You searched for:"Omero Benedicto Poli Neto"
We found (11) results for your search.Summary
Rev Bras Ginecol Obstet. 2022;44(12):1102-1109
To evaluate the use of misoprostol prior to hysteroscopy procedures regarding technical ease, the presence of side effects, and the occurrence of complications.
This is a retrospective, observational, analytical, case-control study, with the review of medical records of 266 patients followed-up at the Gynecological Videoendoscopy Sector of the Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto of the Universidade de São Paulo (HCFMRP – USP, in the Portuguese acronym) from 2014 to 2019, comparing 133 patients who used the drug before the procedure with 133 patients who did not.
The occurrence of postmenopausal uterine bleeding was the main indication for hysteroscopy and revealed a statistical difference between groups (p < 0.001), being present in 93.23% of the patients in the study group and in 69.7% of the patients in the control group. Only 2 patients (1.5%) in the study group reported adverse effects. Although no statistical differences were observed regarding the occurrence of complications during the procedure (p = 0.0662), a higher total number of complications was noted in the group that used misoprostol (n = 7; 5.26%) compared with the group that did not use the drug (n = 1; 0.75%), a fact that is clinically relevant. When evaluating the ease of the technique (measured by the complete performance of all steps of the hysteroscopy procedure), it was verified that although there was no difference between groups (p = 0.0586), the control group had more than twice as many incompletely performed procedures (n = 17) when compared with the group that used misoprostol previously (n = 8), which is also clinically relevant.
The use of misoprostol prior to hysteroscopy in our service indicated that the drug can facilitate the performance of the procedure, but not without side effects and presenting higher complication rates.
Summary
Rev Bras Ginecol Obstet. 2022;44(12):1102-1109
To evaluate the use of misoprostol prior to hysteroscopy procedures regarding technical ease, the presence of side effects, and the occurrence of complications.
This is a retrospective, observational, analytical, case-control study, with the review of medical records of 266 patients followed-up at the Gynecological Videoendoscopy Sector of the Hospital das Clínicas da Faculdade de Medicina de Ribeirão Preto of the Universidade de São Paulo (HCFMRP – USP, in the Portuguese acronym) from 2014 to 2019, comparing 133 patients who used the drug before the procedure with 133 patients who did not.
The occurrence of postmenopausal uterine bleeding was the main indication for hysteroscopy and revealed a statistical difference between groups (p < 0.001), being present in 93.23% of the patients in the study group and in 69.7% of the patients in the control group. Only 2 patients (1.5%) in the study group reported adverse effects. Although no statistical differences were observed regarding the occurrence of complications during the procedure (p = 0.0662), a higher total number of complications was noted in the group that used misoprostol (n = 7; 5.26%) compared with the group that did not use the drug (n = 1; 0.75%), a fact that is clinically relevant. When evaluating the ease of the technique (measured by the complete performance of all steps of the hysteroscopy procedure), it was verified that although there was no difference between groups (p = 0.0586), the control group had more than twice as many incompletely performed procedures (n = 17) when compared with the group that used misoprostol previously (n = 8), which is also clinically relevant.
The use of misoprostol prior to hysteroscopy in our service indicated that the drug can facilitate the performance of the procedure, but not without side effects and presenting higher complication rates.
Summary
Rev Bras Ginecol Obstet. 2008;30(4):167-170
DOI 10.1590/S0100-72032008000400002
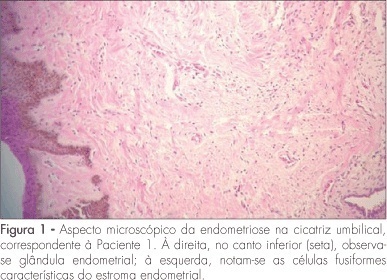
PURPOSE: to present a series of cases of umbilical endometriosis in patients in reproductive age, with no previous pelvic surgery. METHODS: four patients aged between 33 and 43 years were included in the study. They all presented umbilical bleeding associated or not with pelvic pain, and medical history varied from two months to four years. Abdominal wall ultrasound was performed for diagnosis support before surgical excision of the umbilical lesions, and histological examination was also performed. RESULTS: the ultrasonographic evaluation of the four patients showed hypoechogenic umbilical lesion suggestive of endometriosis. All patients were submitted to surgical excision and histological examination of the lesions. CA-125 serum levels were measured in three of the patients, but they were within normal ranges (from 6.8 to 10.1 U/mL). In addition to umbilical surgery, laparoscopy was performed in all patients, but only one presented concomitant pelvic endometriosis. In a one-year follow-up, patients maintained asymptomatic and there was no recurrence of the lesions. CONCLUSIONS: umbilical endometriosis is a rare entity, but it may be remembered as a possibility in cases of umbilical nodulations or bleeding, even if there is no previous history of pelvic surgery with endometrial manipulation. Its treatment is always surgical and, in general, it is enough to promote complete elimination of the lesion and of the symptoms.
