You searched for:"Leila Katz"
We found (9) results for your search.Summary
Rev Bras Ginecol Obstet. 2023;45(2):089-095
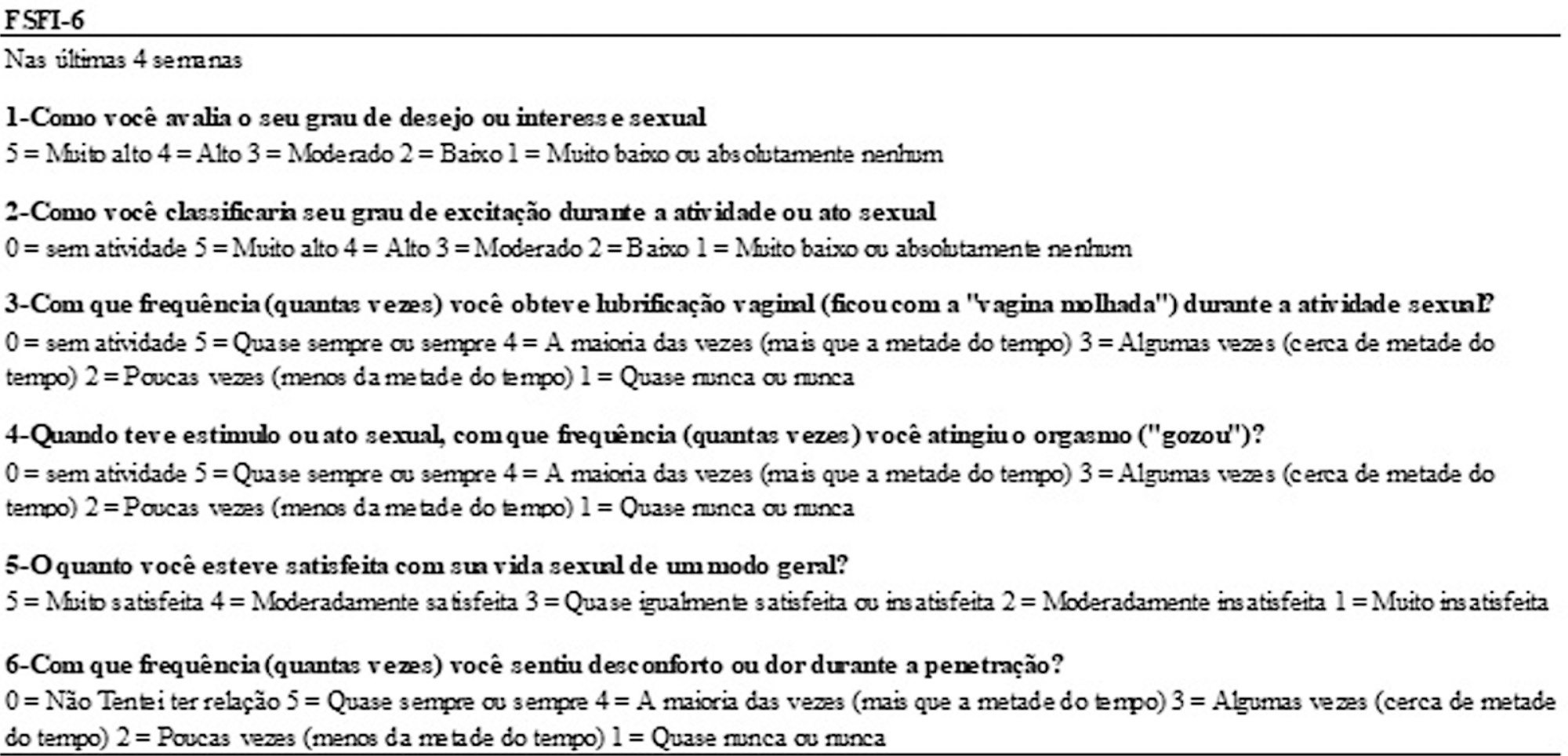
We evaluated internal consistency, test-retest reliability, and criterion validity of the Brazilian Portuguese version of the Female Sexual Function Index 6-item Version (FSFI-6) for postpartum women.
