You searched for:"Geraldo Duarte"
We found (52) results for your search.-
Febrasgo Position Statement
Vulvovaginitis in pregnant women
- Geraldo Duarte
 ,
, - Iara Moreno Linhares ,
- Regis Kreitchmann ,
- Andréa da Rocha Tristão ,
- Evelyn Traina , [ … ],
- Joelma Queiroz Andrade
Summary
Febrasgo Position StatementVulvovaginitis in pregnant women
Rev Bras Ginecol Obstet. 2024;46:e-FPS03
- Geraldo Duarte ,
- Iara Moreno Linhares ,
- Regis Kreitchmann ,
- Andréa da Rocha Tristão ,
- Evelyn Traina ,
- Ivete Canti ,
- Marcos Takimura ,
- Joelma Queiroz Andrade
Views225See moreKey points
• The balanced vaginal microbiome is the main factor defending the vaginal environment against infections. Lactobacilli play a key role in this regard, maintaining the vaginal pH within the normal range (3.8 to 4.5).
•Hormonal and immune adaptations resulting from pregnancy influence changes in the vaginal microbiome during pregnancy.
•An altered vaginal microbiome predisposes to human immunodeficiency virus (HIV) infection.
•Bacterial vaginosis is the main clinical expression of an imbalanced vaginal microbiome.
•Vulvovaginal candidiasis depends more on the host’s conditions than on the etiological agent.
•Trichomonas vaginalis is a protozoan transmitted during sexual intercourse.
•The use of probiotics is not approved for use in pregnant women.
Views225

Summary
Febrasgo Position StatementVulvovaginitis in pregnant women
Rev Bras Ginecol Obstet. 2024;46:e-FPS03
- Geraldo Duarte ,
- Iara Moreno Linhares ,
- Regis Kreitchmann ,
- Andréa da Rocha Tristão ,
- Evelyn Traina ,
- Ivete Canti ,
- Marcos Takimura ,
- Joelma Queiroz Andrade
Views225See moreKey points
• The balanced vaginal microbiome is the main factor defending the vaginal environment against infections. Lactobacilli play a key role in this regard, maintaining the vaginal pH within the normal range (3.8 to 4.5).
•Hormonal and immune adaptations resulting from pregnancy influence changes in the vaginal microbiome during pregnancy.
•An altered vaginal microbiome predisposes to human immunodeficiency virus (HIV) infection.
•Bacterial vaginosis is the main clinical expression of an imbalanced vaginal microbiome.
•Vulvovaginal candidiasis depends more on the host’s conditions than on the etiological agent.
