You searched for:"Roxana Knobel"
We found (6) results for your search.-
Febrasgo Position Statement
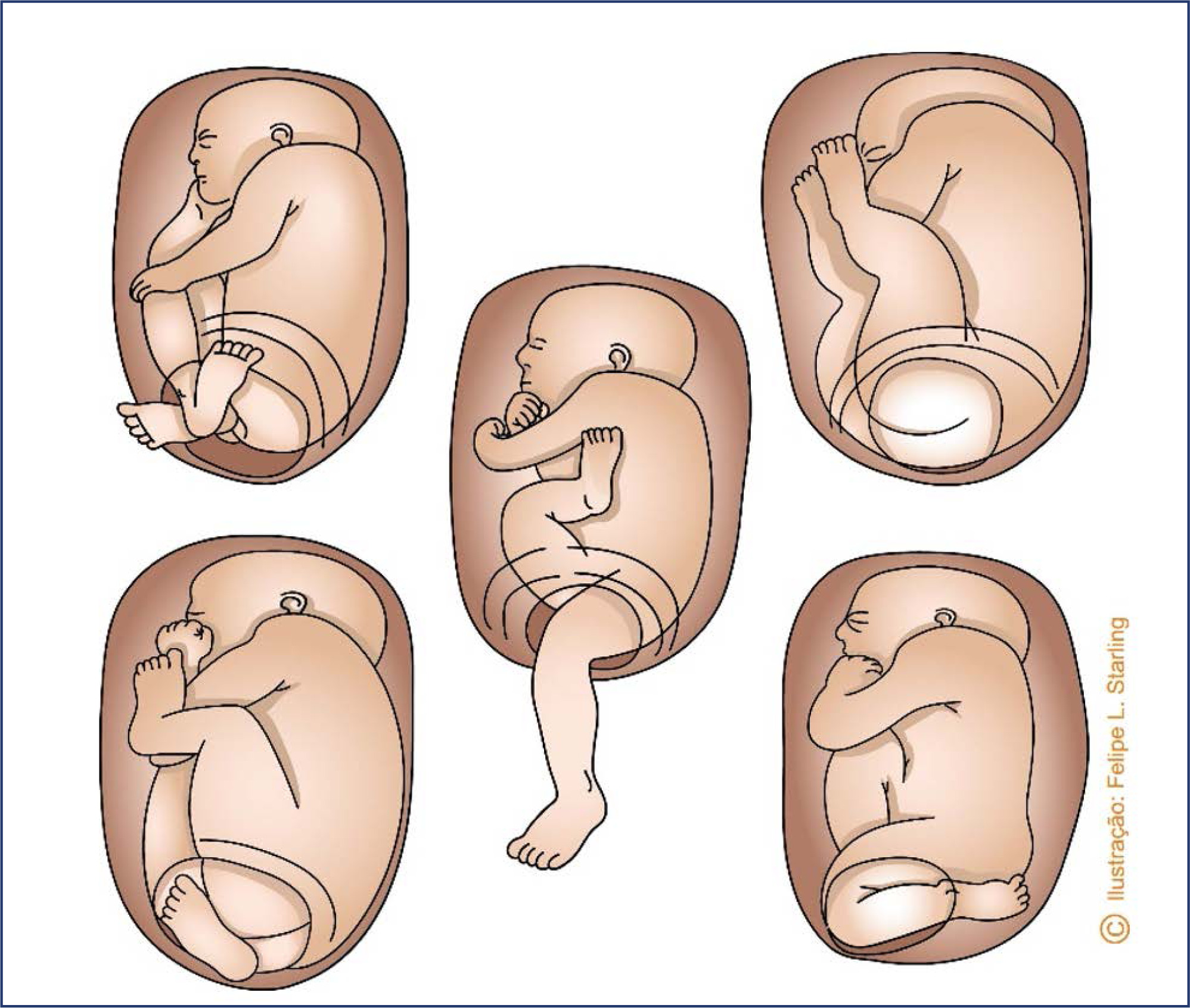
Breech birth care: Number 1 – 2024
- Álvaro Luiz Lage Alves
 ,
, - Alexandre Massao Nozaki ,
- Carla Betina Andreucci Polido ,
- Lucas Barbosa da Silva ,
- Roxana Knobel
Summary
Febrasgo Position StatementBreech birth care: Number 1 – 2024
Rev Bras Ginecol Obstet. 2024;46:e-rbgofps1
Views551

Summary
Febrasgo Position StatementBreech birth care: Number 1 – 2024
Rev Bras Ginecol Obstet. 2024;46:e-rbgofps1
- Álvaro Luiz Lage Alves
-
Letter to the Editor
Commentary on “Nonpharmacological Methods to Reduce Pain During Active Labor in a Real-life Setting”
Rev Bras Ginecol Obstet. 2023;45(9):549-550
Summary
Letter to the EditorCommentary on “Nonpharmacological Methods to Reduce Pain During Active Labor in a Real-life Setting”
Rev Bras Ginecol Obstet. 2023;45(9):549-550
Views2Dear Editor,We have read with interest the article by Silva et al. The study concluded that in a real-life setting there was no difference in the intensity of labor pain between patients who used nonpharmacological methods during the active phase of labor and those who did not. We appreciate the efforts of the research team, […]See moreViews2Summary
Letter to the EditorCommentary on “Nonpharmacological Methods to Reduce Pain During Active Labor in a Real-life Setting”
Rev Bras Ginecol Obstet. 2023;45(9):549-550
Views2Dear Editor,We have read with interest the article by Silva et al. The study concluded that in a real-life setting there was no difference in the intensity of labor pain between patients who used nonpharmacological methods during the active phase of labor and those who did not. We appreciate the efforts of the research team, […]See more -
Febrasgo Position Statement
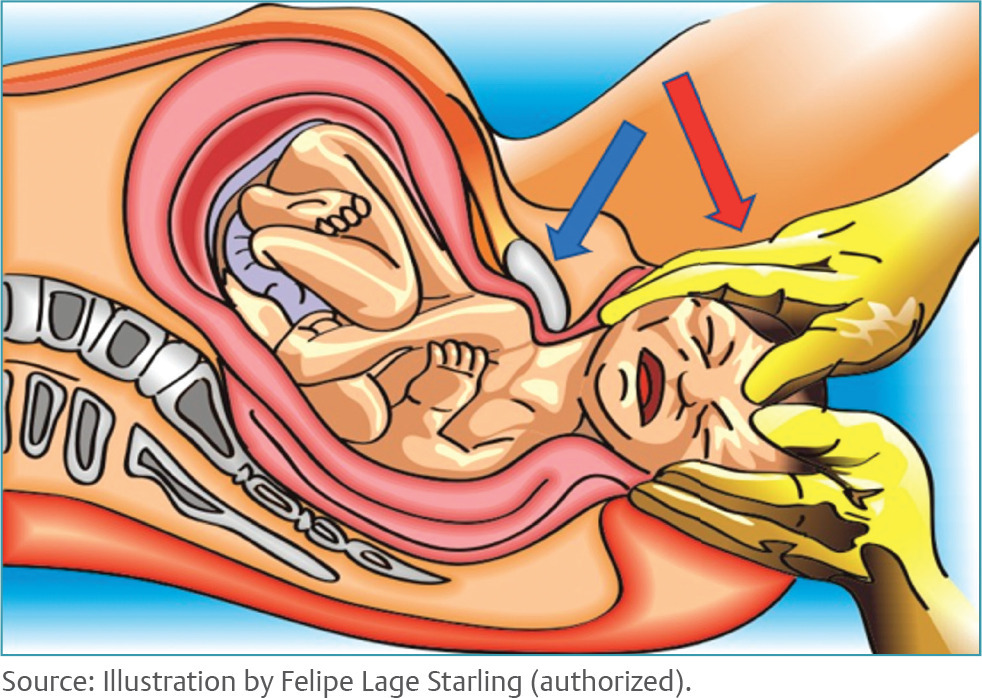
Management of shoulder dystocia – Number 7 – July 2022
Rev Bras Ginecol Obstet. 2022;44(7):723-736
Summary
Febrasgo Position StatementManagement of shoulder dystocia – Number 7 – July 2022
Rev Bras Ginecol Obstet. 2022;44(7):723-736
Views2Summary
Febrasgo Position StatementManagement of shoulder dystocia – Number 7 – July 2022
Rev Bras Ginecol Obstet. 2022;44(7):723-736
-
Original Article