Summary
Rev Bras Ginecol Obstet. 2008;30(4):167-170
DOI 10.1590/S0100-72032008000400002
PURPOSE: to present a series of cases of umbilical endometriosis in patients in reproductive age, with no previous pelvic surgery. METHODS: four patients aged between 33 and 43 years were included in the study. They all presented umbilical bleeding associated or not with pelvic pain, and medical history varied from two months to four years. Abdominal wall ultrasound was performed for diagnosis support before surgical excision of the umbilical lesions, and histological examination was also performed. RESULTS: the ultrasonographic evaluation of the four patients showed hypoechogenic umbilical lesion suggestive of endometriosis. All patients were submitted to surgical excision and histological examination of the lesions. CA-125 serum levels were measured in three of the patients, but they were within normal ranges (from 6.8 to 10.1 U/mL). In addition to umbilical surgery, laparoscopy was performed in all patients, but only one presented concomitant pelvic endometriosis. In a one-year follow-up, patients maintained asymptomatic and there was no recurrence of the lesions. CONCLUSIONS: umbilical endometriosis is a rare entity, but it may be remembered as a possibility in cases of umbilical nodulations or bleeding, even if there is no previous history of pelvic surgery with endometrial manipulation. Its treatment is always surgical and, in general, it is enough to promote complete elimination of the lesion and of the symptoms.
Summary
Rev Bras Ginecol Obstet. 2007;29(4):181-185
DOI 10.1590/S0100-72032007000400003
PURPOSE: to determine the efficacy of 10% lidocaine spray applied to the cervix before the procedure of diagnostic hysteroscopy, in order to reduce the painful process and the discomfort caused by the exam. METHODS: a total of 261 consecutive patients participated in the study, which was conducted from March 2004 to March 2005. The patients were randomly assigned to one of two groups: one group receiving topical lidocaine spray (lidocaine group - LdG) and the other, receiving no medication before the procedure (control group - CG). In the LdG patients, thirty milligrams of 10% lidocaine spray were applied to the surface of the cervix five minutes before hysteroscopy started. Immediately, after the end of the procedure, the patients from both groups were asked to respond to a questionnaire about pain and to quantify the pain, in centimeters, using a 10-cm non-graduated visual analog scale. The unpaired t test, the Mann-Whitney test and the chi2 test were used for statistical analyses, considering p significant if lower than 0.05. RESULTS: there was no statistically significant difference between groups regarding age, parity or percentage of patients in menacme or menopause, or regarding the indications for the procedure and the hysteroscopic findings. A biopsy was necessary in 57 of the 132 LdG patients and in 48 of the 129 CG patients (p=0.96). The mean pain score was 4.3±2.9 in LdG and 3.9±2.5 in CG (p=0.2). A difference in the mean pain score was observed only among patients in menacme and menopause receiving or not the lidocaine spray, with p=0.01 and p=0.04 respectively. CONCLUSIONS: the use of lidocaine spray during diagnostic hysteroscopy does not minimize the discomfort and pain of the patients and therefore should not be applied.
