Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(1):35-40
To evaluate the variability of three-dimensional automatic counts of ovarian follicles measuring 2-6 to 2-10 mm during the menstrual cycle and to determine if this test can be applied outside the early follicular phase of the menstrual cycle.
in a prospective observational study, serial transvaginal ultrasound scans were performed from April 20, 2013, to October 30, 2014, on infertile patients. Inclusion criteria: age between 18 and 35 years, BMI 18-25 kg/m2, regular menstrual cycles, no history of ovarian surgery and no hormonal changes in TSH, prolactin, fasting insulin or glucose. We excluded patients with ovarian cysts or who did not complete one or more days of the serial transvaginal ultrasound scans. The follicle count was performed in 3D mode ultrasound with a Sono AVC system. Visits were scheduled for the early follicular, mid-follicular, periovulatory and luteal phases of the menstrual cycle.
Forty-five women were included. The Friedman test showed that the total number of follicles measuring 2-6 mmvaried significantly (p = 0.001) across the four periods of the menstrual cycle. The Paired Student t-test showed a significant increase in 2-6 mm follicle count from the mid-follicular and periovulatory phase to the luteal phase. We found no significant intra-cycle variation between the small follicles (2-6 mm) in the early follicular, mid-follicular and periovulatory phases. The Friedman test showed that the total number of follicles measuring 2-10 mm varied significantly (p = 0.003) across the menstrual cycle.
The variation of three-dimensional automatic counts of 2-6 mm follicles in the early follicular, mid-follicular and periovulatory phases was not statistically significant. The significant variability in the counts of follicles measuring 2-10 mm across the menstrual cycle does not permit this examination to be performed side the early follicular phase.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(1):35-40
To evaluate the variability of three-dimensional automatic counts of ovarian follicles measuring 2-6 to 2-10 mm during the menstrual cycle and to determine if this test can be applied outside the early follicular phase of the menstrual cycle.
in a prospective observational study, serial transvaginal ultrasound scans were performed from April 20, 2013, to October 30, 2014, on infertile patients. Inclusion criteria: age between 18 and 35 years, BMI 18-25 kg/m2, regular menstrual cycles, no history of ovarian surgery and no hormonal changes in TSH, prolactin, fasting insulin or glucose. We excluded patients with ovarian cysts or who did not complete one or more days of the serial transvaginal ultrasound scans. The follicle count was performed in 3D mode ultrasound with a Sono AVC system. Visits were scheduled for the early follicular, mid-follicular, periovulatory and luteal phases of the menstrual cycle.
Forty-five women were included. The Friedman test showed that the total number of follicles measuring 2-6 mmvaried significantly (p = 0.001) across the four periods of the menstrual cycle. The Paired Student t-test showed a significant increase in 2-6 mm follicle count from the mid-follicular and periovulatory phase to the luteal phase. We found no significant intra-cycle variation between the small follicles (2-6 mm) in the early follicular, mid-follicular and periovulatory phases. The Friedman test showed that the total number of follicles measuring 2-10 mm varied significantly (p = 0.003) across the menstrual cycle.