Adequacy of Antenatal Care during the COVID-19 Pandemic: Observational Study with Postpartum Women
- Margot Marie Martin ,
- Roxana Knobel ,
- Vitor Nandi ,
- Jessica Goedert Pereira ,
- Alberto Trapani Junior , [ … ],
- Carla Betina Andreucci
Summary
Original ArticleAdequacy of Antenatal Care during the COVID-19 Pandemic: Observational Study with Postpartum Women
Rev Bras Ginecol Obstet. 2022;44(4):398-408
- Margot Marie Martin ,
- Roxana Knobel ,
- Vitor Nandi ,
- Jessica Goedert Pereira ,
- Alberto Trapani Junior ,
- Carla Betina Andreucci
Views4See moreAbstract
Objective
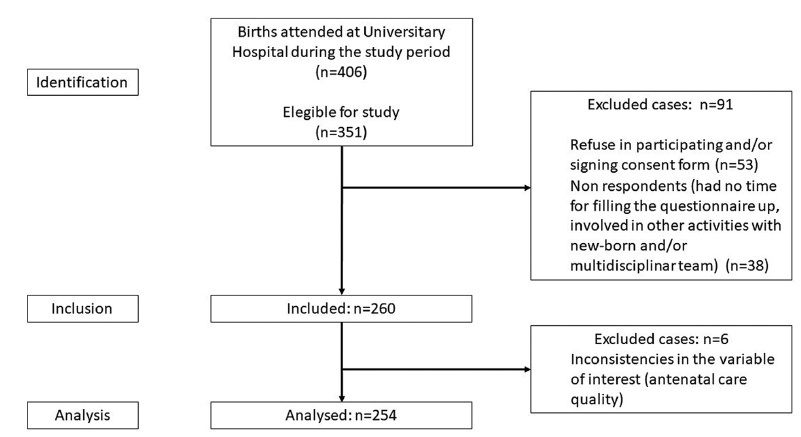
The present study aimed to evaluate the antenatal care adequacy for women who gave birth at the University Hospital of Santa Catarina in Florianopolis (Brazil) during the COVID-19 pandemic, and to evaluate the association of adequacy with sociodemographic, clinical, and access characteristics.
Methods
Data were collected between October and December 2020, including 254 patients who delivered in the University Hospital from Federal University of Santa Catarina and answered our questionnaires. Additional data were obtained from patients’ antenatal booklets. Antenatal care was classified as adequate, intermediate, or inadequate according to the number of appointments, gestational age at the beginning of follow-up, and tests results. We carried out a descriptive statistical analysis and a bivariate/with odds ratio analysis onmaternal sociodemographic, clinical and health access variables that were compared with antenatal adequacy.
Results
Antenatal care was considered adequate in 35.8% of cases, intermediate in 46.8%, and inadequate in 17.4%. The followingmaternal variables were associated with inadequate prenatal care (intermediate or inadequate prenatal care): having black or brown skin colour, having two or more children, being of foreign nationality, not being fluent in Portuguese, and using illicit drugs during pregnancy; the clinical variables were more than 6 weeks between appointments, and not attending high-risk antenatal care; as for access, the variables were difficulties in attending or scheduling appointments, and attending virtual appointments only.
Conclusion