•Trichomonas vaginalis is a protozoan transmitted during sexual intercourse.
•The use of probiotics is not approved for use in pregnant women.
- Geraldo Duarte
-
Original Article
Seroprevalence of Toxoplasmosis in Puerperal Women Treated at a Tertiary Referral Hospital
- Juliana Fernandes Medeiros ,
- Ana Cláudia Rabelo e Silva ,
- Natália Domene Franco da Rocha ,
- Alexia Viegas Georg ,
- Patricia Pereira dos Santos Melli , [ … ],
- Geraldo Duarte
Summary
Original ArticleSeroprevalence of Toxoplasmosis in Puerperal Women Treated at a Tertiary Referral Hospital
Rev Bras Ginecol Obstet. 2023;45(2):059-064
- Juliana Fernandes Medeiros ,
- Ana Cláudia Rabelo e Silva ,
- Natália Domene Franco da Rocha ,
- Alexia Viegas Georg ,
- Patricia Pereira dos Santos Melli ,
- Silvana Maria Quintana ,
- Geraldo Duarte
Views0See moreAbstract
Objective
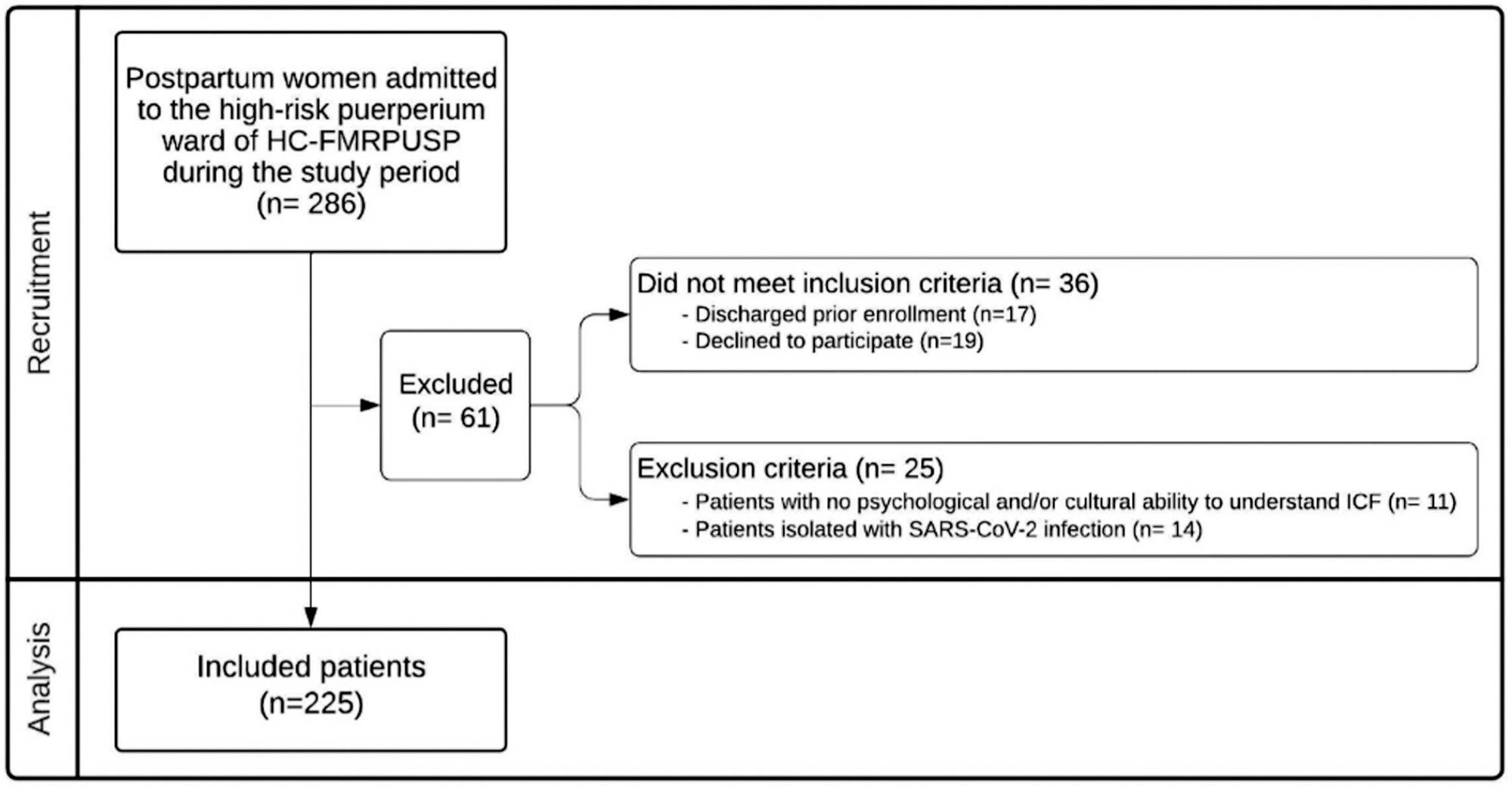
To evaluate the seroprevalence of toxoplasmosis among puerperal women cared for at a tertiary university hospital and the level of understanding of these puerperal women about toxoplasmosis, vertical transmission, and its prophylaxis.
Methods
For this cross-sectional study, we evaluated 225 patients using presential interviews, prenatal documentation, and electronic medical records. Data were stored using Research Electronic Data Capture (REDCap) software. Prevalence rates were estimated by the presence of reactive IgG antibodies against Toxoplasma gondii. Data analysis was performed using the chi-square test and calculation of the odds ratio (OR). Seroreactivity to T. gondii and exposure variables (age, educational level, and parity) were analyzed using a confidence interval (95%CI) and a significance level of 5% (p < 0.05).
Results
The seropositivity rate for T. gondii was 40%. There was no association between seroprevalence and age. Primiparity was a protective factor against seropositivity and low education was a risk factor.
Conclusion
Knowledge of T. gondii infection and its transmission forms was significantly limited, presenting a risk for acute maternal toxoplasmosis and vertical transmission of this protozoan. Increasing the education level regarding the risk of toxoplasmosis during pregnancy could reduce the rates of infection and vertical transmission of this parasite.