The variation of three-dimensional automatic counts of 2-6 mm follicles in the early follicular, mid-follicular and periovulatory phases was not statistically significant. The significant variability in the counts of follicles measuring 2-10 mm across the menstrual cycle does not permit this examination to be performed side the early follicular phase.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(1):35-40
DOI 10.1590/S0100-72032003000100006
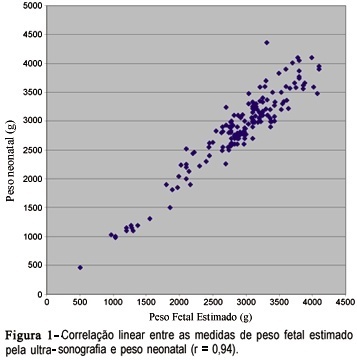
PURPOSE: tocompare the ultrasound estimation of fetal weight (EFW) with neonatal weight and to evaluate the performance of the normal EFW curve according to gestational age for the diagnosis of fetal/neonatal weight deviation and associated factors. METHODS: one hundred and eighty-six pregnant women who delivered at the institution from November 1998 to January 2000 and who had one ultra-sonographic evaluation performed until three days prior to delivery with estimation of the amniotic fluid index were included. EFW was calculated and classified in to small for gestational age (SGA), adequate for gestational age (AGA) and large for gestational age (LGA) through the normal EFW curve for this population. Neonatal weight was similarly classified. The variability of the measures and the degree of linear correlation between EFW and neonatal weight, as well as sensitivity, specificity and predictive values for the use of the normal EFW curve in the diagnosis of neonatal weight deviations were calculated. RESULTS: the difference between EFW and neonatal weight ranged from -540 to +594 g, with a mean of +46.9 g, and the two measures presented a linear correlation coefficient of 0.94. The normal EFW curve had a sensitivity of 100% and specificity of 90.5% in detecting SGA neonates and of 94.4 and 92.8%, respectively, in detecting LGA; however, the predictive positive values were low for both conditions. CONCLUSIONS:ultrasound EFW was in agreement with the neonatal weight, with a mean overweight of approximately 47 g, and its normal curve showed a good performance in the screening of SGA and LGA neonates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2003;25(1):35-40
DOI 10.1590/S0100-72032003000100006
PURPOSE: tocompare the ultrasound estimation of fetal weight (EFW) with neonatal weight and to evaluate the performance of the normal EFW curve according to gestational age for the diagnosis of fetal/neonatal weight deviation and associated factors. METHODS: one hundred and eighty-six pregnant women who delivered at the institution from November 1998 to January 2000 and who had one ultra-sonographic evaluation performed until three days prior to delivery with estimation of the amniotic fluid index were included. EFW was calculated and classified in to small for gestational age (SGA), adequate for gestational age (AGA) and large for gestational age (LGA) through the normal EFW curve for this population. Neonatal weight was similarly classified. The variability of the measures and the degree of linear correlation between EFW and neonatal weight, as well as sensitivity, specificity and predictive values for the use of the normal EFW curve in the diagnosis of neonatal weight deviations were calculated. RESULTS: the difference between EFW and neonatal weight ranged from -540 to +594 g, with a mean of +46.9 g, and the two measures presented a linear correlation coefficient of 0.94. The normal EFW curve had a sensitivity of 100% and specificity of 90.5% in detecting SGA neonates and of 94.4 and 92.8%, respectively, in detecting LGA; however, the predictive positive values were low for both conditions. CONCLUSIONS:ultrasound EFW was in agreement with the neonatal weight, with a mean overweight of approximately 47 g, and its normal curve showed a good performance in the screening of SGA and LGA neonates.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(1):35-40
DOI 10.1590/S0100-72032009000100007
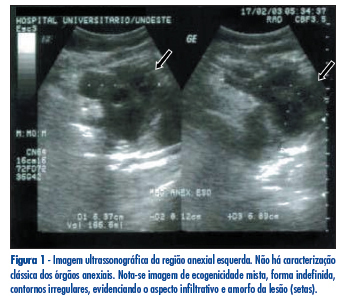
Desmoid tumor is a noncapsulated neoplasia, locally aggressive, originated from the fibroblasts of the musculo-aponeurotic tissues. Even though with no malignant behavior, such as the ability of generating metastasis or of invasion, the desmoid tumor has a high tendency for local growth, causing deformities in the adjacent organs, pain and sometimes organ dysfunction, depending on the area involved. We report the case of a large intra-abdominal desmoid tumor, invading pelvic organs in a 53 year-old patient. The neoplasia has been totally extirpated and, at the moment, five years after the surgery, the patient presents no clinical or radiologic sign of lesion relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2009;31(1):35-40
DOI 10.1590/S0100-72032009000100007
Desmoid tumor is a noncapsulated neoplasia, locally aggressive, originated from the fibroblasts of the musculo-aponeurotic tissues. Even though with no malignant behavior, such as the ability of generating metastasis or of invasion, the desmoid tumor has a high tendency for local growth, causing deformities in the adjacent organs, pain and sometimes organ dysfunction, depending on the area involved. We report the case of a large intra-abdominal desmoid tumor, invading pelvic organs in a 53 year-old patient. The neoplasia has been totally extirpated and, at the moment, five years after the surgery, the patient presents no clinical or radiologic sign of lesion relapse.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(1):35-42
To evaluate the outcomes of surgical treatment in patients with chemoradiotherapy (CRT)-resistant and locally advanced cervical cancer (LACC).
