Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(6):333-336
Isthmocele is a discontinuation of the myometrium at the uterine scar site in a patient with a previous cesarian section (CS). The cause of isthmocele appears to be multifactorial. Poor surgical technique, low incision location, uterine retroflection, obesity, smoking, inadequate healing of scars, and maternal age are possible related factors. Most patients with this condition are asymptomatic. However, women can present with postmenstrual bleeding, pelvic pain, subfertility, dysmenorrhea, infertility, and scar abscess. Brazil has one of the world s highest cesarean section rates. One of the consequences of the rising rate of CS is the isthmocele, an emerging female health problem. Here we report a case of mucinous cystadenoma arising in a uterine isthmocele, a complication, as far as we could investigate, not yet described in the literature.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2023;45(6):333-336
Isthmocele is a discontinuation of the myometrium at the uterine scar site in a patient with a previous cesarian section (CS). The cause of isthmocele appears to be multifactorial. Poor surgical technique, low incision location, uterine retroflection, obesity, smoking, inadequate healing of scars, and maternal age are possible related factors. Most patients with this condition are asymptomatic. However, women can present with postmenstrual bleeding, pelvic pain, subfertility, dysmenorrhea, infertility, and scar abscess. Brazil has one of the world s highest cesarean section rates. One of the consequences of the rising rate of CS is the isthmocele, an emerging female health problem. Here we report a case of mucinous cystadenoma arising in a uterine isthmocele, a complication, as far as we could investigate, not yet described in the literature.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):333-339
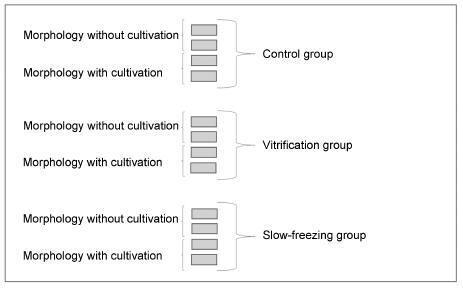
To assess the viability of bovine ovarian tissue after cryopreservation through either slow freezing or vitrification, and to compare it to that of control tissue by performing morphological analyses.
The study included 20 bovine ovarian cortex fragments that were divided into control, vitrification, and slow freezing groups. Each group consisted of four fragments of the same ovary, two fixed without cultivation, and two fixed with cultivation. Tissues were evaluated based on follicular morphology immediately after heating and after 7 days of culture, and compared with the control group.
A total of 240 fragments were analyzed, generating a sample of 1,344 follicles without cultivation and 552 with cultivation. When the non-cultivated samples were classified as non-atretic follicles, 572 were found in the control group, 289 in the vitrification group, and 373 in the slow freezing group, showing no significant differences. When classified as atretic, 46 follicles were found in the control group, 23 in the vitrification group, and 41 in the slow freezing group, also showing no statistical difference. In the post-culture sample, an evolution of the follicular stages could be observed. This finding was important to support that the follicles considered non-atretic in the non-cultivated group were actually viable in the morphological evaluation.
With no differences between the protocols, vitrification was shown to be an advanced and alternative method for patients who will undergo treatments that
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2016;38(7):333-339
To assess the viability of bovine ovarian tissue after cryopreservation through either slow freezing or vitrification, and to compare it to that of control tissue by performing morphological analyses.
The study included 20 bovine ovarian cortex fragments that were divided into control, vitrification, and slow freezing groups. Each group consisted of four fragments of the same ovary, two fixed without cultivation, and two fixed with cultivation. Tissues were evaluated based on follicular morphology immediately after heating and after 7 days of culture, and compared with the control group.
A total of 240 fragments were analyzed, generating a sample of 1,344 follicles without cultivation and 552 with cultivation. When the non-cultivated samples were classified as non-atretic follicles, 572 were found in the control group, 289 in the vitrification group, and 373 in the slow freezing group, showing no significant differences. When classified as atretic, 46 follicles were found in the control group, 23 in the vitrification group, and 41 in the slow freezing group, also showing no statistical difference. In the post-culture sample, an evolution of the follicular stages could be observed. This finding was important to support that the follicles considered non-atretic in the non-cultivated group were actually viable in the morphological evaluation.