Therefore, questionnaires were applied to 100 sexually active women in the postpartum period. The Cronbach α coefficient was used to evaluate the internal consistency. Test-retest reliability was analyzed by Kappa for each item of the questionnaire and by the Wilcoxon parametric test, comparing the total scores of each evaluation. For the assessment of criterion validity, the FSFI was used as the gold standard and the receiver operating characteristic (ROC) curve was constructed. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). It was found that the internal consistency of the FSFI-6 questionnaire was considerably high (0.839).
The test-retest reliability results were satisfactory. It can also be stated that the FSFI-6 questionnaire presented excellent discriminant validity (area under the curve [AUC] = 0.926). Women may be considered as having sexual dysfunction if the overall FSFI-6 score is < 21, with 85.5% sensitivity, 82.2% specificity, positive likelihood ratio of 4.81 and negative likelihood ratio of 0.18.
We conclude that the Brazilian Portuguese version of FSFI-6 is valid for use in postpartum women.
Summary
Rev Bras Ginecol Obstet. 2023;45(2):089-095
We evaluated internal consistency, test-retest reliability, and criterion validity of the Brazilian Portuguese version of the Female Sexual Function Index 6-item Version (FSFI-6) for postpartum women.
Therefore, questionnaires were applied to 100 sexually active women in the postpartum period. The Cronbach α coefficient was used to evaluate the internal consistency. Test-retest reliability was analyzed by Kappa for each item of the questionnaire and by the Wilcoxon parametric test, comparing the total scores of each evaluation. For the assessment of criterion validity, the FSFI was used as the gold standard and the receiver operating characteristic (ROC) curve was constructed. Statistical analysis was performed using IBM SPSS Statistics for Windows, version 21.0 (IBM Corp., Armonk, NY, USA). It was found that the internal consistency of the FSFI-6 questionnaire was considerably high (0.839).
The test-retest reliability results were satisfactory. It can also be stated that the FSFI-6 questionnaire presented excellent discriminant validity (area under the curve [AUC] = 0.926). Women may be considered as having sexual dysfunction if the overall FSFI-6 score is < 21, with 85.5% sensitivity, 82.2% specificity, positive likelihood ratio of 4.81 and negative likelihood ratio of 0.18.
We conclude that the Brazilian Portuguese version of FSFI-6 is valid for use in postpartum women.
Summary
Rev Bras Ginecol Obstet. 2000;22(3):159-165
DOI 10.1590/S0100-72032000000300007
Purpose: to determine the frequency of recurrence of seizures after anticonvulsant therapy with magnesium sulfate and to evaluate treatment and maternal prognosis. Patients and Methods: a prospective cohort study was conducted, enrolling all cases of eclampsia managed at IMIP between January/1995 and June/1998. Magnesium sulfate and oxygen therapy were administered routinely and interruption of pregnancy was performed after maternal stabilization. The frequency of recurrence of seizures and its association with maternal complications were determined. chi² test for association was used at a 5% level of significance. Results: twelve cases presented recurrence of convulsions after magnesium sulfate (10%) and all received a repeated dose. In four of them convulsions persisted and they received intravenous diazepam. After diazepam, one patient still had seizures, with unsuccessful administration of phenytoin and therefore barbituric coma was induced (thionembutal). This patient had a CT-scan with evidence of intracerebral hemorrhage. Maternal complications were significantly more frequent in the group with recurrence: coma (16.7% versus 0.95), acidosis (50% versus 2.9%), pulmonary edema (16.7% versus 2.9%), cerebral hemorrhage (16.7% versus 0%) and acute renal failure (16.7% versus 1.9%). Three cases of maternal death occurred in patients with recurrence (25%) versus 2 cases in patients without recurrence (1.9%). Conclusions: rate of recurrence after anticonvulsant therapy with magnesium sulfate is low (10%) but it is associated with increased maternal morbidity and mortality. These cases must be managed in an intensive care unit and submitted to routine CT-scan because cerebral hemorrhage can be the cause of recurrence.