Patients with LACC who underwent surgery due to resistance to CRT between 2005 and 2015 were reviewed retrospectively. Disease-free survival (DFS) and overall survival (OS) related factors were analyzed.
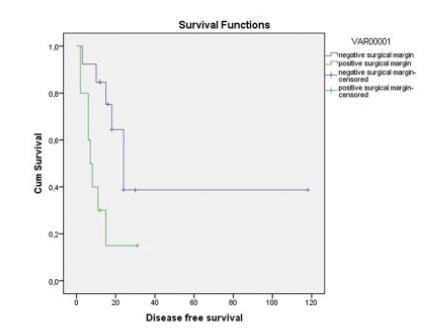
A total of 23 patients were included in the study and the median age was 51 years old. A total of 14 patients (60.8%) experienced recurrence; among these recurrences, 8 of them were local, 5 were distant, 1 was both distant and local. A total of 9 patients (39%) died. The Median DFS and OS durations were 15 and 32 months, respectively. A total of 17 patients (74%) had undergone simple hysterectomy, 4 (17%) radical hysterectomy, and 2 (9%) total pelvic exenteration. Postoperative grade 3 and 4 complications were seen in 12 patients (52%). Macroscopic tumor presence in the pathology specimen was associated with distant recurrence and positive surgical margins with local recurrence (Log-Rank test p = 0.029 and p = 0.048, respectively). The only factor associated with OS was surgical margin positivity (Log-Rank test p = 0.008). The type of surgery, grades 3 and 4 postoperative complications, brachytherapy, and tumor histology were not associated with recurrence.
In patients with LACC, hysterectomy is an option in the presence of a central residual tumor after CRT. However, the risk of grades 3 and 4 complications of performed surgery is high. The presence of macroscopic tumor in the pathology specimen and positive surgical margins are poor prognostic factors. The goal of the surgeon should be to achieve a negative surgical margin. It does not seem important if the surgery is simple or radical.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2020;42(1):35-42
To evaluate the outcomes of surgical treatment in patients with chemoradiotherapy (CRT)-resistant and locally advanced cervical cancer (LACC).
Patients with LACC who underwent surgery due to resistance to CRT between 2005 and 2015 were reviewed retrospectively. Disease-free survival (DFS) and overall survival (OS) related factors were analyzed.
A total of 23 patients were included in the study and the median age was 51 years old. A total of 14 patients (60.8%) experienced recurrence; among these recurrences, 8 of them were local, 5 were distant, 1 was both distant and local. A total of 9 patients (39%) died. The Median DFS and OS durations were 15 and 32 months, respectively. A total of 17 patients (74%) had undergone simple hysterectomy, 4 (17%) radical hysterectomy, and 2 (9%) total pelvic exenteration. Postoperative grade 3 and 4 complications were seen in 12 patients (52%). Macroscopic tumor presence in the pathology specimen was associated with distant recurrence and positive surgical margins with local recurrence (Log-Rank test p = 0.029 and p = 0.048, respectively). The only factor associated with OS was surgical margin positivity (Log-Rank test p = 0.008). The type of surgery, grades 3 and 4 postoperative complications, brachytherapy, and tumor histology were not associated with recurrence.