Summary
Rev Bras Ginecol Obstet. 2007;29(4):181-185
DOI 10.1590/S0100-72032007000400003
PURPOSE: to determine the efficacy of 10% lidocaine spray applied to the cervix before the procedure of diagnostic hysteroscopy, in order to reduce the painful process and the discomfort caused by the exam. METHODS: a total of 261 consecutive patients participated in the study, which was conducted from March 2004 to March 2005. The patients were randomly assigned to one of two groups: one group receiving topical lidocaine spray (lidocaine group - LdG) and the other, receiving no medication before the procedure (control group - CG). In the LdG patients, thirty milligrams of 10% lidocaine spray were applied to the surface of the cervix five minutes before hysteroscopy started. Immediately, after the end of the procedure, the patients from both groups were asked to respond to a questionnaire about pain and to quantify the pain, in centimeters, using a 10-cm non-graduated visual analog scale. The unpaired t test, the Mann-Whitney test and the chi2 test were used for statistical analyses, considering p significant if lower than 0.05. RESULTS: there was no statistically significant difference between groups regarding age, parity or percentage of patients in menacme or menopause, or regarding the indications for the procedure and the hysteroscopic findings. A biopsy was necessary in 57 of the 132 LdG patients and in 48 of the 129 CG patients (p=0.96). The mean pain score was 4.3±2.9 in LdG and 3.9±2.5 in CG (p=0.2). A difference in the mean pain score was observed only among patients in menacme and menopause receiving or not the lidocaine spray, with p=0.01 and p=0.04 respectively. CONCLUSIONS: the use of lidocaine spray during diagnostic hysteroscopy does not minimize the discomfort and pain of the patients and therefore should not be applied.

Summary
Rev Bras Ginecol Obstet. 2017;39(1):26-30
To evaluate the long-term effectiveness of perineal Thiele massage in the treatment of women with dyspareunia caused by tenderness of the pelvic floor muscles.
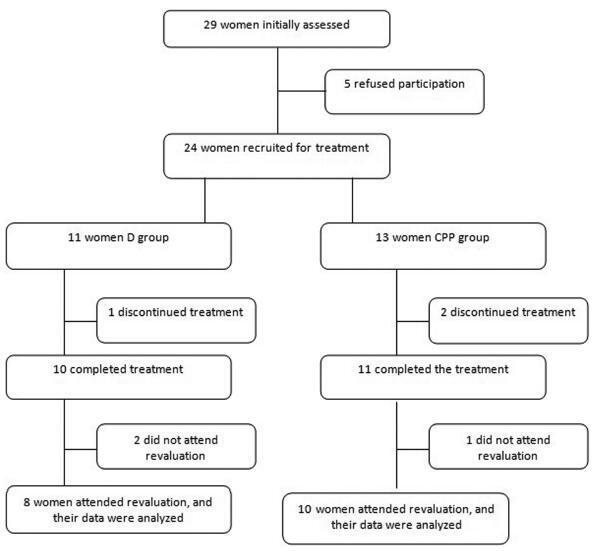
A total of 18 women with diagnoses of dyspareunia caused by tenderness of the pelvic floor muscles were included in the study. The women were divided in two groups: the dyspareunia (D) group - 8 women with dyspareunia caused by tenderness of the pelvic floor muscles; and the chronic pelvic pain group (CPP) group - 10 women with dyspareunia caused by tenderness of the pelvic floor muscles associated with CPP. Each patient filled out the Visual Analogue Scale (VAS), the McGill Pain Index, the Female Sexual Function Index (FSFI) and the Hospital Anxiety and Depression Scale (HADS). After an evaluation, the women underwent transvaginal massage using the Thiele technique over a period of 5 minutes, once a week for 4 weeks.
All women had significant improvements in their dyspareunia according the VAS and the McGill Pain Index (p < 0,001), but the HADS scores did not show significant differences. Regarding sexual function, the D group showed improvements on all aspects of sexual function, while the CPP group showed differences only in the pain domain.
Thiele massage is effective in the treatment of dyspareunia caused by tenderness of the pelvic floor muscles with a long-term pain relief.
Summary
Rev Bras Ginecol Obstet. 2017;39(1):26-30
To evaluate the long-term effectiveness of perineal Thiele massage in the treatment of women with dyspareunia caused by tenderness of the pelvic floor muscles.
A total of 18 women with diagnoses of dyspareunia caused by tenderness of the pelvic floor muscles were included in the study. The women were divided in two groups: the dyspareunia (D) group - 8 women with dyspareunia caused by tenderness of the pelvic floor muscles; and the chronic pelvic pain group (CPP) group - 10 women with dyspareunia caused by tenderness of the pelvic floor muscles associated with CPP. Each patient filled out the Visual Analogue Scale (VAS), the McGill Pain Index, the Female Sexual Function Index (FSFI) and the Hospital Anxiety and Depression Scale (HADS). After an evaluation, the women underwent transvaginal massage using the Thiele technique over a period of 5 minutes, once a week for 4 weeks.