Summary
Rev Bras Ginecol Obstet. 2000;22(3):159-165
DOI 10.1590/S0100-72032000000300007
Purpose: to determine the frequency of recurrence of seizures after anticonvulsant therapy with magnesium sulfate and to evaluate treatment and maternal prognosis. Patients and Methods: a prospective cohort study was conducted, enrolling all cases of eclampsia managed at IMIP between January/1995 and June/1998. Magnesium sulfate and oxygen therapy were administered routinely and interruption of pregnancy was performed after maternal stabilization. The frequency of recurrence of seizures and its association with maternal complications were determined. chi² test for association was used at a 5% level of significance. Results: twelve cases presented recurrence of convulsions after magnesium sulfate (10%) and all received a repeated dose. In four of them convulsions persisted and they received intravenous diazepam. After diazepam, one patient still had seizures, with unsuccessful administration of phenytoin and therefore barbituric coma was induced (thionembutal). This patient had a CT-scan with evidence of intracerebral hemorrhage. Maternal complications were significantly more frequent in the group with recurrence: coma (16.7% versus 0.95), acidosis (50% versus 2.9%), pulmonary edema (16.7% versus 2.9%), cerebral hemorrhage (16.7% versus 0%) and acute renal failure (16.7% versus 1.9%). Three cases of maternal death occurred in patients with recurrence (25%) versus 2 cases in patients without recurrence (1.9%). Conclusions: rate of recurrence after anticonvulsant therapy with magnesium sulfate is low (10%) but it is associated with increased maternal morbidity and mortality. These cases must be managed in an intensive care unit and submitted to routine CT-scan because cerebral hemorrhage can be the cause of recurrence.
Summary
Rev Bras Ginecol Obstet. 1998;20(5):289-292
DOI 10.1590/S0100-72031998000500009
Pneumoperitoneum, abdominal pain and paralytic ileus in the postoperative period are usually related to perforation of the gastrointestinal tract. The authors present a case of a patient submitted to cesarean section (abruptio placentae) who had a postoperative course of abdominal distention and abdominal pain. Abdominal X-ray showed important dilatation of the colon and small bowel. Pneumoperitoneum was seen on chest X-ray. An exploratory laparotomy was performed because of suspicion of intestinal perforation. The operation showed a marked dilatation of bowel, pneumoperitoneum, and infected hemoperitoneum and subaponeurotic hematoma (Escherichia coli), without any perforation. Postoperative recovery was good and antibiotics were given for 4 days (ceftriaxone + metronidazole). The patient was diseharged from hospital on the 7th day after laparotomy. After review of the literature the authors concluded that this case of pneumoperitoneum was probably related to infection by a gas-producing bacterium in a patient with clinical findings of paralytic ileus.
Summary
Rev Bras Ginecol Obstet. 1998;20(5):289-292
DOI 10.1590/S0100-72031998000500009
Pneumoperitoneum, abdominal pain and paralytic ileus in the postoperative period are usually related to perforation of the gastrointestinal tract. The authors present a case of a patient submitted to cesarean section (abruptio placentae) who had a postoperative course of abdominal distention and abdominal pain. Abdominal X-ray showed important dilatation of the colon and small bowel. Pneumoperitoneum was seen on chest X-ray. An exploratory laparotomy was performed because of suspicion of intestinal perforation. The operation showed a marked dilatation of bowel, pneumoperitoneum, and infected hemoperitoneum and subaponeurotic hematoma (Escherichia coli), without any perforation. Postoperative recovery was good and antibiotics were given for 4 days (ceftriaxone + metronidazole). The patient was diseharged from hospital on the 7th day after laparotomy. After review of the literature the authors concluded that this case of pneumoperitoneum was probably related to infection by a gas-producing bacterium in a patient with clinical findings of paralytic ileus.
Summary
Rev Bras Ginecol Obstet. 2016;38(7):325-332
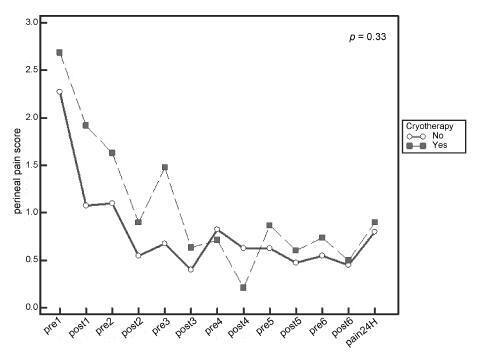
Systematic reviews that evaluate the perineal cryotherapy to reduce pain in the vaginal postpartum are inconclusive.