In patients with LACC, hysterectomy is an option in the presence of a central residual tumor after CRT. However, the risk of grades 3 and 4 complications of performed surgery is high. The presence of macroscopic tumor in the pathology specimen and positive surgical margins are poor prognostic factors. The goal of the surgeon should be to achieve a negative surgical margin. It does not seem important if the surgery is simple or radical.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(1):35-39
Robotic surgeries for cervical cancer have several advantages compared with lapa-rotomic or laparoscopic surgeries. Robotic single-site surgery has many advantages compared with the multiport approach, but its safety and feasibility are not established in radical oncologic surgeries. We report a case of a Federation of Gynecology and Obstetrics (FIGO) stage IB1 cervical carcinoma whose radical hysterectomy, sentinel lymph node mapping, and lymph node dissection were entirely performed by robotic single-site approach. The patient recovered very well, and was discharged from the hospital within 24 hours.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2017;39(1):35-39
Robotic surgeries for cervical cancer have several advantages compared with lapa-rotomic or laparoscopic surgeries. Robotic single-site surgery has many advantages compared with the multiport approach, but its safety and feasibility are not established in radical oncologic surgeries. We report a case of a Federation of Gynecology and Obstetrics (FIGO) stage IB1 cervical carcinoma whose radical hysterectomy, sentinel lymph node mapping, and lymph node dissection were entirely performed by robotic single-site approach. The patient recovered very well, and was discharged from the hospital within 24 hours.

Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):35-40
To evaluate the presence of residual disease in the uterine specimen after hysteroscopic polypectomy or polyp biopsy in patients with endometrioid endometrial cancer (EC).
We analyzed a series of 104 patients (92 cases from the Hospital AC Camargo and 12 from the Hospital do Servidor Público Estadual de São Paulo) with polyps that were diagnosed by hysteroscopy, showing endometrioid EC associated with the polyp or in the final pathological specimen. Patients underwent a surgical approach for endometrial cancer from January 2002 to January 2017. Their clinical and pathological data were retrospectively retrieved from the medical records.
In78cases (75%), thepolyphad EC, and in 40(38.5%), itwas restricted tothe polyp, without endometrial involvement. The pathologic stage was IA in 96 cases (92.3%) and 90 (86.5%) had histologic grade 1 or 2. In 18 cases (17.3%), there was no residual disease in the final uterine specimen, but only in 9 of them the hysteroscopy suggested that the tumor was restricted to the polyp. In 5 cases (4.8%) from the group without outside of the polyp during hysteroscopy, myometrial invasion was noted in the final uterine specimen. This finding suggests the possibility of disease extrapolation through the base of the polyp.
Patients with endometrioid EC associated with polyps may have the tumor completely removed during hysteroscopy, but the variables shown in the present study could not safely predict which patient would have no residual disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2021;43(1):35-40
To evaluate the presence of residual disease in the uterine specimen after hysteroscopic polypectomy or polyp biopsy in patients with endometrioid endometrial cancer (EC).
We analyzed a series of 104 patients (92 cases from the Hospital AC Camargo and 12 from the Hospital do Servidor Público Estadual de São Paulo) with polyps that were diagnosed by hysteroscopy, showing endometrioid EC associated with the polyp or in the final pathological specimen. Patients underwent a surgical approach for endometrial cancer from January 2002 to January 2017. Their clinical and pathological data were retrospectively retrieved from the medical records.
In78cases (75%), thepolyphad EC, and in 40(38.5%), itwas restricted tothe polyp, without endometrial involvement. The pathologic stage was IA in 96 cases (92.3%) and 90 (86.5%) had histologic grade 1 or 2. In 18 cases (17.3%), there was no residual disease in the final uterine specimen, but only in 9 of them the hysteroscopy suggested that the tumor was restricted to the polyp. In 5 cases (4.8%) from the group without outside of the polyp during hysteroscopy, myometrial invasion was noted in the final uterine specimen. This finding suggests the possibility of disease extrapolation through the base of the polyp.