In a sample of pregnant women from a teaching hospital in Florianópolis during the COVID-19 pandemic, antenatal care was considered adequate in 35.8%, intermediate in 46.8%, and inadequate in 17.4% of cases.
Views4Summary
Original ArticleAdequacy of Antenatal Care during the COVID-19 Pandemic: Observational Study with Postpartum Women
Rev Bras Ginecol Obstet. 2022;44(4):398-408
- Margot Marie Martin ,
- Roxana Knobel ,
- Vitor Nandi ,
- Jessica Goedert Pereira ,
- Alberto Trapani Junior ,
- Carla Betina Andreucci
Views4See moreAbstract
Objective
The present study aimed to evaluate the antenatal care adequacy for women who gave birth at the University Hospital of Santa Catarina in Florianopolis (Brazil) during the COVID-19 pandemic, and to evaluate the association of adequacy with sociodemographic, clinical, and access characteristics.
Methods
Data were collected between October and December 2020, including 254 patients who delivered in the University Hospital from Federal University of Santa Catarina and answered our questionnaires. Additional data were obtained from patients’ antenatal booklets. Antenatal care was classified as adequate, intermediate, or inadequate according to the number of appointments, gestational age at the beginning of follow-up, and tests results. We carried out a descriptive statistical analysis and a bivariate/with odds ratio analysis onmaternal sociodemographic, clinical and health access variables that were compared with antenatal adequacy.
Results
Antenatal care was considered adequate in 35.8% of cases, intermediate in 46.8%, and inadequate in 17.4%. The followingmaternal variables were associated with inadequate prenatal care (intermediate or inadequate prenatal care): having black or brown skin colour, having two or more children, being of foreign nationality, not being fluent in Portuguese, and using illicit drugs during pregnancy; the clinical variables were more than 6 weeks between appointments, and not attending high-risk antenatal care; as for access, the variables were difficulties in attending or scheduling appointments, and attending virtual appointments only.
Conclusion
In a sample of pregnant women from a teaching hospital in Florianópolis during the COVID-19 pandemic, antenatal care was considered adequate in 35.8%, intermediate in 46.8%, and inadequate in 17.4% of cases.