To evaluate clinical effectiveness of cryotherapy in the management of humanized postpartum perineal pain and vaginal edema.
A double-bind randomized controlled clinical trial (UTN number: U1111- 1131-8433) was conducted in a hospital in Northeastern, Brazil.Women were included following humanized childbirth. All had vaginal deliveries of a single, full-term pregnancy with cephalic presentation. Exclusion criteria included previous perineal lesion, episiotomy during the current delivery, instrumental delivery, uterine curettage and postpartum hemorrhage. In the experimental group, an ice pack was applied six times on the perineum for 20 minutes, reducing the temperature between 10 and 15° C, then 60 minutes without exposure to cold. In the non-cryotherapy, a water bag unable to reduce the temperature to this extent was used, compliance with the same application protocol of the first group. Perineal temperature wasmonitored at zero, 10 and 20 minutes for application in both groups. Evaluations were made immediately before and after the applications and 24 hours after delivery spontaneous, to determine the association between variables.
A total of 80 women were included in the study, 40 in each group. There was no significant difference in scores of perineal pain and edema between the groups with or without cryotherapy until 24 hours after childbirth. There was no difference between groups when accomplished repeated measures analysis over the 24 hours after delivery, considering the median perineal pain (p = 0.3) and edema (p = 0.9). Perineal cryotherapy did not influence the amount of analgesics used (p = 0.07) and no adverse effect was registered.
The use of cryotherapy following normal vaginal delivery within the concept of humanized minimally interventionist childbirth had no effect on perineal pain and edema, since it was already substantially lower, nor the need for pain medicaments.
Summary
Rev Bras Ginecol Obstet. 2016;38(7):325-332
Systematic reviews that evaluate the perineal cryotherapy to reduce pain in the vaginal postpartum are inconclusive.
To evaluate clinical effectiveness of cryotherapy in the management of humanized postpartum perineal pain and vaginal edema.
A double-bind randomized controlled clinical trial (UTN number: U1111- 1131-8433) was conducted in a hospital in Northeastern, Brazil.Women were included following humanized childbirth. All had vaginal deliveries of a single, full-term pregnancy with cephalic presentation. Exclusion criteria included previous perineal lesion, episiotomy during the current delivery, instrumental delivery, uterine curettage and postpartum hemorrhage. In the experimental group, an ice pack was applied six times on the perineum for 20 minutes, reducing the temperature between 10 and 15° C, then 60 minutes without exposure to cold. In the non-cryotherapy, a water bag unable to reduce the temperature to this extent was used, compliance with the same application protocol of the first group. Perineal temperature wasmonitored at zero, 10 and 20 minutes for application in both groups. Evaluations were made immediately before and after the applications and 24 hours after delivery spontaneous, to determine the association between variables.
A total of 80 women were included in the study, 40 in each group. There was no significant difference in scores of perineal pain and edema between the groups with or without cryotherapy until 24 hours after childbirth. There was no difference between groups when accomplished repeated measures analysis over the 24 hours after delivery, considering the median perineal pain (p = 0.3) and edema (p = 0.9). Perineal cryotherapy did not influence the amount of analgesics used (p = 0.07) and no adverse effect was registered.
The use of cryotherapy following normal vaginal delivery within the concept of humanized minimally interventionist childbirth had no effect on perineal pain and edema, since it was already substantially lower, nor the need for pain medicaments.
