Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):569-574
DOI 10.1590/SO100-720320140005068
The aim of this study was to evaluate the clinical features and prognostic implications of patients with recurrent cervical cancer.
By reviewing the medical records we evaluated all patients with cervical cancer at stages IA to IVA who started treatment at a specialized hospital in the Southeast region of Brazil from 2007 to 2009. Recurrence episodes were categorized according to location of disease and information was collected regarding the type of treatment and survival of these patients. The sample was characterized by descriptive statistics and association analyses were performed using Fisher's exact test.
Fifty cases of recurrence were identified among 469 selected records, with 31 patients being symptomatic at diagnosis of recurrence (62%); and 19 being asymptomatic (38%). Among women with symptoms, eight requested anticipation of the previously scheduled appointment because of the presence of clinical complaints. Patients with symptoms at the diagnosis of recurrence had lower rates of overall two-year survival (39.4 versus 67.6%) (p=0.081). None of the patients with recurrence at distance received curative intent treatment, but all received surgical treatment or radiotherapy aiming at full remission of the disease. Women who requested anticipation of the appointment because of the presence of symptoms had a significant reduction of overall two-year survival after recurrence (0 versus 60.4%; p<0.001) compared to those who attended the consultation on the scheduled date, and none of them received curative intent treatment. As expected, the patients who underwent palliative treatment with the main objective of improving quality of life and increasing survival but with no perspective of cure had a significant reduction in overall survival compared to those who were treated with curative intent (76.7 versus 35.4%; p<0.001).
The benefit of detecting asymptomatic recurrence of cervical cancer has the potential to improve the prognosis of patients with local and regional recurrence, but studies on larger series are necessary to confirm this possibility.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):569-574
DOI 10.1590/SO100-720320140005068
The aim of this study was to evaluate the clinical features and prognostic implications of patients with recurrent cervical cancer.
By reviewing the medical records we evaluated all patients with cervical cancer at stages IA to IVA who started treatment at a specialized hospital in the Southeast region of Brazil from 2007 to 2009. Recurrence episodes were categorized according to location of disease and information was collected regarding the type of treatment and survival of these patients. The sample was characterized by descriptive statistics and association analyses were performed using Fisher's exact test.
Fifty cases of recurrence were identified among 469 selected records, with 31 patients being symptomatic at diagnosis of recurrence (62%); and 19 being asymptomatic (38%). Among women with symptoms, eight requested anticipation of the previously scheduled appointment because of the presence of clinical complaints. Patients with symptoms at the diagnosis of recurrence had lower rates of overall two-year survival (39.4 versus 67.6%) (p=0.081). None of the patients with recurrence at distance received curative intent treatment, but all received surgical treatment or radiotherapy aiming at full remission of the disease. Women who requested anticipation of the appointment because of the presence of symptoms had a significant reduction of overall two-year survival after recurrence (0 versus 60.4%; p<0.001) compared to those who attended the consultation on the scheduled date, and none of them received curative intent treatment. As expected, the patients who underwent palliative treatment with the main objective of improving quality of life and increasing survival but with no perspective of cure had a significant reduction in overall survival compared to those who were treated with curative intent (76.7 versus 35.4%; p<0.001).
The benefit of detecting asymptomatic recurrence of cervical cancer has the potential to improve the prognosis of patients with local and regional recurrence, but studies on larger series are necessary to confirm this possibility.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):575-580
DOI 10.1590/SO100-720320140005158
To compare the distributions of patients with clinical-pathological subtypes of luminal B-like breast cancer according to the 2011 and 2013 St. Gallen International Breast Cancer Conference Expert Panel.
We studied 142 women with breast cancer who were positive to estrogen receptor and had been treated in São Paulo state, southeast Brazil. The expression of the following receptors was assessed by immunohistochemistry: estrogen, progesterone (PR) and Ki-67. The expression of HER-2 was measured by fluorescent in situ hybridization analysis in tissue microarray.
There were 29 cases of luminal A breast cancers according to the 2011 St. Gallen International Breast Cancer Conference Expert Panel that were classified as luminal B-like in the 2013 version. Among the 65 luminal B-like breast cancer cases, 29 (45%) were previous luminal A tumors, 15 cases (20%) had a Ki-67 >14% and were at least 20% PR positive and 21 cases (35%) had Ki-67 >14% and more than 20% were PR positive.
