You searched for:"Eura Martins Lage"
We found (3) results for your search.Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):421-427
DOI 10.1590/SO100-720320150005355
To evaluate the prevalence of toxoplasmosis, rubella, cytomegalovirus, hepatitis B&C and syphilis (Torchs) in a cohort pregnant women and to identify the sociodemographic, clinical and laboratory factors.
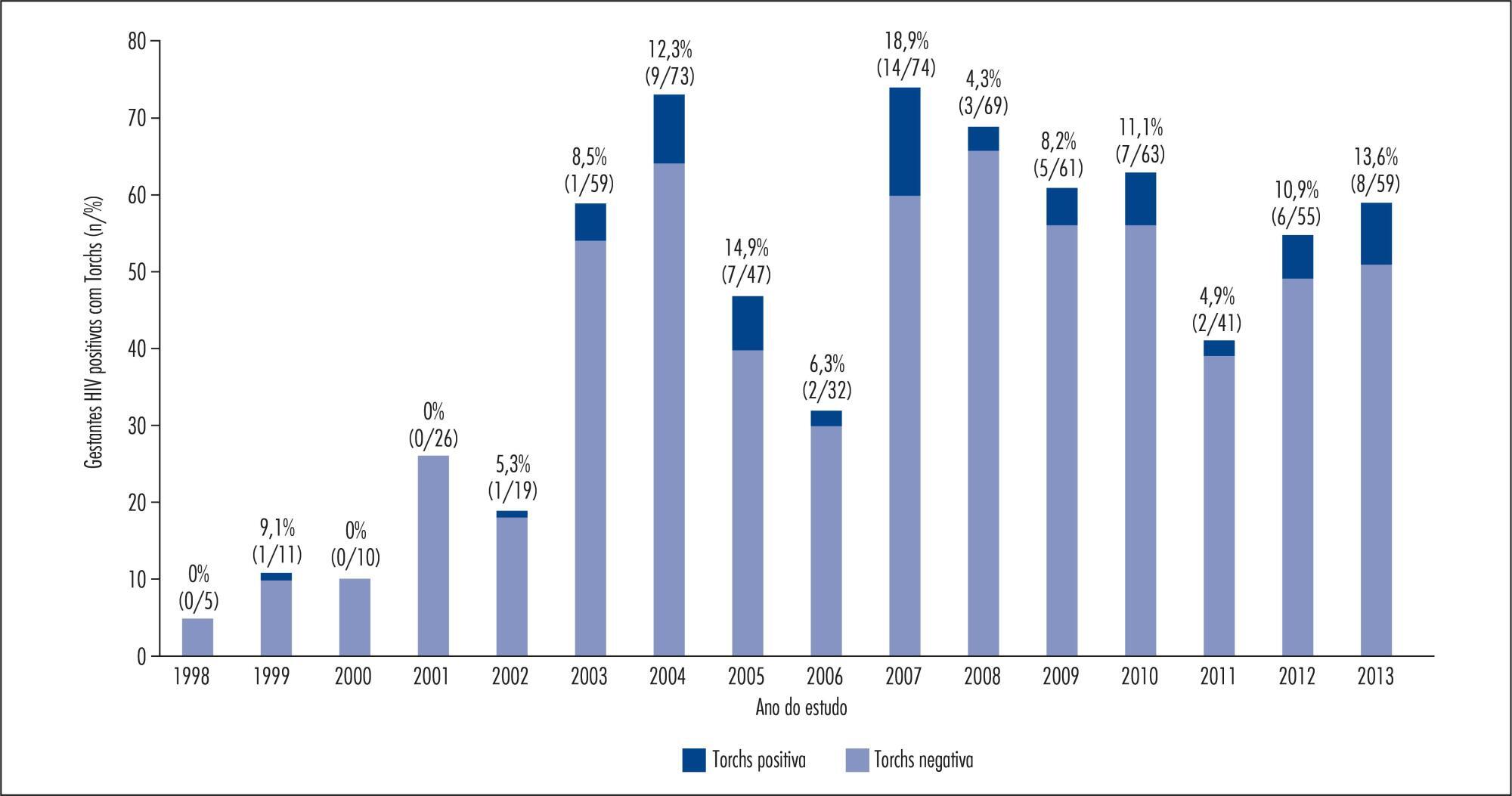
A total of 1,573 HIV-infected pregnant women from a Brazilian metropolitan region were studied between 1998 and 2013. The results of serological tests were available for 704 (44.8%) pregnant women. Pregnant women were considered to be Torchs positive (Gtp) when they had positive results for at least one of these infections, and to be Torchs negative (Gtn) when they had negative results for all of them. Maternal covariables were: age, marital status, educational level, time and mode of infection, CD4 lymphocyte count, viral load at delivery, and use of antiretroviral therapy (ARV). Neonatal covariables were: HIV infection, prematurity, low birth weight, neonatal complications, abortion and neonatal death. Odds ratios with 95% confidence interval were used to quantify the association between maternal and neonatal variables and the presence of Torchs.