Summary
Rev Bras Ginecol Obstet. 2002;24(8):527-533
DOI 10.1590/S0100-72032002000800005
Purpose: to analyze the perinatal results of patients submitted to a 100 g oral glucose tolerance test (OGTT) during prenatal care at the Instituto Materno-Infantil de Pernambuco (IMIP), according to three different criteria. Methods: a cross-sectional study was conducted involving 210 pregnant patients attended at the IMIP, who were tested by a 100 g OGTT and had a singleton, topic pregnancy, without history of diabetes or glucose intolerance before pregnancy, and who delivered at the IMIP. The patients were classified into one of the following categories according to the levels found by OGTT: controls, mild hyperglycemia, Bertini's group, Carpenter's group and the National Diabetes Data Group (NDDG). These classes were then compared and association between the categories and preeclampsia, large for gestational age (LGA) newborns, rate of cesarean delivery, stillbirth, and mean birth weight was investigated. Results: the frequency of gestational diabetes was 48.1, 18.1, and 9% according to Bertini's, Carpenter and Coustan's and NDDG criteria, respectively, and mild hyperglycemia was present in 10.5%. Age of patients increased with a higher degree of carbohydrate intolerance. The groups did not differ regarding frequency of LGA, C-section, stillbirths, and birth weight. There was an increased frequency of preeclampsia among women with hyperglycemia and gestational diabetes according to Carpenter and Coustan's criteria. Conclusions: prevalence of gestational diabetes varied between 9 and 48% according to the different criteria, but maternal and perinatal results did not differ significantly among the groups. Strict diagnostic criteria can determine overdiagnosis without improvement of perinatal outcome.
Summary
Rev Bras Ginecol Obstet. 2002;24(8):527-533
DOI 10.1590/S0100-72032002000800005
Purpose: to analyze the perinatal results of patients submitted to a 100 g oral glucose tolerance test (OGTT) during prenatal care at the Instituto Materno-Infantil de Pernambuco (IMIP), according to three different criteria. Methods: a cross-sectional study was conducted involving 210 pregnant patients attended at the IMIP, who were tested by a 100 g OGTT and had a singleton, topic pregnancy, without history of diabetes or glucose intolerance before pregnancy, and who delivered at the IMIP. The patients were classified into one of the following categories according to the levels found by OGTT: controls, mild hyperglycemia, Bertini's group, Carpenter's group and the National Diabetes Data Group (NDDG). These classes were then compared and association between the categories and preeclampsia, large for gestational age (LGA) newborns, rate of cesarean delivery, stillbirth, and mean birth weight was investigated. Results: the frequency of gestational diabetes was 48.1, 18.1, and 9% according to Bertini's, Carpenter and Coustan's and NDDG criteria, respectively, and mild hyperglycemia was present in 10.5%. Age of patients increased with a higher degree of carbohydrate intolerance. The groups did not differ regarding frequency of LGA, C-section, stillbirths, and birth weight. There was an increased frequency of preeclampsia among women with hyperglycemia and gestational diabetes according to Carpenter and Coustan's criteria. Conclusions: prevalence of gestational diabetes varied between 9 and 48% according to the different criteria, but maternal and perinatal results did not differ significantly among the groups. Strict diagnostic criteria can determine overdiagnosis without improvement of perinatal outcome.
Summary
Rev Bras Ginecol Obstet. 2019;41(9):555-563
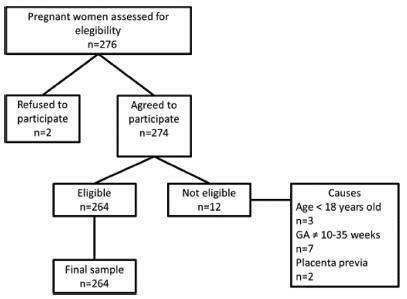
To determine the prevalence of sexual dysfunction and its associated factors in pregnant women.
A descriptive, cross-sectional study including 262 pregnant women aged 18 years or older with gestational age between 10 and 35 weeks. Women with urinary tract infections and conditions of gestational risk were excluded. The Pregnancy Sexual Response Inventory (PSRI) questionnaire was used. We performed a univariate descriptive analysis, and comparisons between the mean values of the sexual function domains were made using the Student t-test. The chi-squared test was used to determine the association between the independent and dependent variables. The prevalence ratios, with their respective 95% confidence intervals, were also estimated, and a multivariate analysis was performed.
A total of 64.9% of women reported a decrease in the frequency of sexual activity during pregnancy. Slightly more than half of the women (50.8%) were satisfied, and arousal was reported as excellent/good by 30.5% of them. The frequency of sexual difficulties/dysfunctions increased with pregnancy, rising from 5.7% to 58.8%, and pain during sexual intercourse was reported by 45.8% of them. Having higher education degree decreased the chance of being sexually dissatisfied by 50%. The total PSRI score showed a significant decrease from the prepregnancy period (mean score = 89.8, “excellent”) to the pregnancy period (mean score = 59.2, “good”).