The 2013 St. Gallen consensus updated the definition of intrinsic molecular subtypes and increased the number of patients classified as having luminal B-like breast cancer in our series, for whom the use of cytotoxic drugs will probably be proposed with additional treatment cost.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):575-580
DOI 10.1590/SO100-720320140005158
To compare the distributions of patients with clinical-pathological subtypes of luminal B-like breast cancer according to the 2011 and 2013 St. Gallen International Breast Cancer Conference Expert Panel.
We studied 142 women with breast cancer who were positive to estrogen receptor and had been treated in São Paulo state, southeast Brazil. The expression of the following receptors was assessed by immunohistochemistry: estrogen, progesterone (PR) and Ki-67. The expression of HER-2 was measured by fluorescent in situ hybridization analysis in tissue microarray.
There were 29 cases of luminal A breast cancers according to the 2011 St. Gallen International Breast Cancer Conference Expert Panel that were classified as luminal B-like in the 2013 version. Among the 65 luminal B-like breast cancer cases, 29 (45%) were previous luminal A tumors, 15 cases (20%) had a Ki-67 >14% and were at least 20% PR positive and 21 cases (35%) had Ki-67 >14% and more than 20% were PR positive.
The 2013 St. Gallen consensus updated the definition of intrinsic molecular subtypes and increased the number of patients classified as having luminal B-like breast cancer in our series, for whom the use of cytotoxic drugs will probably be proposed with additional treatment cost.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):562-568
DOI 10.1590/SO100-720320140005161
To verify the existence of associations between different maternal ages and the perinatal outcomes of preterm birth and intrauterine growth restriction in the city of São Luís, Maranhão, Northeastern Brazil.
A cross-sectional study using a sample of 5,063 hospital births was conducted in São Luís, from January to December 2010. The participants comprise the birth cohort for the study "Etiological factors of preterm birth and consequences of perinatal factors for infant health: birth cohorts from two Brazilian cities" (BRISA). Frequencies and 95% confidence intervals were used to describe the results. Multiple logistic regression models were applied to assess the adjusted odds ratio (OR) of maternal age associated with the following outcomes: preterm birth and intrauterine growth restriction.
The percentage of early teenage pregnancy (12–15 years old) was 2.2%, and of late (16–19 years old) was 16.4%, while pregnancy at an advanced maternal age (>35 years) was 5.9%. Multivariate analyses showed a statistically significant increase in preterm births among females aged 12–15 years old (OR=1.6; p=0.04) compared with those aged 20–35 years. There was also a higher rate in preterm births among females aged 16–19 years old (OR=1.3; p=0.01). Among those with advanced maternal age (>35 years old), the increase in the prevalence of preterm birth had only borderline statistical significance (OR=1.4; p=0.05). There was no statistically significant association between maternal age and increased prevalence of intrauterine growth restriction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(12):562-568
DOI 10.1590/SO100-720320140005161
To verify the existence of associations between different maternal ages and the perinatal outcomes of preterm birth and intrauterine growth restriction in the city of São Luís, Maranhão, Northeastern Brazil.
A cross-sectional study using a sample of 5,063 hospital births was conducted in São Luís, from January to December 2010. The participants comprise the birth cohort for the study "Etiological factors of preterm birth and consequences of perinatal factors for infant health: birth cohorts from two Brazilian cities" (BRISA). Frequencies and 95% confidence intervals were used to describe the results. Multiple logistic regression models were applied to assess the adjusted odds ratio (OR) of maternal age associated with the following outcomes: preterm birth and intrauterine growth restriction.