Views0Summary
Original ArticleSeroprevalence of Toxoplasmosis in Puerperal Women Treated at a Tertiary Referral Hospital
Rev Bras Ginecol Obstet. 2023;45(2):059-064
- Juliana Fernandes Medeiros ,
- Ana Cláudia Rabelo e Silva ,
- Natália Domene Franco da Rocha ,
- Alexia Viegas Georg ,
- Patricia Pereira dos Santos Melli ,
- Silvana Maria Quintana ,
- Geraldo Duarte
Views0See moreAbstract
Objective
To evaluate the seroprevalence of toxoplasmosis among puerperal women cared for at a tertiary university hospital and the level of understanding of these puerperal women about toxoplasmosis, vertical transmission, and its prophylaxis.
Methods
For this cross-sectional study, we evaluated 225 patients using presential interviews, prenatal documentation, and electronic medical records. Data were stored using Research Electronic Data Capture (REDCap) software. Prevalence rates were estimated by the presence of reactive IgG antibodies against Toxoplasma gondii. Data analysis was performed using the chi-square test and calculation of the odds ratio (OR). Seroreactivity to T. gondii and exposure variables (age, educational level, and parity) were analyzed using a confidence interval (95%CI) and a significance level of 5% (p < 0.05).
Results
The seropositivity rate for T. gondii was 40%. There was no association between seroprevalence and age. Primiparity was a protective factor against seropositivity and low education was a risk factor.
Conclusion
Knowledge of T. gondii infection and its transmission forms was significantly limited, presenting a risk for acute maternal toxoplasmosis and vertical transmission of this protozoan. Increasing the education level regarding the risk of toxoplasmosis during pregnancy could reduce the rates of infection and vertical transmission of this parasite.
- Juliana Fernandes Medeiros
-
Editorial
Increase in cesarean sections in Brazil – a call to reflection
- Antonio Braga ,
- Sue Yazaki Sun ,
- Alberto Carlos Moreno Zaconeta ,
- Alberto Trapani Junior ,
- Adriana Gomes Luz , [ … ],
- Rosiane Mattar
Summary
EditorialIncrease in cesarean sections in Brazil – a call to reflection
Rev Bras Ginecol Obstet. 2023;45(3):109-112
- Antonio Braga ,
- Sue Yazaki Sun ,
- Alberto Carlos Moreno Zaconeta ,
- Alberto Trapani Junior ,
- Adriana Gomes Luz ,
- Gabriel Osanan ,
- Geraldo Duarte ,
- José Geraldo Lopes Ramos ,
- Maria Celeste Osório Wender ,
- Roseli Mieko Yamamoto Nomura ,
- Rossana Pulcineli Vieira Francisco ,
- Vera Therezinha Medeiros Borges ,
- Rosiane Mattar
Views2Cesarean rates have increased progressively over the decades in all countries, and a high figure of 56% was reached in Brazil, second only to the Dominican Republic (59%) and well above the average of developing countries. This scenario in our country motivated government and private sector initiatives, among which the Projeto Parto Adequado (“Adequate Childbirth […]See moreViews2Summary
EditorialIncrease in cesarean sections in Brazil – a call to reflection
Rev Bras Ginecol Obstet. 2023;45(3):109-112
- Antonio Braga ,
- Sue Yazaki Sun ,
- Alberto Carlos Moreno Zaconeta ,
- Alberto Trapani Junior ,
- Adriana Gomes Luz ,
- Gabriel Osanan ,
- Geraldo Duarte ,
- José Geraldo Lopes Ramos ,
- Maria Celeste Osório Wender ,
- Roseli Mieko Yamamoto Nomura ,
- Rossana Pulcineli Vieira Francisco ,
- Vera Therezinha Medeiros Borges ,
- Rosiane Mattar