The mean sexual function score during pregnancy was classified as good, although most pregnant women reported at least one type of alteration in the sexual function domains, and the report of dissatisfaction was more frequent in women with lower schooling.
Summary
Rev Bras Ginecol Obstet. 2019;41(9):555-563
To determine the prevalence of sexual dysfunction and its associated factors in pregnant women.
A descriptive, cross-sectional study including 262 pregnant women aged 18 years or older with gestational age between 10 and 35 weeks. Women with urinary tract infections and conditions of gestational risk were excluded. The Pregnancy Sexual Response Inventory (PSRI) questionnaire was used. We performed a univariate descriptive analysis, and comparisons between the mean values of the sexual function domains were made using the Student t-test. The chi-squared test was used to determine the association between the independent and dependent variables. The prevalence ratios, with their respective 95% confidence intervals, were also estimated, and a multivariate analysis was performed.
A total of 64.9% of women reported a decrease in the frequency of sexual activity during pregnancy. Slightly more than half of the women (50.8%) were satisfied, and arousal was reported as excellent/good by 30.5% of them. The frequency of sexual difficulties/dysfunctions increased with pregnancy, rising from 5.7% to 58.8%, and pain during sexual intercourse was reported by 45.8% of them. Having higher education degree decreased the chance of being sexually dissatisfied by 50%. The total PSRI score showed a significant decrease from the prepregnancy period (mean score = 89.8, “excellent”) to the pregnancy period (mean score = 59.2, “good”).
The mean sexual function score during pregnancy was classified as good, although most pregnant women reported at least one type of alteration in the sexual function domains, and the report of dissatisfaction was more frequent in women with lower schooling.
Summary
Rev Bras Ginecol Obstet. 2019;41(11):636-646
To determine the prevalence of episiotomy and the factors associated with the knowledge, attitude and practice (KAP) of Brazilian obstetricians in relation to this procedure.
A KAP survey was conducted with obstetricians working in Brazil. An electronic form containing structured questions previously evaluated using the Delphi method was created in Google Docs and sent by e-mail. A multivariate logistic regression was performed to determine the principal factors associated with adequate KAP. For each dependent variable (knowledge, attitude and practice) coded as adequate (1 = yes; 0 = no), a multiple logistic regression model was developed. Binary codes (1 = yes and 0 = no) were assigned to every independent or predictor variables. Prevalence ratios (PRs) and their respective 95% confidence intervals (95%CIs) were calculated as measures of relative risk, at a significance level of 5%.
Out of the 13 thousand physicians contacted, 1,163 replied, and 50 respondents were excluded. The mean episiotomy rate reported was of 42%. Knowledge was determined as adequate in 44.5% of the cases, attitude, in 10.9%, and practice, in 26.8% of the cases.
Most respondents had inadequate knowledge, attitudes and practices regarding episiotomy. Although some factors such as age, teaching, working in the public sector and attending congresses improved knowledge, attitude and practice, we must recognize that episiotomy rates remain well above what would be considered ideal. Adequate knowledge is more prevalent than adequate attitude or practice, indicating that improving knowledge is crucial but insufficient to change the outlook of episiotomies in Brazil.
Summary
Rev Bras Ginecol Obstet. 2019;41(11):636-646
To determine the prevalence of episiotomy and the factors associated with the knowledge, attitude and practice (KAP) of Brazilian obstetricians in relation to this procedure.
A KAP survey was conducted with obstetricians working in Brazil. An electronic form containing structured questions previously evaluated using the Delphi method was created in Google Docs and sent by e-mail. A multivariate logistic regression was performed to determine the principal factors associated with adequate KAP. For each dependent variable (knowledge, attitude and practice) coded as adequate (1 = yes; 0 = no), a multiple logistic regression model was developed. Binary codes (1 = yes and 0 = no) were assigned to every independent or predictor variables. Prevalence ratios (PRs) and their respective 95% confidence intervals (95%CIs) were calculated as measures of relative risk, at a significance level of 5%.