With no differences between the protocols, vitrification was shown to be an advanced and alternative method for patients who will undergo treatments that
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(7):333-338
DOI 10.1590/S0100-720320150005373
To describe the prevalence of malformations found in fetuses with trisomy of chromosomes 13, 18 and 21 by identifying the most frequent within each condition.
A retrospective cross-sectional study with the analysis of trisomy cases of chromosomes 13, 18 and 21 diagnosed through fetal karyotype obtained by amniocentesis/cordocentesis, between October 1994 and May 2014, at a Teaching Hospital in Brazil Southern Region. Malformations identified through morphological ultrasonography were described and, subsequently, confirmed in newborn examinations and/or fetal autopsy. The results were analyzed using Fisher's test and analysis of variance (ANOVA), with a 5% level of significance (p=0.05).
Sixty-nine cases of trisomy were diagnosed among 840 exams; nine were excluded due to outcome outside Hospital de Clínicas de Porto Alegre or incomplete records, remaining 60 cases (nine cases of chromosome 13 trisomy, 26 of chromosome 18, and 25 of chromosome 21). In all three groups, heart disease occurred in most cases; the ventricular septal defect was more prevalent and occurred in 66.7% of the trisomy 13 group. Gastrointestinal abnormalities were more prevalent in the trisomy 18 group, especially omphalocele (38.5%; p<0.01). Genitourinary anomalies were more significantly frequent in the trisomy 13 group (pyelectasis, 55.6% - p<0.01; ambiguous genitalia, 33.3% - p=0.01). Central nervous system defects were identified in all cases of trisomy 13. Facial cracks were significantly more prevalent among fetuses with trisomy 13 (66.7%; p<0.01). Hand and feet malformations significantly differed among the trisomy groups. Hand defects occurred in 50% of trisomy 18 cases, and in 44.4% of all trisomy 13 cases (p<0.01); congenital clubfoot was more common in the trisomy 18 group, being detected in 46.2% of fetuses (p<0.01). The abnormalities were found in 50.9, 27.3 and 21.7% of trisomy 18, 13 and 21 cases respectively.
Many fetal malformations identified at ultrasound are suggestive of trisomy and represent an important tool for etiologic diagnosis and prenatal and pre-conception genetic counseling.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(7):333-338
DOI 10.1590/S0100-720320150005373
To describe the prevalence of malformations found in fetuses with trisomy of chromosomes 13, 18 and 21 by identifying the most frequent within each condition.
A retrospective cross-sectional study with the analysis of trisomy cases of chromosomes 13, 18 and 21 diagnosed through fetal karyotype obtained by amniocentesis/cordocentesis, between October 1994 and May 2014, at a Teaching Hospital in Brazil Southern Region. Malformations identified through morphological ultrasonography were described and, subsequently, confirmed in newborn examinations and/or fetal autopsy. The results were analyzed using Fisher's test and analysis of variance (ANOVA), with a 5% level of significance (p=0.05).
Sixty-nine cases of trisomy were diagnosed among 840 exams; nine were excluded due to outcome outside Hospital de Clínicas de Porto Alegre or incomplete records, remaining 60 cases (nine cases of chromosome 13 trisomy, 26 of chromosome 18, and 25 of chromosome 21). In all three groups, heart disease occurred in most cases; the ventricular septal defect was more prevalent and occurred in 66.7% of the trisomy 13 group. Gastrointestinal abnormalities were more prevalent in the trisomy 18 group, especially omphalocele (38.5%; p<0.01). Genitourinary anomalies were more significantly frequent in the trisomy 13 group (pyelectasis, 55.6% - p<0.01; ambiguous genitalia, 33.3% - p=0.01). Central nervous system defects were identified in all cases of trisomy 13. Facial cracks were significantly more prevalent among fetuses with trisomy 13 (66.7%; p<0.01). Hand and feet malformations significantly differed among the trisomy groups. Hand defects occurred in 50% of trisomy 18 cases, and in 44.4% of all trisomy 13 cases (p<0.01); congenital clubfoot was more common in the trisomy 18 group, being detected in 46.2% of fetuses (p<0.01). The abnormalities were found in 50.9, 27.3 and 21.7% of trisomy 18, 13 and 21 cases respectively.