The percentage of early teenage pregnancy (12–15 years old) was 2.2%, and of late (16–19 years old) was 16.4%, while pregnancy at an advanced maternal age (>35 years) was 5.9%. Multivariate analyses showed a statistically significant increase in preterm births among females aged 12–15 years old (OR=1.6; p=0.04) compared with those aged 20–35 years. There was also a higher rate in preterm births among females aged 16–19 years old (OR=1.3; p=0.01). Among those with advanced maternal age (>35 years old), the increase in the prevalence of preterm birth had only borderline statistical significance (OR=1.4; p=0.05). There was no statistically significant association between maternal age and increased prevalence of intrauterine growth restriction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):489-496
DOI 10.1590/S0100-720320140005090
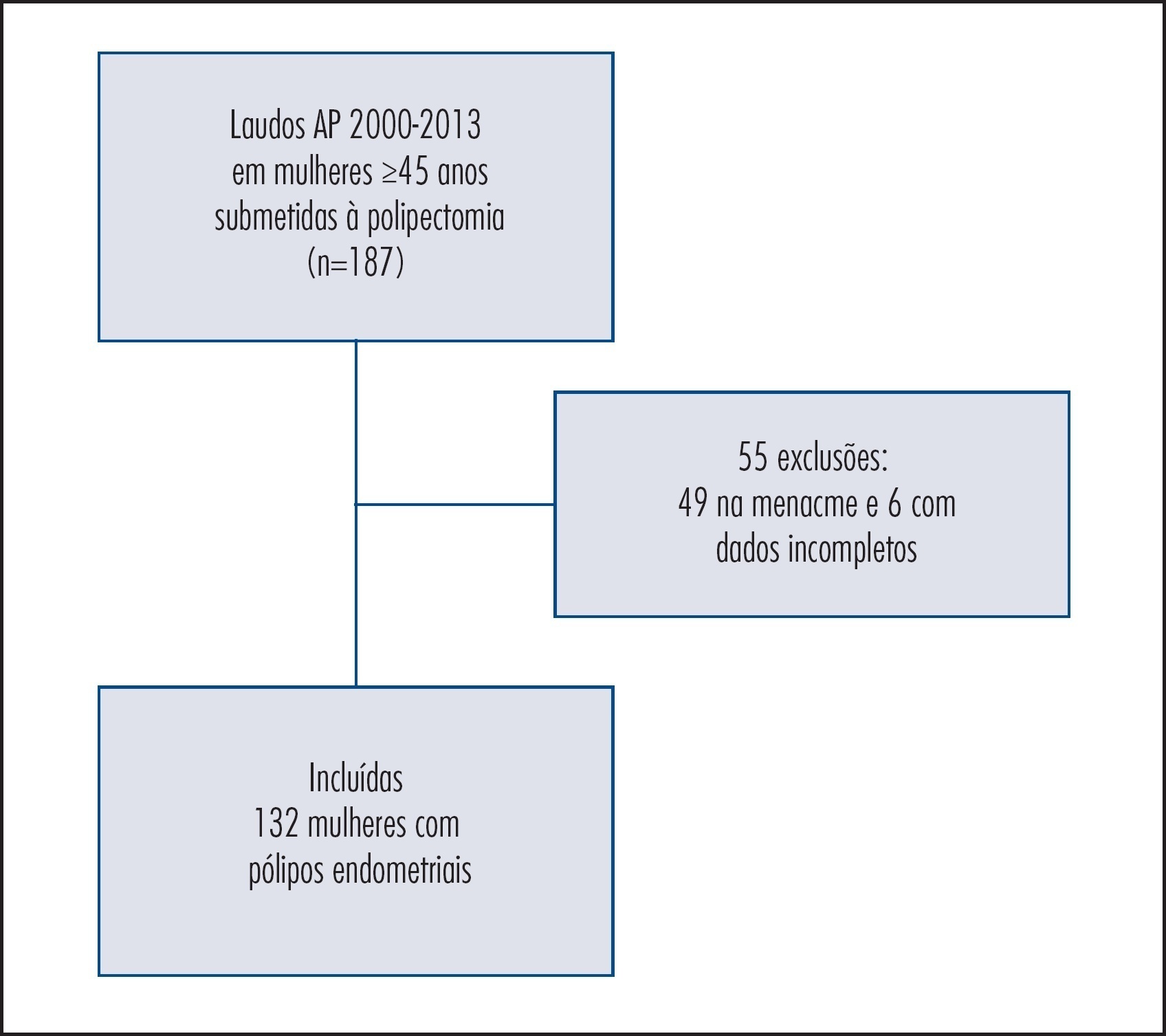
To evaluate the predictive clinical factors for the development of endometrial polyps in postmenopausal women.