Views2Cesarean rates have increased progressively over the decades in all countries, and a high figure of 56% was reached in Brazil, second only to the Dominican Republic (59%) and well above the average of developing countries. This scenario in our country motivated government and private sector initiatives, among which the Projeto Parto Adequado (“Adequate Childbirth […]See more - Antonio Braga
-
Original Article
Expert Recommendations on Monkeypox (MPX) in Pregnancy, Postpartum and Lactating Women
- Rosiane Mattar ,
- Antonio Rodrigues Braga Neto ,
- Adriana Gomes Luz ,
- Alan Hatanaka ,
- Alberto Zaconeta , [ … ],
- Vera Therezinha Medeiros Borges
Summary
Original ArticleExpert Recommendations on Monkeypox (MPX) in Pregnancy, Postpartum and Lactating Women
Rev Bras Ginecol Obstet. 2022;44(12):1122-1125
- Rosiane Mattar ,
- Antonio Rodrigues Braga Neto ,
- Adriana Gomes Luz ,
- Alan Hatanaka ,
- Alberto Zaconeta ,
- Cristina Aparecida Falbo Guazzelli ,
- Evelyn Traina ,
- Fernanda Spadotto Baptista ,
- Gabriel Osanan ,
- Geraldo Duarte ,
- Jose Geraldo Lopes Ramos ,
- Maria Lucia Oppermann ,
- Rossana Pulcineli Vieira Francisco ,
- Sigrid Maria Loureiro de Queiroz Cardoso ,
- Silvana Maria Quintana ,
- Sue Yazaki Sun ,
- Vera Therezinha Medeiros Borges
Views0The Monkeypox DiseaseIn 2020, Brazil and the whole world faced the COVID-19 pandemic, which caused a high number of deaths. This disease was particularly severe for pregnant and postpartum women and determined a significant increase in the Maternal Death Ratio (MMR). To face the disease and assist health professionals in the qualification of the best […]See moreViews0Summary
Original ArticleExpert Recommendations on Monkeypox (MPX) in Pregnancy, Postpartum and Lactating Women
Rev Bras Ginecol Obstet. 2022;44(12):1122-1125
- Rosiane Mattar ,
- Antonio Rodrigues Braga Neto ,
- Adriana Gomes Luz ,
- Alan Hatanaka ,
- Alberto Zaconeta ,
- Cristina Aparecida Falbo Guazzelli ,
- Evelyn Traina ,
- Fernanda Spadotto Baptista ,
- Gabriel Osanan ,
- Geraldo Duarte ,
- Jose Geraldo Lopes Ramos ,
- Maria Lucia Oppermann ,
- Rossana Pulcineli Vieira Francisco ,
- Sigrid Maria Loureiro de Queiroz Cardoso ,
- Silvana Maria Quintana ,
- Sue Yazaki Sun ,
- Vera Therezinha Medeiros Borges
Views0The Monkeypox DiseaseIn 2020, Brazil and the whole world faced the COVID-19 pandemic, which caused a high number of deaths. This disease was particularly severe for pregnant and postpartum women and determined a significant increase in the Maternal Death Ratio (MMR). To face the disease and assist health professionals in the qualification of the best […]See more - Rosiane Mattar
-
Original Article
Assistance to Victims of Sexual Violence in a Referral Service: A 10-Year Experience
- Gabriel Ramalho de Jesus ,
- Natália Pavoni Rodrigues ,
- Giordana Campos Braga ,
- Renata Abduch ,
- Patricia Pereira dos Santos Melli , [ … ],
- Silvana Maria Quintana
Summary
Original ArticleAssistance to Victims of Sexual Violence in a Referral Service: A 10-Year Experience
Rev Bras Ginecol Obstet. 2022;44(1):47-54
- Gabriel Ramalho de Jesus ,
- Natália Pavoni Rodrigues ,
- Giordana Campos Braga ,
- Renata Abduch ,
- Patricia Pereira dos Santos Melli ,
- Geraldo Duarte ,
- Silvana Maria Quintana
Views1See moreAbstract
Objective
To evaluate the assistance provided to women victims of sexual violence and their participation in the follow-up treatment after the traumatic event, presenting a sociodemographic profile, gynecological background, and circumstances of the event, and reporting the results, acceptance, and side effects of prophylaxis for sexually transmitted infections (STIs) and pregnancy.
