were mild and temporary, vaginal bleeding, nausea and edema being the most common. Conclusion: tibolone may be considered a safe and efficient option to treat climacteric symptoms in postmenopausal women without significant impact on lipid profile.