Observational cohort study with postmenopausal women who had been at a public university hospital. Clinical, anthropometrical, laboratorial, and ultrasonographic data of 132 patients with a histopathological diagnosis of endometrial polyps and 264 women without endometrial alterations (control) were compared in order to evaluate the predictive factors of endometrial polyps. Women with amenorrhea ≥12 months and ≥45 years of age were included in the study at a proportion of 1 case for 2 controls. The Student's t, χ2, and logistic regression tests were used for statistical analysis – odds ratio (OR).
Patients with endometrial polyps were older and had been in menopause for a longer time compared to control (p<0.0001). The percentage of obese women with polyps (72.0%) was higher compared to the Control Group (39%; p<0.0001). The measurement of waist circumference was superior among patients with polyps (p=0.0001). We observed a higher incidence of diabetes, hypertension and dyslipidemia in patients with endometrial polyps (p<0.0001). According to the US National Cholesterol Education Program/Adult Treatment Panel III (NCEP/ATP III) criteria, 48.5% of women with polyps and 33.3% of the Control Group were classified as having metabolic syndrome (p=0.004). Analysis of risk for endometrial polyps formation showed higher chances of occurrence of the disorder in patients with: BMI≥25 kg/m2 (OR=4.6; 95%CI 2.1–10.0); glucose ≥100 mg/dL (OR=2.8; 95%CI 1.3–5.9); dyslipidemia (OR=7.0; 95%CI 3.7–13.3); diabetes (OR=2.5; 95%CI 1.0–6.3), and metabolic syndrome (OR=2.7; 95%CI 1.1–6.4) compared to the Control Group.
In postmenopausal women, obesity, dyslipidemia, hyperglycemia and presence of metabolic syndrome were predictive factors for the development of endometrial polyps.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):489-496
DOI 10.1590/S0100-720320140005090
To evaluate the predictive clinical factors for the development of endometrial polyps in postmenopausal women.
Observational cohort study with postmenopausal women who had been at a public university hospital. Clinical, anthropometrical, laboratorial, and ultrasonographic data of 132 patients with a histopathological diagnosis of endometrial polyps and 264 women without endometrial alterations (control) were compared in order to evaluate the predictive factors of endometrial polyps. Women with amenorrhea ≥12 months and ≥45 years of age were included in the study at a proportion of 1 case for 2 controls. The Student's t, χ2, and logistic regression tests were used for statistical analysis – odds ratio (OR).
Patients with endometrial polyps were older and had been in menopause for a longer time compared to control (p<0.0001). The percentage of obese women with polyps (72.0%) was higher compared to the Control Group (39%; p<0.0001). The measurement of waist circumference was superior among patients with polyps (p=0.0001). We observed a higher incidence of diabetes, hypertension and dyslipidemia in patients with endometrial polyps (p<0.0001). According to the US National Cholesterol Education Program/Adult Treatment Panel III (NCEP/ATP III) criteria, 48.5% of women with polyps and 33.3% of the Control Group were classified as having metabolic syndrome (p=0.004). Analysis of risk for endometrial polyps formation showed higher chances of occurrence of the disorder in patients with: BMI≥25 kg/m2 (OR=4.6; 95%CI 2.1–10.0); glucose ≥100 mg/dL (OR=2.8; 95%CI 1.3–5.9); dyslipidemia (OR=7.0; 95%CI 3.7–13.3); diabetes (OR=2.5; 95%CI 1.0–6.3), and metabolic syndrome (OR=2.7; 95%CI 1.1–6.4) compared to the Control Group.
In postmenopausal women, obesity, dyslipidemia, hyperglycemia and presence of metabolic syndrome were predictive factors for the development of endometrial polyps.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):497-502
DOI 10.1590/S0100-720320140004985
To evaluate the sexual function and factors associated with sexual dysfunction in climacteric women.
A cross-sectional study was conducted on 173 women aged 35 to 65 years old, with a steady partner during the last 6 months, who are literate, without cognitive impairment, and with sexual activity for at least 6 months. The instrument used to assess sexual performance was the Sexual Quotient, female version. The association between sexual dysfunction and sociodemographic data, personal, obstetric and sexual history was determined by Pearson's χ2 test and strength of association by the odds ratio (OR) with a 95% confidence interval (95%CI).