Out of the 13 thousand physicians contacted, 1,163 replied, and 50 respondents were excluded. The mean episiotomy rate reported was of 42%. Knowledge was determined as adequate in 44.5% of the cases, attitude, in 10.9%, and practice, in 26.8% of the cases.
Most respondents had inadequate knowledge, attitudes and practices regarding episiotomy. Although some factors such as age, teaching, working in the public sector and attending congresses improved knowledge, attitude and practice, we must recognize that episiotomy rates remain well above what would be considered ideal. Adequate knowledge is more prevalent than adequate attitude or practice, indicating that improving knowledge is crucial but insufficient to change the outlook of episiotomies in Brazil.
Summary
Rev Bras Ginecol Obstet. 2002;24(10):655-661
DOI 10.1590/S0100-72032002001000004
PURPOSE: to evaluate the effects of antenatal corticosteroid treatment on the incidence of respiratory distress syndrome (RDS), neonatal morbidities, and mortality in preterm babies assisted at IMIP, a teaching hospital in Brazil. METHODS: this was an observational, analytical, cohort study which included 155 newborns from women who delivered prematurely. The study was conducted between February and November 2001 and included 78 women in the corticosteroid-treated group and 77 in the nontreated group. The study design included the incidence of RDS, assessment of morbidities related to prematurity and tabulation of neonatal mortality. The risk ratio and its 95% confidence interval were determined for estimation of the relative risk for RDS and neonatal outcome (dependent variables) according to antenatal corticoid therapy administration (independent variable). RESULTS: corticosteroid treatment was administered to 50.3% of the patients (64% of the women received the full treatment course, while 36% of the same group received a partial course of treatment). The incidence of RDS was significantly lower in the corticosteroid treated group (37.2%) compared with the nontreated group (63.6%). There was no observable decrease in the risk for morbidities associated with prematurity. There was a decrease in mortality and in the frequency of supplemental oxygen therapy in the corticosteroid group (37%). On multiple logical regression analysis, there was a 72% reduction in the risk for RDS in the corticosteroid group, and approximately a seven times greater risk for RDS in babies of gestational age below 32 weeks. CONCLUSIONS: a favorable impact of antenatal corticosteroid administration was observed, with significant reduction of the risk for RDS in patients with gestational age between 26 and 35 weeks. Although no effect on the other morbidities was observed, this can be explained by the small size of the sample.
Summary
Rev Bras Ginecol Obstet. 2002;24(10):655-661
DOI 10.1590/S0100-72032002001000004
PURPOSE: to evaluate the effects of antenatal corticosteroid treatment on the incidence of respiratory distress syndrome (RDS), neonatal morbidities, and mortality in preterm babies assisted at IMIP, a teaching hospital in Brazil. METHODS: this was an observational, analytical, cohort study which included 155 newborns from women who delivered prematurely. The study was conducted between February and November 2001 and included 78 women in the corticosteroid-treated group and 77 in the nontreated group. The study design included the incidence of RDS, assessment of morbidities related to prematurity and tabulation of neonatal mortality. The risk ratio and its 95% confidence interval were determined for estimation of the relative risk for RDS and neonatal outcome (dependent variables) according to antenatal corticoid therapy administration (independent variable). RESULTS: corticosteroid treatment was administered to 50.3% of the patients (64% of the women received the full treatment course, while 36% of the same group received a partial course of treatment). The incidence of RDS was significantly lower in the corticosteroid treated group (37.2%) compared with the nontreated group (63.6%). There was no observable decrease in the risk for morbidities associated with prematurity. There was a decrease in mortality and in the frequency of supplemental oxygen therapy in the corticosteroid group (37%). On multiple logical regression analysis, there was a 72% reduction in the risk for RDS in the corticosteroid group, and approximately a seven times greater risk for RDS in babies of gestational age below 32 weeks. CONCLUSIONS: a favorable impact of antenatal corticosteroid administration was observed, with significant reduction of the risk for RDS in patients with gestational age between 26 and 35 weeks. Although no effect on the other morbidities was observed, this can be explained by the small size of the sample.