- Margot Marie Martin
-
Original Article
Cesarean-section Rates in Brazil from 2014 to 2016: Cross-sectional Analysis Using the Robson Classification
- Roxana Knobel ,
- Thiago Jose Pinheiro Lopes ,
- Mariane de Oliveira Menezes ,
- Carla Betina Andreucci ,
- Juliana Toledo Gieburowski , [ … ],
- Maira Libertad Soligo Takemoto
Summary
Original ArticleCesarean-section Rates in Brazil from 2014 to 2016: Cross-sectional Analysis Using the Robson Classification
Rev Bras Ginecol Obstet. 2020;42(9):522-528
- Roxana Knobel ,
- Thiago Jose Pinheiro Lopes ,
- Mariane de Oliveira Menezes ,
- Carla Betina Andreucci ,
- Juliana Toledo Gieburowski ,
- Maira Libertad Soligo Takemoto
Views3Abstract
Objective
To obtain cesarean-section (CS) rates according to the Robson Group Classification in five different regions of Brazil.
Methods
A descriptive epidemiological study using data from secondary birth records fromthe Computer Science Department of the Brazilian Unified Health System (Datasus, in Portuguese) between January 1st, 2014, and December 31st, 2016, including all live births in Brazil.
Results
The overall rate of CSwas of 56%. The sample was divided into 11 groups, and vaginal births were more frequent in groups 1 (53.6%), 3 (80.0%) and 4 (55.1%). The highest CS rates were found in groups 5 (85.7%), 6 (89.5%), 7 (85.2%) and 9 (97.0%). The overall CS rate per region varied from 46.2% in the North to 62.1% in the Midwest. Group 5 was the largest obstetric population in the South, Southeast and Midwest, and group 3 was the largest in the North and Northeast. Group 5 contributed the most to the overall CS rate, accounting for 30.8% of CSs.
Conclusion
Over half of the births in Brazil were cesarean sections. The Midwest had the highestCS rates,while theNorth had the lowest. The largestobstetric population in the North and in the Northeast was composed of women in group 3, while in the South, Southeast and Midwest it was group 5. Among all regions, the largest contribution to the overall CS rate was from group 5.
Key-words Cesarean sectioninduced laborobstetric deliveryrepeat cesarean sectionvaginal birth after cesarean sectionSee moreViews3Summary
Original ArticleCesarean-section Rates in Brazil from 2014 to 2016: Cross-sectional Analysis Using the Robson Classification
Rev Bras Ginecol Obstet. 2020;42(9):522-528
- Roxana Knobel ,
- Thiago Jose Pinheiro Lopes ,
- Mariane de Oliveira Menezes ,
- Carla Betina Andreucci ,
- Juliana Toledo Gieburowski ,
- Maira Libertad Soligo Takemoto
Views3Abstract
Objective
To obtain cesarean-section (CS) rates according to the Robson Group Classification in five different regions of Brazil.
Methods
A descriptive epidemiological study using data from secondary birth records fromthe Computer Science Department of the Brazilian Unified Health System (Datasus, in Portuguese) between January 1st, 2014, and December 31st, 2016, including all live births in Brazil.
Results
The overall rate of CSwas of 56%. The sample was divided into 11 groups, and vaginal births were more frequent in groups 1 (53.6%), 3 (80.0%) and 4 (55.1%). The highest CS rates were found in groups 5 (85.7%), 6 (89.5%), 7 (85.2%) and 9 (97.0%). The overall CS rate per region varied from 46.2% in the North to 62.1% in the Midwest. Group 5 was the largest obstetric population in the South, Southeast and Midwest, and group 3 was the largest in the North and Northeast. Group 5 contributed the most to the overall CS rate, accounting for 30.8% of CSs.
Conclusion
Over half of the births in Brazil were cesarean sections. The Midwest had the highestCS rates,while theNorth had the lowest. The largestobstetric population in the North and in the Northeast was composed of women in group 3, while in the South, Southeast and Midwest it was group 5. Among all regions, the largest contribution to the overall CS rate was from group 5.