In this study, 46.2% of the women reported sexual dysfunction. There was a decrease in the chance of sexual dysfunction for the age group between 35 and 49 years old (OR=0.3; 95%CI 0.2–0.6) and for women who felt comfortable talking about sex (OR=0.5; 95%CI 0.2–0.8). However, the presence of osteoporosis (OR=3.3; 95%CI 1.5–7.6), urinary incontinence (OR=2.0; 95%CI 1.1–3.7), and surgical corrections of the pelvic floor (OR=2.2; 95%CI 1.1–4.5) increased this chance.
The frequency of sexual dysfunction in women aged 35 to 65 years old was 46.2% and factors such as osteoporosis, urinary incontinence and surgical corrections of the pelvic floor increased the chance of sexual dysfunction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):497-502
DOI 10.1590/S0100-720320140004985
To evaluate the sexual function and factors associated with sexual dysfunction in climacteric women.
A cross-sectional study was conducted on 173 women aged 35 to 65 years old, with a steady partner during the last 6 months, who are literate, without cognitive impairment, and with sexual activity for at least 6 months. The instrument used to assess sexual performance was the Sexual Quotient, female version. The association between sexual dysfunction and sociodemographic data, personal, obstetric and sexual history was determined by Pearson's χ2 test and strength of association by the odds ratio (OR) with a 95% confidence interval (95%CI).
In this study, 46.2% of the women reported sexual dysfunction. There was a decrease in the chance of sexual dysfunction for the age group between 35 and 49 years old (OR=0.3; 95%CI 0.2–0.6) and for women who felt comfortable talking about sex (OR=0.5; 95%CI 0.2–0.8). However, the presence of osteoporosis (OR=3.3; 95%CI 1.5–7.6), urinary incontinence (OR=2.0; 95%CI 1.1–3.7), and surgical corrections of the pelvic floor (OR=2.2; 95%CI 1.1–4.5) increased this chance.
The frequency of sexual dysfunction in women aged 35 to 65 years old was 46.2% and factors such as osteoporosis, urinary incontinence and surgical corrections of the pelvic floor increased the chance of sexual dysfunction.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):503-508
DOI 10.1590/S0100-720320140005081
To evaluate variations in the body mass index in patients undergoing adjuvant chemotherapy for breast cancer, and to associate these changes with patient's age and adjuvant chemotherapy regimen.
We performed a retrospective cohort study in order to correlate any variation in the body mass index before and after adjuvant chemotherapy with patient's age and adjuvant chemotherapy regimen. Patients who received any form of prior hormone therapy, such as tamoxifen or aromatase inhibitors, were excluded. We selected data for 196 patients with stage I to III breast cancer who were treated by radical or conservative surgery and received adjuvant chemotherapy at the Cancer Institute of the State of São Paulo, Brazil.
Before adjuvant chemotherapy, 67.8% of patients were classified as overweight or obese according to their body mass indices. Around 66.3% (95% CI 59.7–73.0) of the patients exhibited an increase in the body mass index after adjuvant chemotherapy. The average age of all patients was 56.3±11.3 years. Participants whose body mass index increased were younger than those with no increase (54.7±11.1 versus 59.3±11.2 years; p=0.007). Patients were treated with the following adjuvant chemotherapy regimens: doxorubicin, cyclophosphamide, and paclitaxel (AC-T, 129 patients, 65.8%); 5-fluoracil, doxorubicin, and cyclophosphamide (36 patients, 18.4%); cyclophosphamide, methotrexate, and 5-fluoracil (16 patients, 8.2%); docetaxel and cyclophosphamide (7 patients, 3.6%); and other regimen (8 patients, 4.1%). The AC-T regimen showed a statistically significant association with increase in the body mass index (p<0.001 by ANOVA).
Most patients with breast cancer showed an increase in the body mass index after adjuvant chemotherapy, especially after the AC-T chemotherapy regimen.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):503-508
DOI 10.1590/S0100-720320140005081
To evaluate variations in the body mass index in patients undergoing adjuvant chemotherapy for breast cancer, and to associate these changes with patient's age and adjuvant chemotherapy regimen.
We performed a retrospective cohort study in order to correlate any variation in the body mass index before and after adjuvant chemotherapy with patient's age and adjuvant chemotherapy regimen. Patients who received any form of prior hormone therapy, such as tamoxifen or aromatase inhibitors, were excluded. We selected data for 196 patients with stage I to III breast cancer who were treated by radical or conservative surgery and received adjuvant chemotherapy at the Cancer Institute of the State of São Paulo, Brazil.