Many fetal malformations identified at ultrasound are suggestive of trisomy and represent an important tool for etiologic diagnosis and prenatal and pre-conception genetic counseling.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(6):333-337
DOI 10.1590/S0100-72032000000600003
Purpose: to evaluate the efficacy of conservative axillary dissection (levels I and II) in the surgical treatment of stage I breast cancer. Methods: the results of 142 mastectomies performed from January/93 to December/98 in patients with clinical stage I breast cancer (T1NO) were evaluated. Removing the axillary lymph nodes present at levels I and II, with the preservation of the pectoralis muscles, the axillary lymph nodes were dissected by the author (LAGB), and subsequently one section of each lymph node was histopathologically evaluated. Quadrantectomy was performed in 138 cases and modified mastectomy (Patey), in 4 cases. The predominance of the T1c (130 cases) was observed. Results: a total of 3,282 lymph nodes were removed (2,456 at level I and 826 at level II), with an average of 23.1 nodes per axilla. Only 68 were histologically involved (2%). "Skip" metastasis was present only in one case (0.7%). Thirty-five false negative cases were observed (24.6%), with involvement of level I in 34 cases (97.1%) and of level II in 2 cases (5.7%). We observed 107 cases with negative axillary lymph nodes (75.4%). Conclusion: the axillary dissection of levels I and II is sufficient to treat the axilla in clinical stage I breast cancer. In clinical stage II and III of the disease, the complete axillary dissection including levels I, II and III is indicated. The interpectoral Rotter group will be removed if surgically suspicious.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2000;22(6):333-337
DOI 10.1590/S0100-72032000000600003
Purpose: to evaluate the efficacy of conservative axillary dissection (levels I and II) in the surgical treatment of stage I breast cancer. Methods: the results of 142 mastectomies performed from January/93 to December/98 in patients with clinical stage I breast cancer (T1NO) were evaluated. Removing the axillary lymph nodes present at levels I and II, with the preservation of the pectoralis muscles, the axillary lymph nodes were dissected by the author (LAGB), and subsequently one section of each lymph node was histopathologically evaluated. Quadrantectomy was performed in 138 cases and modified mastectomy (Patey), in 4 cases. The predominance of the T1c (130 cases) was observed. Results: a total of 3,282 lymph nodes were removed (2,456 at level I and 826 at level II), with an average of 23.1 nodes per axilla. Only 68 were histologically involved (2%). "Skip" metastasis was present only in one case (0.7%). Thirty-five false negative cases were observed (24.6%), with involvement of level I in 34 cases (97.1%) and of level II in 2 cases (5.7%). We observed 107 cases with negative axillary lymph nodes (75.4%). Conclusion: the axillary dissection of levels I and II is sufficient to treat the axilla in clinical stage I breast cancer. In clinical stage II and III of the disease, the complete axillary dissection including levels I, II and III is indicated. The interpectoral Rotter group will be removed if surgically suspicious.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-335
DOI 10.1590/S0100-72032001000500013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-335
DOI 10.1590/S0100-72032001000500013
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-334
DOI 10.1590/S0100-72032001000500012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2001;23(5):334-334
DOI 10.1590/S0100-72032001000500012
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(11):334-340
DOI 10.1590/S0100-72032011001100003
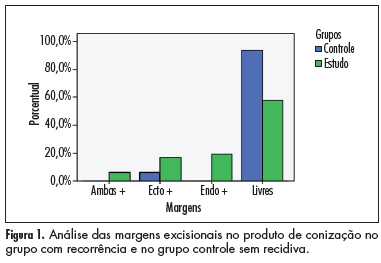
PURPOSE: To evaluate the ability of various factors related to the conization process in cytological/histological cervical intraepithelial neoplasias (CIN), after therapeutic conization. METHODS: A retrospective review was conducted of patients who had undergone conization due to CIN 2 and 3, from January 1999 to January 2006. They were divided into two groups: case group (residual disease or recurrence) and control group (without residual disease or recurrence), during 18 months of follow up. Univariate and multivariate analysis were used to define the predictive factors of disease recurrence. The c2 test or Fisher exact test was used for statistical analysis, with the level of significance set at p£0.05. RESULTS: Forty-eight patients showed recurrence/progression of CIN (case group) and 65 showed no recurrence/progression of disease (control group). Age and parity were similar in the two groups, as determined by calculation of the mean and standard deviation. There was no difference in smoking habits or in the use of contraceptive methods. The recurrence rate was 14.6%. Only conization positive margins were predictors of recurrence/progression (p<0.001). The conization techinique, the surgeon, CIN grade, gland involvement, and size of the uterine volume removed were not related to the evolution of disease after surgery. CONCLUSION: The recurrence of CIN 2 and 3 was related to positive margins in the product of conization.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2011;33(11):334-340