Among 704 pregnant women, 70 (9.9%; 95%CI 7.8-12.4) had positive serological tests for any Torchs factor. The individual prevalence rates were: 1.5% (10/685) for toxoplasmosis; 1.3% (8/618) for rubella; 1.3% (8/597) for cytomegalovirus; 0.9% (6/653) for hepatitis B and 3.7% (20/545) for hepatitis C; and 3.8% (25/664) for syphilis. The HIV Vertical HIV transmission was 4.6% among Gtp pregnant women and 1.2% among Gtn women. Antiretroviral therapy (ARV), vertical transmission, low birth weight and neonatal complications were significantly associated with Torchs positivity in univariate analysis.
The Torchs prevalence found in the study was high for some infections. These findings emphasize the need to promote serological Torchs screening for all pregnant women, especially HIV-infected women, so that an early diagnosis can be made and treatment interventions can be implemented to prevent vertical HIV transmission.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2015;37(9):421-427
DOI 10.1590/SO100-720320150005355
To evaluate the prevalence of toxoplasmosis, rubella, cytomegalovirus, hepatitis B&C and syphilis (Torchs) in a cohort pregnant women and to identify the sociodemographic, clinical and laboratory factors.
A total of 1,573 HIV-infected pregnant women from a Brazilian metropolitan region were studied between 1998 and 2013. The results of serological tests were available for 704 (44.8%) pregnant women. Pregnant women were considered to be Torchs positive (Gtp) when they had positive results for at least one of these infections, and to be Torchs negative (Gtn) when they had negative results for all of them. Maternal covariables were: age, marital status, educational level, time and mode of infection, CD4 lymphocyte count, viral load at delivery, and use of antiretroviral therapy (ARV). Neonatal covariables were: HIV infection, prematurity, low birth weight, neonatal complications, abortion and neonatal death. Odds ratios with 95% confidence interval were used to quantify the association between maternal and neonatal variables and the presence of Torchs.
Among 704 pregnant women, 70 (9.9%; 95%CI 7.8-12.4) had positive serological tests for any Torchs factor. The individual prevalence rates were: 1.5% (10/685) for toxoplasmosis; 1.3% (8/618) for rubella; 1.3% (8/597) for cytomegalovirus; 0.9% (6/653) for hepatitis B and 3.7% (20/545) for hepatitis C; and 3.8% (25/664) for syphilis. The HIV Vertical HIV transmission was 4.6% among Gtp pregnant women and 1.2% among Gtn women. Antiretroviral therapy (ARV), vertical transmission, low birth weight and neonatal complications were significantly associated with Torchs positivity in univariate analysis.
The Torchs prevalence found in the study was high for some infections. These findings emphasize the need to promote serological Torchs screening for all pregnant women, especially HIV-infected women, so that an early diagnosis can be made and treatment interventions can be implemented to prevent vertical HIV transmission.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(12):584-590
DOI 10.1590/S0100-72032010001200004
PURPOSE: to evaluate the differences between the maternal and perinatal outcomes of pregnancies complicated by preeclampsia, according to the classification as the severe/mild form, and the early/late onset form. METHODS: a retrospective study with 211 pregnancies complicated by preeclampsia, assessed at a university reference center from 2000 to 2010. The diagnosis and disease severity were based on the values of blood pressure, proteinuria, and clinical and laboratory findings. The pregnant's age, skin color, parity, blood pressure, urine protein semiquantitative values, presence of bilateral notch in the uterine artery dopplervelocimetry and birth conditions were compared between patients with mild and severe disease, as well as between those of early/late onset. The disease was considered to be of early onset when diagnosed at less than 34 weeks of gestational age. RESULTS: most patients had the severe form of preeclampsia (82.8%), and the onset of the condition was early in 50.7%. Blood pressure values (133.6±14.8 versus 115.4 mmHg, p=0.0004 and 132.2±16.5 versus 125.7 mmHg, p=0.0004) and semiquantitative proteinuria (p=0.0003 and p=0.0005) were higher in the early and severe forms compared to mild and late forms. Infant birth weight (1,435.4±521.6 versus 2,710±605.0 g, 1,923.7±807.9 versus 2,415.0±925.0 g, p<0.0001 for both) and Apgar score (p=0.01 for both) were smaller for severe and early preeclampsia compared to mild and late preeclampsia. On the other hand, the presence of a bilateral notch in the uterine arteries was linked to the forms of early onset (69.2 versus 47.9%, p=0.02), whereas fetal growth restriction was more frequent in the severe forms of preeclampsia (30 versus 4.4%, p=0.008). CONCLUSION: the preeclampsia classification based on maternal clinical parameters better reflected the conditions of fetal nutrition, while the early onset of the condition was associated with placental vasculopathy detected by dopplervelocimetry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2010;32(12):584-590
DOI 10.1590/S0100-72032010001200004