Key-words Cesarean sectioninduced laborobstetric deliveryrepeat cesarean sectionvaginal birth after cesarean sectionSee more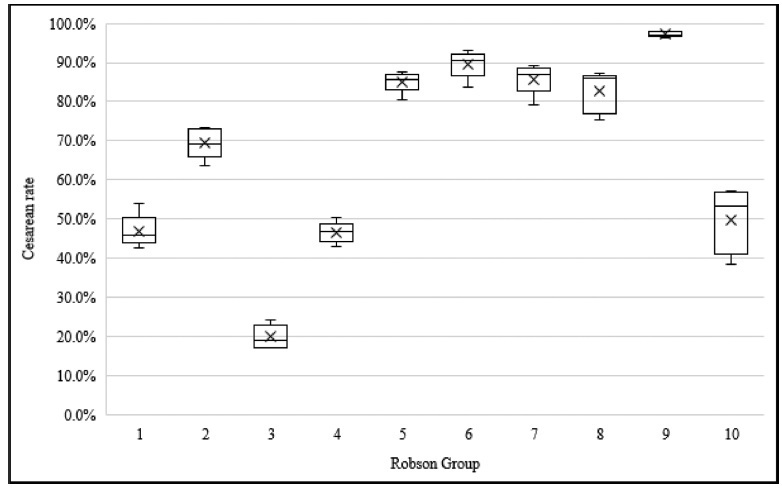
- Roxana Knobel
-
Original Article
A Simple, Reproducible and Low-cost Simulator for Teaching Surgical Techniques to Repair Obstetric Anal Sphincter Injuries
Rev Bras Ginecol Obstet. 2018;40(8):465-470
Summary
Original ArticleA Simple, Reproducible and Low-cost Simulator for Teaching Surgical Techniques to Repair Obstetric Anal Sphincter Injuries
Rev Bras Ginecol Obstet. 2018;40(8):465-470
Views0See moreAbstract
Objective
To describe and evaluate the use of a simple, low-cost, and reproducible simulator for teaching the repair of obstetric anal sphincter injuries (OASIS).
Methods
Twenty resident doctors in obstetrics and gynecology and four obstetricians participated in the simulation. A fourth-degree tear model was created using lowcost materials (condom simulating the rectal mucosa, cotton tissue simulating the internal anal sphincter, and bovine meat simulating the external anal sphincter). The simulator was initially assembled with the aid of anatomical photos to study the anatomy and meaning of each component of the model. The laceration was created and repaired, using end-to-end or overlapping application techniques.
Results
The model cost less than R$ 10.00 and was assembled without difficulty, which improved the knowledge of the participants of anatomy and physiology. The sutures of the layers (rectal mucosa, internal sphincter, and external sphincter) were performed in keeping with the surgical technique. All participants were satisfied with the simulation and felt it improved their knowledge and skills. Between 3 and 6 months after the training, 7 participants witnessed severe lacerations in their practice and reported that the simulation was useful for surgical correction.
Conclusion
The use of a simulator for repair training in OASIS is affordable (low-cost and easy to perform). The simulation seems to improve the knowledge and surgical skills necessary to repair severe lacerations. Further systematized studies should be performed for evaluation.
Views0Summary
Original ArticleA Simple, Reproducible and Low-cost Simulator for Teaching Surgical Techniques to Repair Obstetric Anal Sphincter Injuries
Rev Bras Ginecol Obstet. 2018;40(8):465-470
Views0See moreAbstract
Objective
To describe and evaluate the use of a simple, low-cost, and reproducible simulator for teaching the repair of obstetric anal sphincter injuries (OASIS).
Methods
Twenty resident doctors in obstetrics and gynecology and four obstetricians participated in the simulation. A fourth-degree tear model was created using lowcost materials (condom simulating the rectal mucosa, cotton tissue simulating the internal anal sphincter, and bovine meat simulating the external anal sphincter). The simulator was initially assembled with the aid of anatomical photos to study the anatomy and meaning of each component of the model. The laceration was created and repaired, using end-to-end or overlapping application techniques.
Results
The model cost less than R$ 10.00 and was assembled without difficulty, which improved the knowledge of the participants of anatomy and physiology. The sutures of the layers (rectal mucosa, internal sphincter, and external sphincter) were performed in keeping with the surgical technique. All participants were satisfied with the simulation and felt it improved their knowledge and skills. Between 3 and 6 months after the training, 7 participants witnessed severe lacerations in their practice and reported that the simulation was useful for surgical correction.
Conclusion
The use of a simulator for repair training in OASIS is affordable (low-cost and easy to perform). The simulation seems to improve the knowledge and surgical skills necessary to repair severe lacerations. Further systematized studies should be performed for evaluation.

Search
Search in:
Tag Cloud
breast (42) breast cancer (42) breast neoplasms (95) Cesarean section (72) endometriosis (66) infertility (56) Maternal mortality (43) menopause (82) obesity (58) postpartum period (40) pregnancy (225) Pregnancy complications (99) Prenatal care (68) prenatal diagnosis (50) Prevalence (41) Quality of life (51) risk factors (94) ultrasonography (79) urinary incontinence (40) women's health (48)