DOI 10.1590/S0100-72032011001100003
PURPOSE: To evaluate the ability of various factors related to the conization process in cytological/histological cervical intraepithelial neoplasias (CIN), after therapeutic conization. METHODS: A retrospective review was conducted of patients who had undergone conization due to CIN 2 and 3, from January 1999 to January 2006. They were divided into two groups: case group (residual disease or recurrence) and control group (without residual disease or recurrence), during 18 months of follow up. Univariate and multivariate analysis were used to define the predictive factors of disease recurrence. The c2 test or Fisher exact test was used for statistical analysis, with the level of significance set at p£0.05. RESULTS: Forty-eight patients showed recurrence/progression of CIN (case group) and 65 showed no recurrence/progression of disease (control group). Age and parity were similar in the two groups, as determined by calculation of the mean and standard deviation. There was no difference in smoking habits or in the use of contraceptive methods. The recurrence rate was 14.6%. Only conization positive margins were predictors of recurrence/progression (p<0.001). The conization techinique, the surgeon, CIN grade, gland involvement, and size of the uterine volume removed were not related to the evolution of disease after surgery. CONCLUSION: The recurrence of CIN 2 and 3 was related to positive margins in the product of conization.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(7):334-339
DOI 10.1590/S0100-72032010000700005
PURPOSE: to evaluate clinical and laboratory characteristics of first-degree male relatives of patients with a confirmed diagnosis of polycystic ovary syndrome (PCOS) and to compare the findings with a control group with no family history of PCOS. METHODS: we randomly selected 28 male individuals aged 18 to 65 years who were first-degree relatives of women diagnosed with PCOS and 28 controls matched for age, waist and body mass index (BMI). RESULTS: men with 1st degree kinship with women with PCOS had higher levels of triglycerides (189.6±103.1 versus 99.4±37.1, p<0.0001), Homeostasis Model Assessment (HOMA-IR) (3.5±9.1 versus 1.0±1.0, p=0.0077) and glucose (130.1±81.7 versus 89.5±7.8, p=0.005), and lower levels of sex hormone binding globulin (SHBG) (23.8±13.8 versus 31.1±9.1, p=0.003). SHBG levels correlated independently with triglyceride levels. These individuals also had more clinical signs of hyperandrogenism. CONCLUSIONS: male individuals who are first-degree relatives of patients with PCOS have a higher degree of dyslipidemia and insulin resistance, lower levels of SHBG, and more evident clinical signs of hyperandrogenism. These findings suggest that insulin resistance may be of hereditary origin in individuals with a family history of PCOS regardless of anthropometric parameters.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(7):334-339
DOI 10.1590/S0100-72032010000700005
PURPOSE: to evaluate clinical and laboratory characteristics of first-degree male relatives of patients with a confirmed diagnosis of polycystic ovary syndrome (PCOS) and to compare the findings with a control group with no family history of PCOS. METHODS: we randomly selected 28 male individuals aged 18 to 65 years who were first-degree relatives of women diagnosed with PCOS and 28 controls matched for age, waist and body mass index (BMI). RESULTS: men with 1st degree kinship with women with PCOS had higher levels of triglycerides (189.6±103.1 versus 99.4±37.1, p<0.0001), Homeostasis Model Assessment (HOMA-IR) (3.5±9.1 versus 1.0±1.0, p=0.0077) and glucose (130.1±81.7 versus 89.5±7.8, p=0.005), and lower levels of sex hormone binding globulin (SHBG) (23.8±13.8 versus 31.1±9.1, p=0.003). SHBG levels correlated independently with triglyceride levels. These individuals also had more clinical signs of hyperandrogenism. CONCLUSIONS: male individuals who are first-degree relatives of patients with PCOS have a higher degree of dyslipidemia and insulin resistance, lower levels of SHBG, and more evident clinical signs of hyperandrogenism. These findings suggest that insulin resistance may be of hereditary origin in individuals with a family history of PCOS regardless of anthropometric parameters.