Before adjuvant chemotherapy, 67.8% of patients were classified as overweight or obese according to their body mass indices. Around 66.3% (95% CI 59.7–73.0) of the patients exhibited an increase in the body mass index after adjuvant chemotherapy. The average age of all patients was 56.3±11.3 years. Participants whose body mass index increased were younger than those with no increase (54.7±11.1 versus 59.3±11.2 years; p=0.007). Patients were treated with the following adjuvant chemotherapy regimens: doxorubicin, cyclophosphamide, and paclitaxel (AC-T, 129 patients, 65.8%); 5-fluoracil, doxorubicin, and cyclophosphamide (36 patients, 18.4%); cyclophosphamide, methotrexate, and 5-fluoracil (16 patients, 8.2%); docetaxel and cyclophosphamide (7 patients, 3.6%); and other regimen (8 patients, 4.1%). The AC-T regimen showed a statistically significant association with increase in the body mass index (p<0.001 by ANOVA).
Most patients with breast cancer showed an increase in the body mass index after adjuvant chemotherapy, especially after the AC-T chemotherapy regimen.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):509-513
DOI 10.1590/S0100-720320140005024
To evaluate the influence of maternal obesity on pregnancy, childbirth, and neonatal outcomes.
A cross-sectional study with 298 postpartum women. Information was obtained through interviews and access to patients' medical records. The patients were divided into three groups according to their pre-gestational body mass index: normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2). Data are reported as adjusted odds ratios with 95% confidence interval (95%CI) following multinomial logistic regression analysis to account for confounding variables.
Compared to pregnant women with normal body mass index, overweight women had greater chances of having cesarean delivery, odds ratio (OR) of 2.2 and 95%CI 1.3–3.9, and obese women even more (OR=4.2; 95%CI 2.1–8.1). The chances of gestational diabetes increased in the Overweight (OR=2.5; 95%CI 1.1–5.6) and Obese groups (OR=11.1; 95%CI 5.0–24.6). The occurrence of hypertensive syndrome was also higher in overweight (OR=3.2; 95%CI 1.2–8.1) and obese pregnant women (OR=7.5; 95%CI 2.9–19.1). Major postpartum hemorrhage only showed greater values in the obese women group (OR=4.1; 95%CI 1.1–15.8). Regarding the newborns, the probability of a low Apgar score at first minute was higher in the Obese Group (OR=5.5; 95%CI 1.2–23.7) and chances of macrosomia were higher in the Overweight Group (OR=2.9; 95%CI 1.3–6.3). Data regarding neonatal hypoglycemia were not conclusive.
Excessive weight (overweight and obesity) during pregnancy increases the chance of maternal complications (gestational diabetes, hypertensive syndrome, and major postpartum hemorrhage) and neonatal outcomes (cesarean delivery, macrosomia, and low Apgar score).
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):509-513
DOI 10.1590/S0100-720320140005024
To evaluate the influence of maternal obesity on pregnancy, childbirth, and neonatal outcomes.
A cross-sectional study with 298 postpartum women. Information was obtained through interviews and access to patients' medical records. The patients were divided into three groups according to their pre-gestational body mass index: normal weight (18.5–24.9 kg/m2), overweight (25.0–29.9 kg/m2), and obese (≥30.0 kg/m2). Data are reported as adjusted odds ratios with 95% confidence interval (95%CI) following multinomial logistic regression analysis to account for confounding variables.
Compared to pregnant women with normal body mass index, overweight women had greater chances of having cesarean delivery, odds ratio (OR) of 2.2 and 95%CI 1.3–3.9, and obese women even more (OR=4.2; 95%CI 2.1–8.1). The chances of gestational diabetes increased in the Overweight (OR=2.5; 95%CI 1.1–5.6) and Obese groups (OR=11.1; 95%CI 5.0–24.6). The occurrence of hypertensive syndrome was also higher in overweight (OR=3.2; 95%CI 1.2–8.1) and obese pregnant women (OR=7.5; 95%CI 2.9–19.1). Major postpartum hemorrhage only showed greater values in the obese women group (OR=4.1; 95%CI 1.1–15.8). Regarding the newborns, the probability of a low Apgar score at first minute was higher in the Obese Group (OR=5.5; 95%CI 1.2–23.7) and chances of macrosomia were higher in the Overweight Group (OR=2.9; 95%CI 1.3–6.3). Data regarding neonatal hypoglycemia were not conclusive.