All women had significant improvements in their dyspareunia according the VAS and the McGill Pain Index (p < 0,001), but the HADS scores did not show significant differences. Regarding sexual function, the D group showed improvements on all aspects of sexual function, while the CPP group showed differences only in the pain domain.
Thiele massage is effective in the treatment of dyspareunia caused by tenderness of the pelvic floor muscles with a long-term pain relief.
Summary
Rev Bras Ginecol Obstet. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
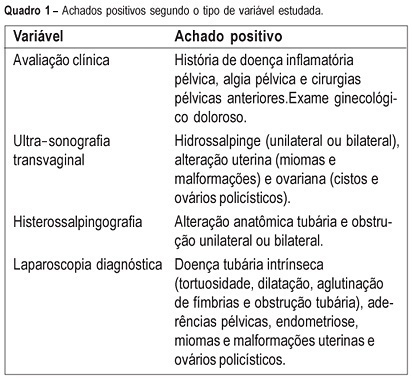
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Rev Bras Ginecol Obstet. 2005;27(7):401-406
DOI 10.1590/S0100-72032005000700006
PURPOSE: to evaluate the agreement between noninvasive methods - pelvic pain, transvaginal ultrasound and hysterosalpingography - and the gynecologic endoscopy approach for the diagnosis of tuboperitoneal factors responsible for conjugal infertility. METHODS: this is a cross-sectional study including 149 infertile patients who were submitted to clinical evaluation, transvaginal ultrasound, hysterosalpingography, hysteroscopy, and laparoscopy. In the evaluation of pelvic pain, the following complaints were considered to be abnormal: pelvic pain of the dyspareunia type, dysmenorrhea or acyclic pain, and pain upon mobilization of the cervix and palpation of the adnexa. Ultrasonographic examination was considered to be altered when adnexal or uterine morphological changes (hydrosalpinx, myomas or uterine malformations) were detected. Hysterosalpingography was considered to be abnormal in the presence of anatomical tubal changes and unilateral or bilateral obstruction. The agreement between noninvasive methods and endoscopy was evaluated by kappa statistics. RESULTS: the agreements between pelvic pain, transvaginal ultrasound, and hysterosalpingography and the endoscopic approach were 46.3% (kappa=0.092; CI 95%: -0.043 to 0.228), 24% (kappa=-0.052; CI 95%: -0.148 to 0.043), and 46% (kappa=0.092; CI 95%: -0.043 to 0.228), respectively. When at least one alteration detected by noninvasive methods was considered, the agreement with endoscopic approach was 63% (kappa=-0.014; CI 95%: -0.227 to 0.199). Sensitivity and specificity in predicting alterations on endoscopic approach were 39.5 and 80% in the presence of pelvic pain, 14.5 and 72% in the presence of alteration on transvaginal ultrasound, 39.5 and 80% in the presence of alteration on hysterosalpingography, and 70.2 and 28% in the presence of at least one alteration by noninvasive methods. CONCLUSION: there is a poor diagnostic agreement between the several noninvasive methods and endoscopy in the investigation of conjugal infertility secondary to tuboperitoneal factors.
Summary
Rev Bras Ginecol Obstet. 2009;31(9):425-426
Summary
Rev Bras Ginecol Obstet. 2009;31(9):425-426
Summary
Rev Bras Ginecol Obstet. 2016;38(1):47-52
Patient autonomy has great importance for a valid informed consent in clinical practice. Our objectives were to quantify thedomains of patient autonomy and to evaluate the variables that can affect patient autonomy in women with chronic pelvic pain.
This study is a cross sectional survey performed in a tertiary care University Hospital. Fifty-two consecutive women scheduled for laparoscopic management of chronic pelvic were included. Three major components of autonomy (competence, information or freedom) were evaluated using a Likert scale with 24 validated affirmatives.
Competence scores (0.85 vs 0.92; p = 0.006) and information scores (0.90 vs 0.93; p = 0.02) were low for women with less than eight years of school attendance. Information scores were low in the presence of anxiety (0.91 vs 0.93; p = 0.05) or depression (0.90 vs 0.93; p = 0.01).
Our data show that systematic evaluation of patient autonomy can provide clinical relevant information in gynecology. Low educational level, anxiety and depression might reduce the patient autonomy in women with chronic pelvic pain.