Methods
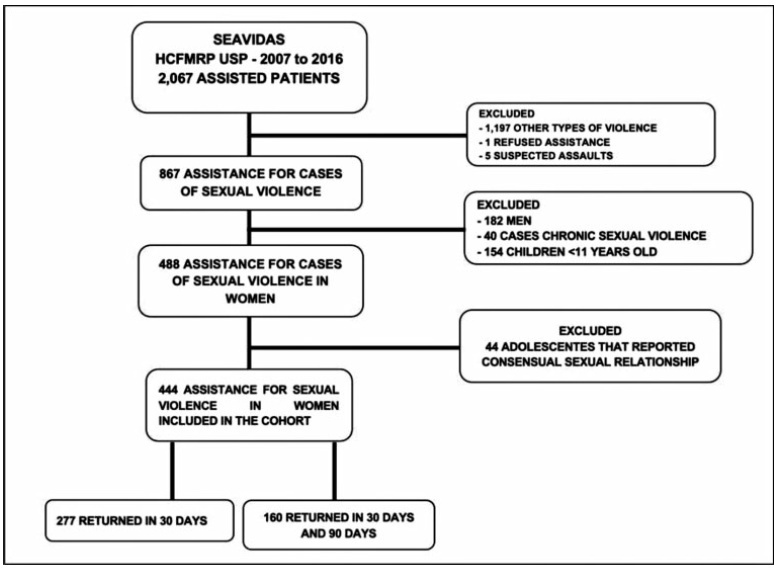
A retrospective cohort study comprising the period between 2007 and 2016. All women receiving medical care and clinical follow-up after a severe episode of sexual violence were included. Records of domestic violence, male victims, children, and adolescents who reported consensual sexual activity were excluded. The present study included descriptive statistics as frequencies and percentages.
Results
A total of 867medical records were reviewed and 444 cases of sexual violence were included. The age of the victims ranged from10 to 77 years old, most of them selfdeclared white, with between 4 and 8 years of education, and denying having a sexual partner. Sexual violence occurred predominantly at night, on public thoroughfare, being committed by an unknown offender. Most victims were assisted at the referral service center within 72 hours after the violence, enabling the recommended prophylaxis. There was high acceptance of antiretroviral therapy (ART), although half of the users reported side effects. Seroconversion to human immunodeficiency virus (HIV) or to hepatitis B virus (HBV) was not detected in women undergoing prophylaxis.
Conclusion
In the present cohort, the profile of victims of sexual violence was loweducated, young, white women. The traumatic event occurred predominantly at night, on public thoroughfare, being committed by an unknown offender. Assistance within the first 72 hours after sexual violence enables the healthcare center to provide prophylactic interventions against STIs and unwanted pregnancies.
Views1Summary
Original ArticleAssistance to Victims of Sexual Violence in a Referral Service: A 10-Year Experience
Rev Bras Ginecol Obstet. 2022;44(1):47-54
- Gabriel Ramalho de Jesus ,
- Natália Pavoni Rodrigues ,
- Giordana Campos Braga ,
- Renata Abduch ,
- Patricia Pereira dos Santos Melli ,
- Geraldo Duarte ,
- Silvana Maria Quintana
Views1See moreAbstract
Objective
To evaluate the assistance provided to women victims of sexual violence and their participation in the follow-up treatment after the traumatic event, presenting a sociodemographic profile, gynecological background, and circumstances of the event, and reporting the results, acceptance, and side effects of prophylaxis for sexually transmitted infections (STIs) and pregnancy.
Methods
A retrospective cohort study comprising the period between 2007 and 2016. All women receiving medical care and clinical follow-up after a severe episode of sexual violence were included. Records of domestic violence, male victims, children, and adolescents who reported consensual sexual activity were excluded. The present study included descriptive statistics as frequencies and percentages.
Results
A total of 867medical records were reviewed and 444 cases of sexual violence were included. The age of the victims ranged from10 to 77 years old, most of them selfdeclared white, with between 4 and 8 years of education, and denying having a sexual partner. Sexual violence occurred predominantly at night, on public thoroughfare, being committed by an unknown offender. Most victims were assisted at the referral service center within 72 hours after the violence, enabling the recommended prophylaxis. There was high acceptance of antiretroviral therapy (ART), although half of the users reported side effects. Seroconversion to human immunodeficiency virus (HIV) or to hepatitis B virus (HBV) was not detected in women undergoing prophylaxis.
Conclusion
In the present cohort, the profile of victims of sexual violence was loweducated, young, white women. The traumatic event occurred predominantly at night, on public thoroughfare, being committed by an unknown offender. Assistance within the first 72 hours after sexual violence enables the healthcare center to provide prophylactic interventions against STIs and unwanted pregnancies.