Excessive weight (overweight and obesity) during pregnancy increases the chance of maternal complications (gestational diabetes, hypertensive syndrome, and major postpartum hemorrhage) and neonatal outcomes (cesarean delivery, macrosomia, and low Apgar score).
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):514-518
DOI 10.1590/S0100-720320140005007
To describe the epidemiologic and obstetric characteristics of women with recurrent miscarriages.
A descriptive and analytical study whose inclusion criterion was every woman that was attended at the clinic for recurrent miscarriage (loss group), between January 2006 and December 2010. Patients that did not live in Salvador, Bahia, Brazil, and those who were not reached by telephone or whose number was not included in the medical record were not included. The Control Group consisted of 204 pregnant women seen at the low-risk prenatal care unit between May 2007 and April 2008. Women who did not accept to be interviewed and those with obstetric risk were excluded from the Control Group. The analyzed variables were: age, education, occupation, marital status, alcohol consumption, body mass index, obstetric history and the gestational age when the losses occurred. The SPSS 18.0 program was used for statistical analysis. Means and standard deviations of continuous variables were compared using the Student's t-test and the frequencies of the nominal variables were compared by the χ2 test.
The mean age of women in the loss group was higher than in the Control Group (32.3±6.3 versus 26.5±6.4 years old, p<0.01). Consumption of alcoholic beverages predominated in the loss group (36.9 versus 22.1%, p=0.01), as well as marital status (93.2 versus 66.7% were married or living in a stable union, p<0.01). The pre-pregnancy body mass index was higher in the loss group (26.9 versus 23.5%, p<0.01). Regarding obstetric history, 103 women with recurrent miscarriage reported 334 pregnancies. Fifty-six of them had 2 or more miscarriages in the first quarter and in 31 of them, 2 or more pregnancies progressed to late abortions/extremely preterm infants.
Some risk factors were identified in women with recurrent losses, such as more advanced age and higher body mass index. These observations agree with more recent proposals regarding recurrent losses that consider the inclusion of losses in various gestational ages.
Summary
Revista Brasileira de Ginecologia e Obstetrícia. 2014;36(11):514-518
DOI 10.1590/S0100-720320140005007
To describe the epidemiologic and obstetric characteristics of women with recurrent miscarriages.
A descriptive and analytical study whose inclusion criterion was every woman that was attended at the clinic for recurrent miscarriage (loss group), between January 2006 and December 2010. Patients that did not live in Salvador, Bahia, Brazil, and those who were not reached by telephone or whose number was not included in the medical record were not included. The Control Group consisted of 204 pregnant women seen at the low-risk prenatal care unit between May 2007 and April 2008. Women who did not accept to be interviewed and those with obstetric risk were excluded from the Control Group. The analyzed variables were: age, education, occupation, marital status, alcohol consumption, body mass index, obstetric history and the gestational age when the losses occurred. The SPSS 18.0 program was used for statistical analysis. Means and standard deviations of continuous variables were compared using the Student's t-test and the frequencies of the nominal variables were compared by the χ2 test.
The mean age of women in the loss group was higher than in the Control Group (32.3±6.3 versus 26.5±6.4 years old, p<0.01). Consumption of alcoholic beverages predominated in the loss group (36.9 versus 22.1%, p=0.01), as well as marital status (93.2 versus 66.7% were married or living in a stable union, p<0.01). The pre-pregnancy body mass index was higher in the loss group (26.9 versus 23.5%, p<0.01). Regarding obstetric history, 103 women with recurrent miscarriage reported 334 pregnancies. Fifty-six of them had 2 or more miscarriages in the first quarter and in 31 of them, 2 or more pregnancies progressed to late abortions/extremely preterm infants.
Some risk factors were identified in women with recurrent losses, such as more advanced age and higher body mass index. These observations agree with more recent proposals regarding recurrent losses that consider the inclusion of losses in various gestational ages.