PURPOSE: to evaluate the differences between the maternal and perinatal outcomes of pregnancies complicated by preeclampsia, according to the classification as the severe/mild form, and the early/late onset form. METHODS: a retrospective study with 211 pregnancies complicated by preeclampsia, assessed at a university reference center from 2000 to 2010. The diagnosis and disease severity were based on the values of blood pressure, proteinuria, and clinical and laboratory findings. The pregnant's age, skin color, parity, blood pressure, urine protein semiquantitative values, presence of bilateral notch in the uterine artery dopplervelocimetry and birth conditions were compared between patients with mild and severe disease, as well as between those of early/late onset. The disease was considered to be of early onset when diagnosed at less than 34 weeks of gestational age. RESULTS: most patients had the severe form of preeclampsia (82.8%), and the onset of the condition was early in 50.7%. Blood pressure values (133.6±14.8 versus 115.4 mmHg, p=0.0004 and 132.2±16.5 versus 125.7 mmHg, p=0.0004) and semiquantitative proteinuria (p=0.0003 and p=0.0005) were higher in the early and severe forms compared to mild and late forms. Infant birth weight (1,435.4±521.6 versus 2,710±605.0 g, 1,923.7±807.9 versus 2,415.0±925.0 g, p<0.0001 for both) and Apgar score (p=0.01 for both) were smaller for severe and early preeclampsia compared to mild and late preeclampsia. On the other hand, the presence of a bilateral notch in the uterine arteries was linked to the forms of early onset (69.2 versus 47.9%, p=0.02), whereas fetal growth restriction was more frequent in the severe forms of preeclampsia (30 versus 4.4%, p=0.008). CONCLUSION: the preeclampsia classification based on maternal clinical parameters better reflected the conditions of fetal nutrition, while the early onset of the condition was associated with placental vasculopathy detected by dopplervelocimetry.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):65-71
DOI 10.1590/S0100-72032014000200004
To analyze the relationships among gestational risk, type of delivery and
immediate maternal and neonatal repercussions.
A retrospective cohort study based on secondary data was conducted in a
university maternity hospital. A total of 1606 births were analyzed over a 9-month
period. Epidemiological, clinical, obstetric and neonatal characteristics were
compared according to the route of delivery and the gestational risk characterized
on the basis of the eligibility criteria for high clinical risk. The occurrence of
maternal and neonatal complications during hospitalization was analyzed according
to gestational risk and cesarean section delivery using univariate and
multivariate logistic analysis.
The overall rate of cesarean sections was 38.3%. High gestational risk was
present in 50.2% of births, mainly represented by hypertensive disorders and fetal
malformations. The total incidence of cesarean section, planned cesarean section
or emergency cesarean section was more frequent in pregnant women at gestational
high risk (p<0.001). Cesarean section alone did not influence maternal outcome,
but was associated with poor neonatal outcome (OR 3.4; 95%CI 2.7-4.4). Gestational
high risk was associated with poor maternal and neonatal outcome (OR 3.8; 95%CI
1.3-8.7 and OR 17.5; 95%CI 11.6-26.3, respectively). In multivariate analysis, the
ratios were maintained, although the effect of gestational risk has determined a
reduction in the OR of the type of delivery alone from 3.4 (95%CI 2.7-4.4) to 1.99
(95%CI 1.5-2.6) for adverse neonatal outcome.
Gestational risk was the main factor associated with poor maternal and neonatal
outcome. Cesarean delivery was not directly associated with poor maternal outcome
but increased the chances of unfavorable neonatal outcomes.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(2):65-71
DOI 10.1590/S0100-72032014000200004
To analyze the relationships among gestational risk, type of delivery and
immediate maternal and neonatal repercussions.
A retrospective cohort study based on secondary data was conducted in a
university maternity hospital. A total of 1606 births were analyzed over a 9-month
period. Epidemiological, clinical, obstetric and neonatal characteristics were
compared according to the route of delivery and the gestational risk characterized
on the basis of the eligibility criteria for high clinical risk. The occurrence of
maternal and neonatal complications during hospitalization was analyzed according
to gestational risk and cesarean section delivery using univariate and
multivariate logistic analysis.
The overall rate of cesarean sections was 38.3%. High gestational risk was
present in 50.2% of births, mainly represented by hypertensive disorders and fetal
malformations. The total incidence of cesarean section, planned cesarean section
or emergency cesarean section was more frequent in pregnant women at gestational
high risk (p<0.001). Cesarean section alone did not influence maternal outcome,
but was associated with poor neonatal outcome (OR 3.4; 95%CI 2.7-4.4). Gestational
high risk was associated with poor maternal and neonatal outcome (OR 3.8; 95%CI
1.3-8.7 and OR 17.5; 95%CI 11.6-26.3, respectively). In multivariate analysis, the
ratios were maintained, although the effect of gestational risk has determined a
reduction in the OR of the type of delivery alone from 3.4 (95%CI 2.7-4.4) to 1.99
(95%CI 1.5-2.6) for adverse neonatal outcome.
Gestational risk was the main factor associated with poor maternal and neonatal
outcome. Cesarean delivery was not directly associated with poor maternal outcome
but increased the chances of unfavorable neonatal outcomes.