- Gabriel Ramalho de Jesus
-
Editorial
Gynecologists and Obstetricians Working Group to Face the COVID-19 Pandemic in Brazil: Successful Experience to be Followed
Rev Bras Ginecol Obstet. 2021;43(8):585-587
Summary
EditorialGynecologists and Obstetricians Working Group to Face the COVID-19 Pandemic in Brazil: Successful Experience to be Followed
Rev Bras Ginecol Obstet. 2021;43(8):585-587
Views1In addition to causing relevant changes in the global routine, the COVID-19 pandemic status announced and recognized by the World Health Organization (WHO) on March 11, 2020, made it clear that no country was ready to face an infectious disease that spread rapidly and involved objective risk of death. The retrospective assessment of the sequence […]See moreViews1Summary
EditorialGynecologists and Obstetricians Working Group to Face the COVID-19 Pandemic in Brazil: Successful Experience to be Followed
Rev Bras Ginecol Obstet. 2021;43(8):585-587
Views1In addition to causing relevant changes in the global routine, the COVID-19 pandemic status announced and recognized by the World Health Organization (WHO) on March 11, 2020, made it clear that no country was ready to face an infectious disease that spread rapidly and involved objective risk of death. The retrospective assessment of the sequence […]See more -
Letter to the Editor
Reply to: Zika Virus Infection, Pregnancy and Microcephaly
Rev Bras Ginecol Obstet. 2018;40(1):54-55
Summary
Letter to the EditorReply to: Zika Virus Infection, Pregnancy and Microcephaly
Rev Bras Ginecol Obstet. 2018;40(1):54-55
Views3Dear Editor,I would like to thank Dr. Sriwijitalai & Wiwanitkit for the letter to the editor about our article on the care of pregnant women at the time of the zika virus infection. I would also like to thank you for the opportunity to clarify some of the topics they have mentioned.[…]See moreViews3Summary
Letter to the EditorReply to: Zika Virus Infection, Pregnancy and Microcephaly
Rev Bras Ginecol Obstet. 2018;40(1):54-55
Views3Dear Editor,I would like to thank Dr. Sriwijitalai & Wiwanitkit for the letter to the editor about our article on the care of pregnant women at the time of the zika virus infection. I would also like to thank you for the opportunity to clarify some of the topics they have mentioned.[…]See more -
Systematic Review
Zika Virus Infection in Pregnant Women and Microcephaly
Rev Bras Ginecol Obstet. 2017;39(5):235-248
Summary
Systematic ReviewZika Virus Infection in Pregnant Women and Microcephaly
Rev Bras Ginecol Obstet. 2017;39(5):235-248
Views0Abstract
From the discovery of the Zika virus (ZIKV) in 1947 in Uganda (Africa), until its arrival in South America, it was not known that it would affect human reproductive life so severely. Today, damagetothe central nervous system is known to be multiple, and microcephaly is considered the tip of the iceberg. Microcephaly actually represents the epilogue of this infection’s devastating process on the central nervous system of embryos and fetuses. As a result of central nervous system aggression by the ZIKV, this infection brings the possibility of arthrogryposis, dysphagia, deafness and visual impairment. All of these changes of varying severity directly or indirectly compromise the future life of these children, and are already considered a congenital syndrome linked to the ZIKV. Diagnosis is one of the main difficulties in the approach of this infection. Considering the clinical part, it has manifestations common to infections by the dengue virus and the chikungunya fever, varying only in subjective intensities. The most frequent clinical variables are rash, febrile state, non-purulent conjunctivitis and arthralgia, among others. In terms of laboratory resources, there are also limitations to the subsidiary diagnosis. Molecular biology tests are based on polymerase chain reaction (PCR)with reverse transcriptase (RT) action, since the ZIKV is a ribonucleic acid (RNA) virus. The RT-PCR shows serum or plasma positivity for a short period of time, no more than five days after the onset of the signs and symptoms. The ZIKVurine test is positive for a longer period, up to 14 days. There are still no reliable techniques for the serological diagnosis of this infection. If there are no complications (meningoencephalitis or Guillain-Barré syndrome), further examination is unnecessary to assess systemic impairment. However, evidence is needed to rule out other infections that also cause rashes, such as dengue, chikungunya, syphilis, toxoplasmosis, cytomegalovirus, rubella, and herpes. There is no specific antiviral therapy against ZIKV, and the therapeutic approach to infected pregnant women is limited to the use of antipyretics and analgesics. Anti-inflammatory drugs should be avoided until the diagnosis of dengue is discarded. There is no need to modify the schedule of prenatal visits for pregnant women infected by ZIKV, but it is necessary to guarantee three ultrasound examinations during pregnancy for low-risk pregnancies, and monthly for pregnant women with confirmed ZIKV infection. Vaginal delivery and natural breastfeeding are advised.