Patients with endometrioid EC associated with polyps may have the tumor completely removed during hysteroscopy, but the variables shown in the present study could not safely predict which patient would have no residual disease.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(6):350-356
DOI 10.1590/S0100-72031998000600008
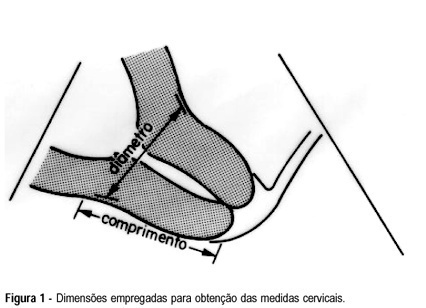
Objective: to evaluate the uterine cervix by digital and transvaginal ultrasound examinations in pregnant women at high risk of having premature delivery. Methods: during the period between February 1995 and September 1997, 38 pregnant women at high risk of having premature delivery between the 20th and 36th week of gestation were examined. These patients were submitted weekly to both digital and transvaginal ultrasound examinations. The digital examination evaluated the uterine cervix using two parameters: length and dilation. The transvaginal ultrasound studied the length and the anteroposterior diameter of the uterine cervix. The behavior of these cervical measurements was analyzed throughout the pregnancies. The two methods were compared regarding cervical evaluation and accuracy of premature birth diagnosis. Results: the rate of premature deliveries was 18.4% (7/38). Digital examination resulted in cervical evaluations with variation coefficients of 30.3% for length and 193% for dilation. Transvaginal ultrasound resulted in cervical evaluations with variation coefficients of 14.7% and 26.5% for the anteroposterior diameter and length, respectively. The cervical length measures obtained on ultrasound were always greater than those obtained on digital examination. Through analysis with the hypothesis test, an indirect relationship was observed between the cervical length and the gestational period for digital examination and ultrasound study (p<0.05 and p<0.01, respectively), and a direct relationship between the cervical dilation and the gestational age observed on the digital examination (p<0.01). Conclusions: among the parameters studied by means of the digital and transvaginal ultrasound examinations, the ultrasound cervical length presented the best accuracy in the diagnosis of premature birth, proving to be more reliable for the evaluation of cervical alterations in pregnant women at high risk of premature delivery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 1998;20(6):350-356
DOI 10.1590/S0100-72031998000600008
Objective: to evaluate the uterine cervix by digital and transvaginal ultrasound examinations in pregnant women at high risk of having premature delivery. Methods: during the period between February 1995 and September 1997, 38 pregnant women at high risk of having premature delivery between the 20th and 36th week of gestation were examined. These patients were submitted weekly to both digital and transvaginal ultrasound examinations. The digital examination evaluated the uterine cervix using two parameters: length and dilation. The transvaginal ultrasound studied the length and the anteroposterior diameter of the uterine cervix. The behavior of these cervical measurements was analyzed throughout the pregnancies. The two methods were compared regarding cervical evaluation and accuracy of premature birth diagnosis. Results: the rate of premature deliveries was 18.4% (7/38). Digital examination resulted in cervical evaluations with variation coefficients of 30.3% for length and 193% for dilation. Transvaginal ultrasound resulted in cervical evaluations with variation coefficients of 14.7% and 26.5% for the anteroposterior diameter and length, respectively. The cervical length measures obtained on ultrasound were always greater than those obtained on digital examination. Through analysis with the hypothesis test, an indirect relationship was observed between the cervical length and the gestational period for digital examination and ultrasound study (p<0.05 and p<0.01, respectively), and a direct relationship between the cervical dilation and the gestational age observed on the digital examination (p<0.01). Conclusions: among the parameters studied by means of the digital and transvaginal ultrasound examinations, the ultrasound cervical length presented the best accuracy in the diagnosis of premature birth, proving to be more reliable for the evaluation of cervical alterations in pregnant women at high risk of premature delivery.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(5):350-350
DOI 10.1590/S0100-72032002000500012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2002;24(5):350-350
DOI 10.1590/S0100-72032002000500012