Summary
Rev Bras Ginecol Obstet. 2016;38(1):47-52
Patient autonomy has great importance for a valid informed consent in clinical practice. Our objectives were to quantify thedomains of patient autonomy and to evaluate the variables that can affect patient autonomy in women with chronic pelvic pain.
This study is a cross sectional survey performed in a tertiary care University Hospital. Fifty-two consecutive women scheduled for laparoscopic management of chronic pelvic were included. Three major components of autonomy (competence, information or freedom) were evaluated using a Likert scale with 24 validated affirmatives.
Competence scores (0.85 vs 0.92; p = 0.006) and information scores (0.90 vs 0.93; p = 0.02) were low for women with less than eight years of school attendance. Information scores were low in the presence of anxiety (0.91 vs 0.93; p = 0.05) or depression (0.90 vs 0.93; p = 0.01).
Our data show that systematic evaluation of patient autonomy can provide clinical relevant information in gynecology. Low educational level, anxiety and depression might reduce the patient autonomy in women with chronic pelvic pain.
Summary
Rev Bras Ginecol Obstet. 2006;28(12):733-740
DOI 10.1590/S0100-72032006001200008
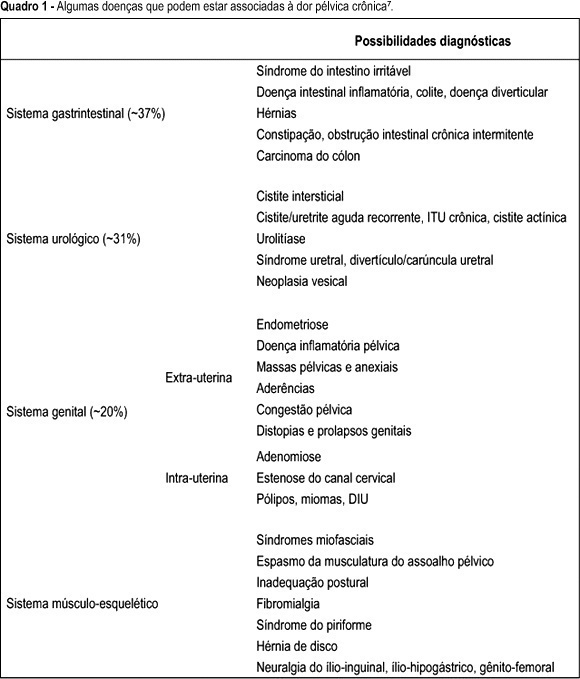
Chronic pelvic pain is a debilitating and highly prevalent disease with a major impact on quality of life and work productivity, beyond significant costs to health services. The dilemma of managing patients with chronic pelvic pain continues to frustrate physicians confronted with these complaints, in part because its pathophysiology is poorly understood. Consequently, its treatment is often unsatisfactory and limited to temporary symptom relief. In the present revision, we discuss the adequate management of chronic pelvic pain. We point out that a comprehensive medical history and physical examination should include special attention to gastrointestinal, urological, gynecological, muscle-skeletal, neurological, psychiatric, and endocrine systems. Thus, a multidisciplinary approach is recommended. Additionally, we emphasize that, although useful, specific surgical procedures, such as laparoscopy, should be indicated only to selected patients, mainly after excluding irritable bowel syndrome and pain of myofascial origin.
Summary
Rev Bras Ginecol Obstet. 2006;28(12):733-740
DOI 10.1590/S0100-72032006001200008
Chronic pelvic pain is a debilitating and highly prevalent disease with a major impact on quality of life and work productivity, beyond significant costs to health services. The dilemma of managing patients with chronic pelvic pain continues to frustrate physicians confronted with these complaints, in part because its pathophysiology is poorly understood. Consequently, its treatment is often unsatisfactory and limited to temporary symptom relief. In the present revision, we discuss the adequate management of chronic pelvic pain. We point out that a comprehensive medical history and physical examination should include special attention to gastrointestinal, urological, gynecological, muscle-skeletal, neurological, psychiatric, and endocrine systems. Thus, a multidisciplinary approach is recommended. Additionally, we emphasize that, although useful, specific surgical procedures, such as laparoscopy, should be indicated only to selected patients, mainly after excluding irritable bowel syndrome and pain of myofascial origin.