Key-words arbovirus infectionsblindness/ etiologydeafness/ etiologymicrocephaly/ ultrasonographyPregnancy complicationsreal-time polymerase chain reactionZika virusSee moreViews0Summary
Systematic ReviewZika Virus Infection in Pregnant Women and Microcephaly
Rev Bras Ginecol Obstet. 2017;39(5):235-248
Views0Abstract
From the discovery of the Zika virus (ZIKV) in 1947 in Uganda (Africa), until its arrival in South America, it was not known that it would affect human reproductive life so severely. Today, damagetothe central nervous system is known to be multiple, and microcephaly is considered the tip of the iceberg. Microcephaly actually represents the epilogue of this infection’s devastating process on the central nervous system of embryos and fetuses. As a result of central nervous system aggression by the ZIKV, this infection brings the possibility of arthrogryposis, dysphagia, deafness and visual impairment. All of these changes of varying severity directly or indirectly compromise the future life of these children, and are already considered a congenital syndrome linked to the ZIKV. Diagnosis is one of the main difficulties in the approach of this infection. Considering the clinical part, it has manifestations common to infections by the dengue virus and the chikungunya fever, varying only in subjective intensities. The most frequent clinical variables are rash, febrile state, non-purulent conjunctivitis and arthralgia, among others. In terms of laboratory resources, there are also limitations to the subsidiary diagnosis. Molecular biology tests are based on polymerase chain reaction (PCR)with reverse transcriptase (RT) action, since the ZIKV is a ribonucleic acid (RNA) virus. The RT-PCR shows serum or plasma positivity for a short period of time, no more than five days after the onset of the signs and symptoms. The ZIKVurine test is positive for a longer period, up to 14 days. There are still no reliable techniques for the serological diagnosis of this infection. If there are no complications (meningoencephalitis or Guillain-Barré syndrome), further examination is unnecessary to assess systemic impairment. However, evidence is needed to rule out other infections that also cause rashes, such as dengue, chikungunya, syphilis, toxoplasmosis, cytomegalovirus, rubella, and herpes. There is no specific antiviral therapy against ZIKV, and the therapeutic approach to infected pregnant women is limited to the use of antipyretics and analgesics. Anti-inflammatory drugs should be avoided until the diagnosis of dengue is discarded. There is no need to modify the schedule of prenatal visits for pregnant women infected by ZIKV, but it is necessary to guarantee three ultrasound examinations during pregnancy for low-risk pregnancies, and monthly for pregnant women with confirmed ZIKV infection. Vaginal delivery and natural breastfeeding are advised.
Key-words arbovirus infectionsblindness/ etiologydeafness/ etiologymicrocephaly/ ultrasonographyPregnancy complicationsreal-time polymerase chain reactionZika virusSee more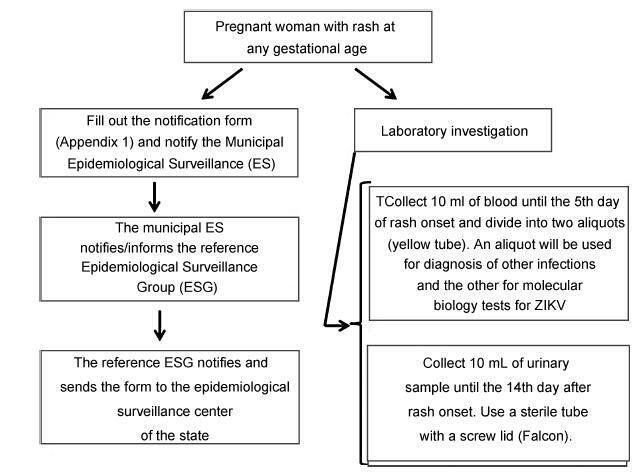
Search
Search in:
Tag Cloud
breast (42) breast cancer (42) breast neoplasms (95) Cesarean section (72) endometriosis (66) infertility (56) Maternal mortality (43) menopause (82) obesity (58) postpartum period (40) pregnancy (225) Pregnancy complications (99) Prenatal care (68) prenatal diagnosis (50) Prevalence (41) Quality of life (51) risk factors (94) ultrasonography (79) urinary incontinence (40) women's health (48)